Article Text

Statistics from Altmetric.com
Finland, like many other western countries, has experienced profound structural changes during the post-war period: urbanisation, increasing education, smaller family size, improved hygiene for food and household water, and prophylaxis and effective care of many potentially dangerous infectious diseases. Many of these factors have been associated with the increased risk for asthma and allergies1 which has also been found in Finland.2
In 1993 the Ministry of Social Affairs and Health in Finland recognised asthma as an important public health issue by appointing a working group to design a national programme for the prevention and alleviation of problems caused by asthma and for reduction of the relevant costs. The group decided to create an action programme emphasising guideline implementation and follow up, which are often neglected in consensus reports on asthma treatment. The 10 year programme was launched in 1994.3 The goals of prevention and treatment were stated as follows: (1) recovery of as many patients as possible with early asthma; (2) asthmatic patients should feel well and their ability for work and functional capacity should correspond with their age; (3) decline in the percentage of patients with severe and moderate asthma from the current 40% to 20%; (4) decrease in the number of bed days of asthmatic patients by 50% by the year 2000 (that is, to 50 000 a year); and (5) reduction in the annual treatment costs per patient by 50% as a result of more effective prevention and treatment of symptoms.
The measures towards achieving the goals were as follows: (1) early diagnosis and active treatment; (2) guided self-management as the primary form of treatment; (3) decrease in respiratory irritants such as smoking and tobacco smoke; (4) implementation of rehabilitation on an outpatient basis combined with normal treatment, planned individually and timed appropriately; (5) increase in knowledge about asthma in key groups; and (6) promotion of scientific research.
The present paper evaluates the programme at the end of 2000. It gives the Finnish perspective to the development of the morbidity and describes a comprehensive approach to decrease the impact of asthma to individuals as well as to society.
From pathophysiology to intervention
In 1994 the widely held dogma was: “Once asthma always asthma, it cannot be cured but only controlled”. The working group based its actions on a more optimistic view: (1) most patients have, in fact, a mild type of disease; (2) inflammation of the bronchial mucosa and lung function abnormalities can be detected early; and (3) early intervention often leads to complete recovery, although disposition to asthmatic reactions remains.
These claims were based on a series of studies which started in the early 1980s by taking fresh biopsy specimens with a rigid tube bronchoscope from eight asthmatic subjects (two mild, three moderate, three severe). All of them showed a more or less damaged epithelium compared with a control subject.4 The most striking observation was that epithelial changes (and influx of inflammatory cells in lamina propria, not commented on in the original paper) also existed in the two mild untreated patients with duration of symptoms of only a few months. This observation led to the idea of anti-inflammatory medication as first line therapy.
To prove the inflammation hypothesis a 3 year intervention study was started.5-7 The results had important clinical implications: (1) early anti-inflammatory treatment with an inhaled steroid causes full clinical and functional remission in most patients with asthma of short duration; (2) maintenance treatment can usually be given at a reduced dose of steroid; and (3) delays in initiating steroid treatment may lead to an impaired clinical and functional response.
The next step was to explore possibilities of guided self-management plans to optimise disease control. It was shown that exacerbations and asthma events can be significantly reduced by educating patients with persistent asthma to adjust their anti-inflammatory treatment according to home monitoring of peak expiratory flow (PEF).8 This also led to reduced health care costs.9
It was also assumed that early detection and treatment of the asthmatic inflammation, when the functional disturbance is mild or just developing, may even prevent overt asthma. However, improved diagnostic tools were needed and the method for induced sputum10 ,11was used in various clinical settings.12 ,13
In an extensive review Bousquet et al 14 have recently described the development of our understanding of asthma and have highlighted the concept of airway remodelling which may be confusing as a definition but is important in the pathogenesis of asthma. The somewhat mechanistic idea of asthma as enhanced bronchospasm has been replaced by a more holistic view regarding asthma as a biological continuum from occasional symptoms to irreversible airway structural changes causing a chronic need for treatment.
Understanding asthma as a fundamentally inflammatory disorder which can be detected early and treated effectively was the basic idea on which the Finnish action programme was formulated.
Working strategy and implementation
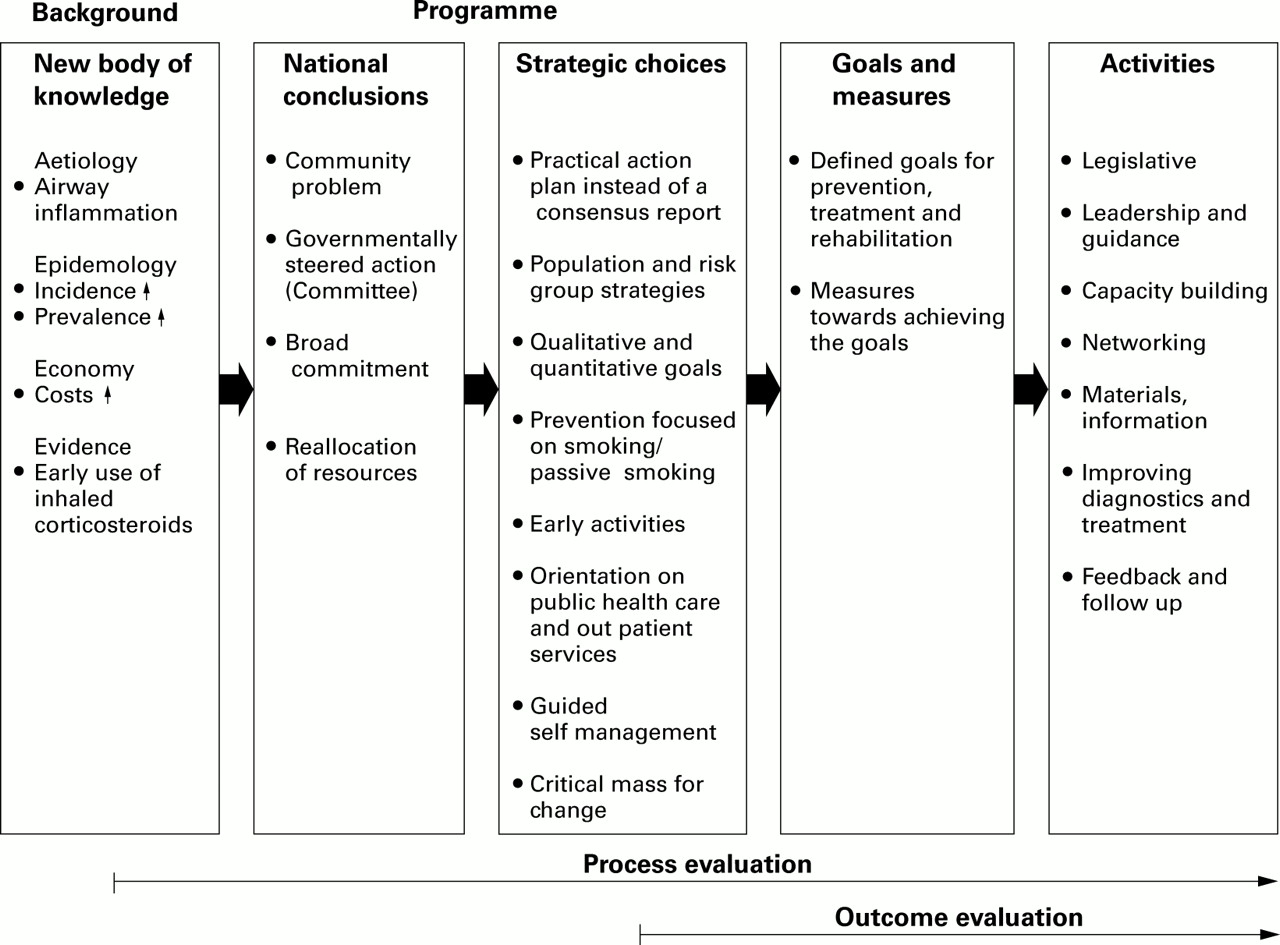
The strategic planning of the programme is outlined in the flow chart in fig 1. The national acts were based on a new body of medical knowledge. Asthma was recognised for the first time as a community problem so, to achieve a broad commitment and reallocation of resources, governmentally steered action was needed. The steering committee decided the strategic choices, set goals and measures, and agreed upon activities which were considered to have the best impact (see box 1). Process and outcome evaluation was also planned.
Legislation
Revised anti-smoking legislation 1995, 2000
Outdoor (1996), indoor (1997) air regulations, Ministry of Social Affairs and Health
Modified drug reimbursement regulations
Leadership, guidance, advocacy
National Asthma Follow up Group
Focal point: The Finnish Lung Health Association
Regional asthma contact specialists (n=31)
Capacity building
Further training: national, regional, local
Forums: national asthma forums 1993, 1995, 1997, 1999; research forums 1997, 2000; respiratory care devices 1996, 1998, 2000
Development of medical training material (e.g. textbooks in Finnish: Pulmonary medicine (1997), Allergology (1999), Asthma (2000))
Networking
Asthma contact persons (local, n=757)
Asthma pharmacy contact persons (n=390)
Professional and public health organisations (n=20)
Materials, information
Asthma programme 1994–2000, Finn Med J (in Finnish) 1994;29:2883–921; Clin Exp Allergy 1996;26(suppl 1):1–24
Health education material
Guided self-management training packages
Asthma Week, Asthma Fair annually
Telephone guidance since 1994; Allergy and Asthma Federation, Pulmonary Association HELI
Improving diagnostics and treatment
Regional and local action plans and treatment chains
Treatment guidelines 1994, 2000
Guided self-management programme
Referral chains
Pharmacy programme 1998
Allergy treatment consensus 1999, Finnish College of Physicians
Early diagnosis and spirometry campaign 1999
Feedback
Follow up report 1998, Ministry of Social Affairs and Health
Follow up report on institutional care 1996, 1997, 1998, 1999
Tailor made local follow up reports since 2000
Specific reports and publications
Presentations in national and domestic conferences
Box 1 Finnish asthma programme: activities planned and undertaken.
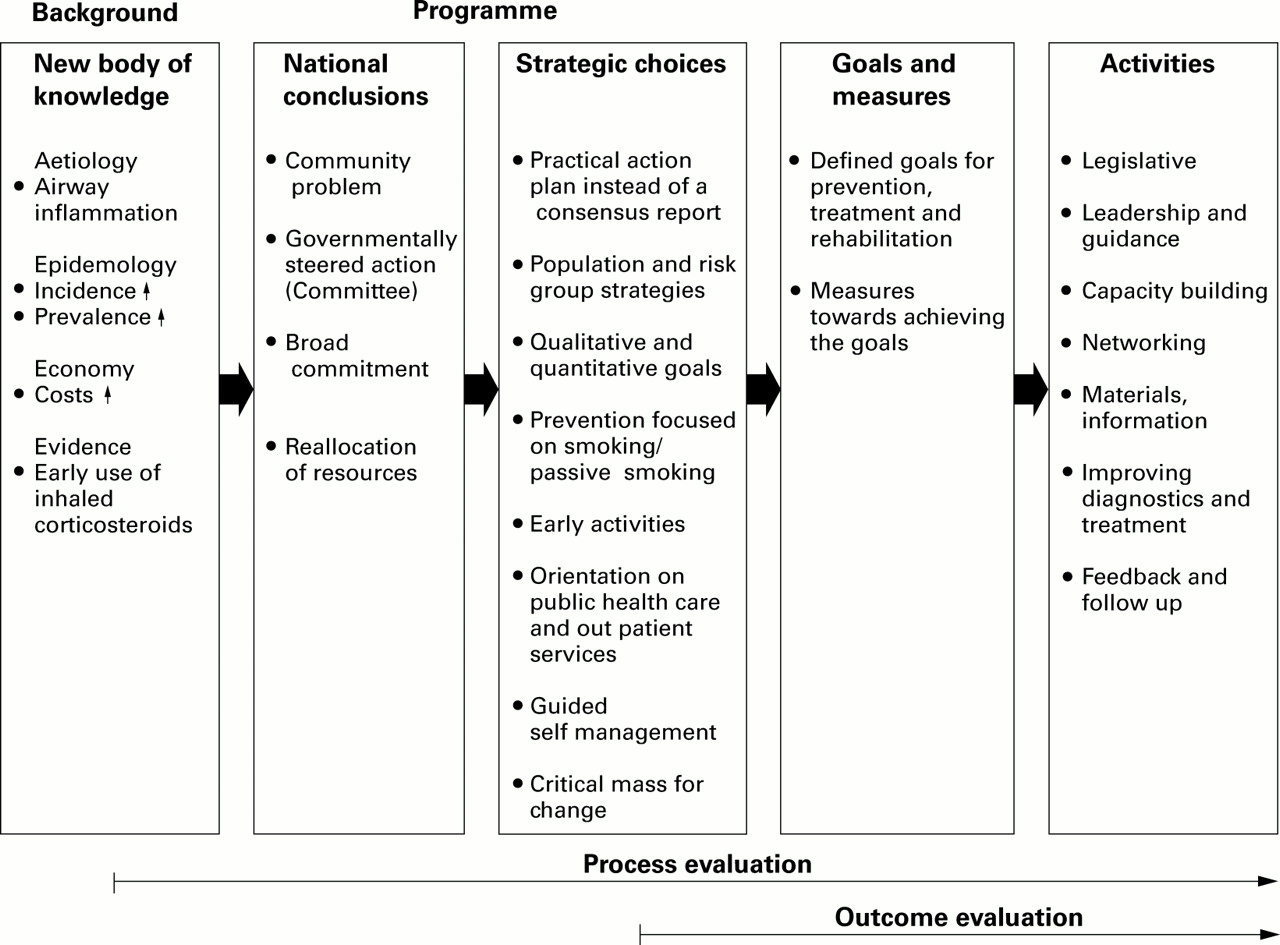
Flow chart of strategic planning, implementation, and evaluation of the programme.
For historical reasons, patients with asthma have been mostly cared for by pulmonary physicians and paediatricians in Finland. It was time to reconsider the division of labour because the growth in the number of patients allowed no alternatives. The steering committee recommended a revision of asthma care in order to increase the role of primary health care. One solution was to train one general practitioner and one nurse in each municipal health centre to work as coordinators of local activities and to take part in the counselling and follow up of patients.
In 1997 a further step was taken to strengthen the local activities by including more than 600 Finnish pharmacies in the programme. The steering committee recommended all pharmacies and health centres to contact each other in order to improve collaboration in the guidance and education of asthmatic patients. The pharmacies were also recommended to nominate one of the pharmacists to act as an asthma contact person.
Follow up and evaluation
IMPLEMENTATION AND COMMITMENT
To study the regional implementation and commitment to the programme, three surveys were conducted using structured questionnaires. The target groups were: (1) in 1998 chief physicians in hospital pulmonary units (31 respondents, response rate 94%), (2) in 1998 asthma contact persons in health centres (757 respondents, response rate 54%), and (3) in 2000 contact persons in those pharmacies which were stated to have a contact person (417/589 responders, response rate 71%).
The survey of chief physicians revealed a high commitment to the programme (table 1). Two thirds of 21 hospital districts had launched regional asthma programmes in line with the national programme. All districts had chosen one or more physicians (mostly a respiratory physician and a paediatrician) to be responsible for the implementation of the regional programme and education for adults and children. Some of the districts had also evaluated their regional programme. For instance, in Hyvinkää district in southern Finland the quality of referrals had improved considerably.15 In 1995 20% of the referrals included data on PEF monitoring or spirometric testing but by 1999 the proportion had increased to 60%. Visits to specialist units had decreased by almost 20%, which means that care of the patients by GPs had improved.
Commitment to the programme: 29/31 chief pulmonary physicians responded
Most of the municipal health care centres (246/261 centres, 94%) had nominated at least one contact person for the programme. Usually one doctor and one nurse in each centre were chosen to coordinate local activities. In addition, some public and private health care units stated that they had a total of 250 doctors or nurses with special skills for asthma care. In 2000 there were 757 such contact persons.
In the health centres, 50% of the 427 contact persons who responded to the inquiry reported participation in the national asthma forums, and 85% had taken part in the regional education sessions. Sixty eight per cent of the respondents thought that they were adequately trained for diagnosing and treating asthma, 17% considered their training as moderate, and 15% as inadequate. Fifty seven per cent of them considered their skills and knowledge to be sufficient for guidance of asthmatic patients, 38% considered their skills and knowledge to be moderate, and 5% poor.
More than 90% of the 417 pharmacies responding to the questionnaire had chosen a contact person who had participated in the regional training courses organised by the steering committee and the Finnish Association of Pharmacies. Sixty five per cent (271/417) of the responding pharmacies had had meetings with the health centre contact persons. Specialist doctors from local hospitals and representatives of patients' associations had also often taken part in these sessions.
The personnel in the pharmacies had especially focused on informing patients of the effects and side effects of asthma medication, on inhalation technique, and the correct use of various inhalers (table2). They had also motivated patients to use anti-inflammatory drugs as first line medication in persistent asthma on a regular basis.
Information given by pharmacists when patients were purchasing asthma medication (n=417, response rate 76%)
Implementation activities of the programme have been based on extensive training and re-training in the whole country, in which patient associations such as the Allergy and Asthma Federation, the Finnish Lung Health Association, and the Pulmonary Association HELI, as well as pharmaceutical companies, have also made important contributions. The main educational activities during the first 5 years of the programme are summarised in table 3.
Main educational activities undertaken during the first 5 years of the programme
HOSPITAL ADMISSIONS, MORTALITY, AND DISABILITY
The number of days in hospital due to asthma has been decreasing since the early 1980s, as has the mortality rate, but these trends had started long before the asthma programme was launched. It should be noted that the trend of decreasing use of hospital inpatient care also applies to many other somatic diseases. However, for asthma there is improved detection and treatment even though the disease severity may be decreasing. In contrast to asthma, the number of hospital days due to chronic obstructive pulmonary disease (COPD) has increased slightly during the 1990s.
In 1981 the Finnish Social Insurance Institution recorded 49 300 asthmatic patients who were entitled to special reimbursement for their drug costs and, in 2000, the figure had increased almost fivefold to 191 268. The number of hospitalised patients decreased in absolute terms from 13 820 (271/100 000 patients, 110 000 hospital days) in 1993 to 8891 patients (174/100 000, 72 000 hospital days) in 1999. In relation to the number of patients with special reimbursement—that is, the real at-risk population—the number of days in hospital in 1999 was only one quarter of that in 1981 (fig 2).

Relative increase in the number of asthmatic patients entitled to special reimbursement for their drug costs and decreases in death rate and days in hospital (index, 1981=100).
The mortality rate due to asthma has shown a similar trend (fig 2). The number of deaths ranged from 97 to 134 during the 1990s with no systematic trend; in 1994 there were 107 deaths from asthma and in 1998 the number was 134. As a proportion of the number of patients with registered asthma, the respective rates were 0.75/1000 in 1994 and 0.74/1000 in 1998. Asthma related deaths in children have become very rare with only a few cases having occurred in 10 years.
In comparison with musculoskeletal or cardiovascular diseases or mental disorders, asthma is a relatively rare cause for disability to work. In 1996 7.9% of asthmatic patients of working age received disability pension and in 1999 the corresponding figure was 5.5%.
The daily allowances paid by the sickness insurance because of asthma have decreased by 39% in the period from 1994 to 1999. Compensation was paid for 164 400 lost days in 1994 and for 100 900 days in 1999. These figures include only those absences from work which had lasted at least 10 days, for which allowances can be paid.
The number of patients attending rehabilitation courses decreased by 23% from 2300 in 1994 to 1764 in 1999.
In 1996 asthma was the main reason for 630 000 outpatient doctor visits in Finland,16 200 000 of which concerned children. Figures from earlier years are not available.
TRENDS IN ASTHMA MEDICATION
The Social Insurance Institution (SII) is responsible for the planning and administration of the national health insurance scheme which covers the total population of 5.1 million people. SII uses two registers: (1) a register of patients entitled to special drug cost reimbursement and (2) the national prescription register which includes data on all reimbursed purchases of medicines. From these two registers patients can be identified and their medication and its cost can be investigated.
If a specialist doctor (in some cases also a general practitioner) verifies reversible bronchial obstruction with lung function tests and the patient needs regular asthma medication after a 6 months follow up period, he or she can be entitled to 75% reimbursement for the drug costs instead of the ordinary 50%.
In 1994 the number of patients with asthma entitled to special reimbursement was 143 379, of which 19 225 (13.4%) were children (<16 years). In 2000 the total number had increased by 33% to 191 268 of which 29 099 (15.2%) were children. In 2000, 56% of patients were female. In children, however, the occurrence of asthma was twice as high in boys as in girls.
Since the early 1980s there has been a continuous increase in the number of patients entitled to special reimbursement of their drug costs. However, for the first time in 1997 the number of new cases in the 0–44 age group was smaller than in the previous year, which may indicate earlier and more effective intervention of asthma resulting in less persistent disease (fig 3A). The incidence of new asthma cases has two peaks: a high peak in small children and a smaller one in old people (fig 3B). The latter peak is slightly influenced by patients with COPD who can have special reimbursement if their bronchial obstruction shows 15% reversibility in the bronchodilator test. COPD accounts for about 5% of all patients entitled to reimbursement in the older age groups.
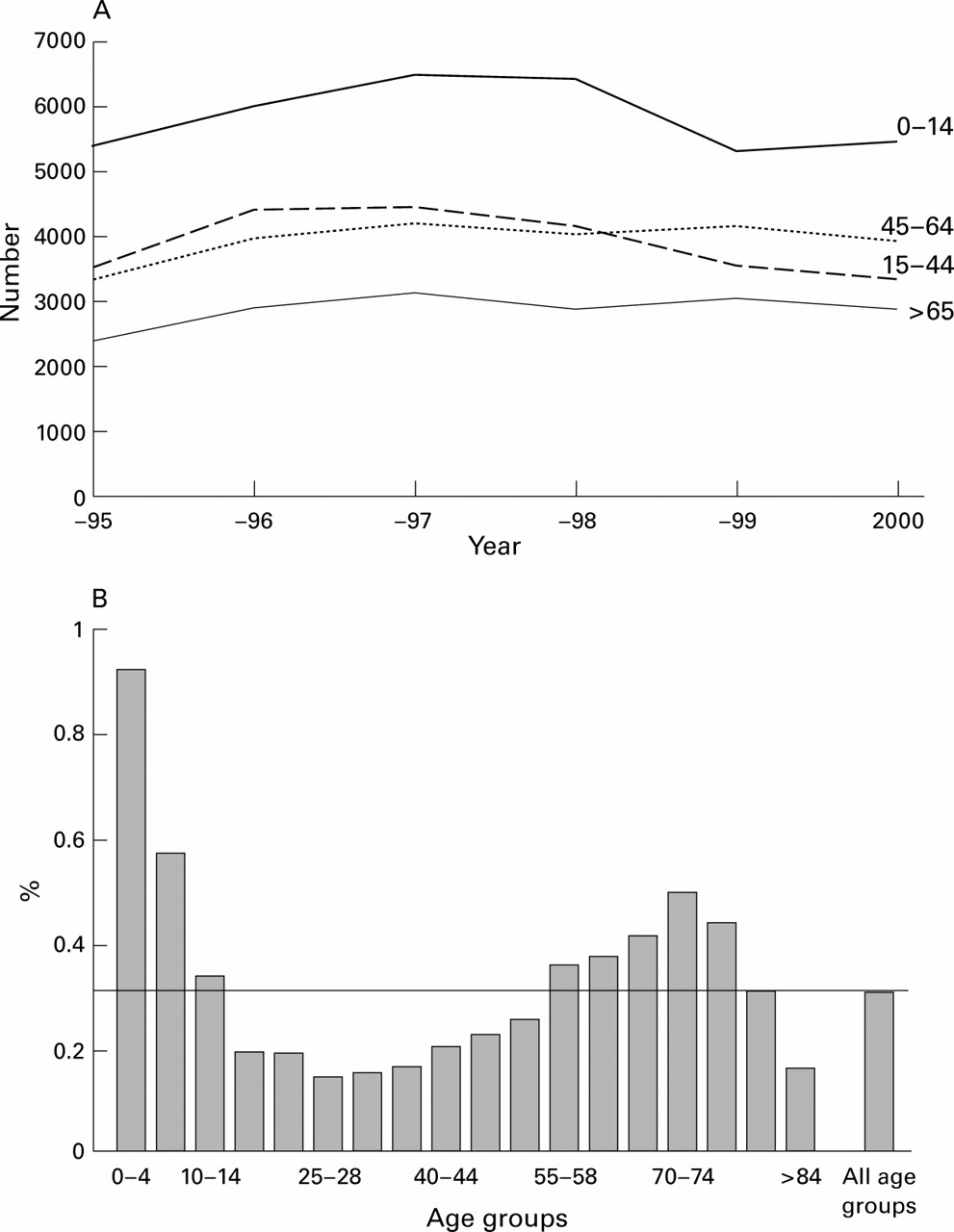
(A) Number of new patients receiving special reimbursement for drug costs from 1995 to 2000 by age group. (B) Incidence of new asthma patients (%) according to the special reimbursement register in the year 2000 by age group.
In addition to patients who are entitled to special reimbursement, there are also patients who use asthma medication occasionally or intermittently because of less persistent disease. In 1994 a total of 233 000 patients purchased asthma medication while in 2000 the figure had increased by 42% to 332 000.
The use of preventive medicines has grown more rapidly than symptom relieving, short acting β2 agonists. The growth in the number of users of inhaled corticosteroids from 1994 to 1999 was 75% while the corresponding figure for short acting β2agonists was 27%. This could be interpreted as a sign of improved disease control. In 1994 Finland was the first Nordic country in which the ratio of defined daily doses (DDD) of preventers to those of relievers exceeded 1.0 (fig 4).17 During the last few years the use of long acting β2 agonists has increased rapidly, which may also have affected the need for short acting relievers.

Ratio of the use of inhaled corticosteroids and short acting β2 agonists from 1994 to 1999.
Modern medication of other than mild forms of asthma consists of at least two asthma medicines, one for prevention and another for treating occasional symptoms. In more severe cases several medicines may be necessary. In a nationwide study in 1996 of asthmatic patients of working age, 16% used only one drug, 58% two drugs (an inhaled steroid and a short acting β2 agonist), 21% used three drugs (the third medicine was in most cases a long acting β2 agonist), and only 5% used four drugs concomitantly.18
Of all the nearly 50 chronic diseases which entitle the patient to special reimbursement, asthma was the second largest at the end of 2000 with only hypertension having more patients. In children, however, asthma was by far the most common chronic disease.
TRENDS IN SMOKING
Smoking patterns among the Finnish adult population are followed regularly by a large postal survey which records health behaviour among adults in Finland.19
Antismoking legislation was revised in 1995 and 2000. Smoking was prohibited at work places except in special smoking rooms. The sale of tobacco products to children younger than 18 years was prohibited. The latest revision demands smoking free areas in restaurants and bars. Finland has Europe's strictest tobacco legislation, and regular smoking by adults has continuously decreased. In 1999 27% of men and 20% of women aged 15–64 years smoked regularly (fig 5A). Passive smoking has decreased accordingly (fig 5B). However, smoking has not decreased among young people; in 1999 17% of 14 year old girls and 12% of boys were daily smokers, and smoking has even increased in girls during the 1990s (fig 5C).

Trends in tobacco use in Finland. (A) Proportion of smokers (%) 1950–99. (B) Daily exposure to cigarette smoke at work for at least one hour, 1985–99. (C) Proportion of daily smokers (%) among 14 year olds, 1977–99.
In 1995–9 only 26% of smokers had been given antismoking advice and counselling by a healthcare professional during the preceding year.20 This is not a satisfactory figure and should be improved.
Finnish national health interview surveys indicate that 27% of asthmatic men were regular smokers in 1987, decreasing to 19% in 1996, while the corresponding figures for men in general were 33% and 26% (unpublished data). Among asthmatic women in 1987 the figures were 16% and 10%, respectively, and 18% and 14% for women in general. In the 15–29 year age group in 1996 smoking was even more frequent among asthmatic subjects than in non-asthmatic subjects. This indicates that asthmatics smoke almost as often as the rest of the population.
TRENDS IN COSTS
Improved disease control means less need for hospital admissions, less absenteeism from work, and improvement in the quality of life. The monetary value of these changes is, however, difficult to estimate because a hospital bed will be filled with another patient if an asthmatic patient does not need it. Loss of production might occur during a short absence from work, but a longstanding or permanent invalidity usually means that somebody else replaces the empty work place. The overall costs of asthma per patient in Finland have probably slowly decreased, but interesting opposite trends have taken place.
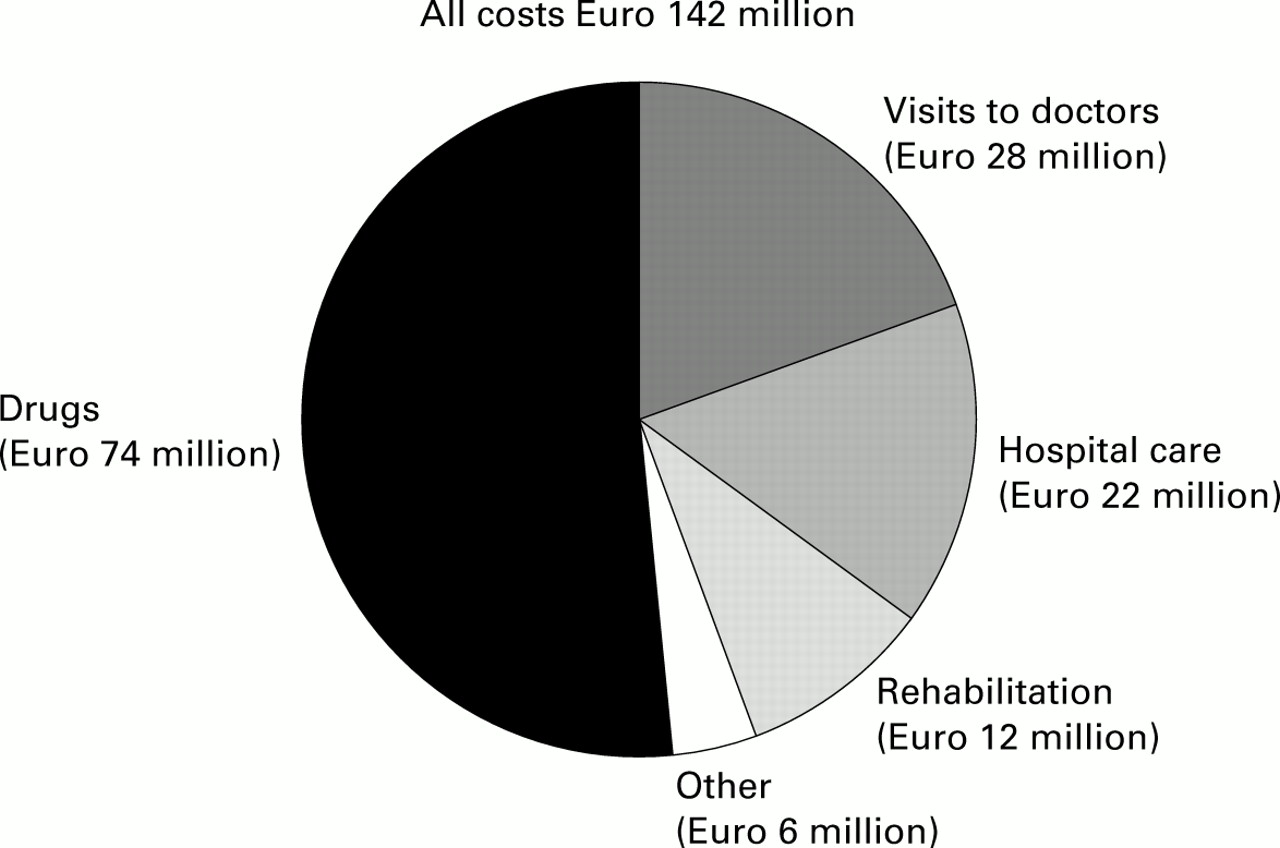
At the end of the 1990s the direct costs of asthma treatment were around Euro 142 million (fig 6). The proportion of these costs attributable to asthma medication was more than half. The cost of asthma drugs in outpatient care was Euro 30 million higher in 1999 than in 1994 (Euro 74 million and 44 million, respectively). Annual costs of medication per patient with special reimbursement—that is, persistent asthma needing regular treatment—were 22% higher in 1999 than in 1994 (Euro 419 and 343 per patient, respectively). Asthma medication has become more expensive, mainly because of new innovations such as fluticasone, formoterol, salmeterol, combination inhalers, and leukotriene modifiers.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Distribution of direct annual costs of asthma in Finland in the late 1990s. Total costs were around Euro 142 million.
In 1999 asthma accounted for about 38 000 hospital inpatient days fewer than in 1993 (the year before the programme was launched), which means a cost decrease of about Euro 11.5 million. The costs for absenteeism from work for asthma were about Euro 14.5 million less in 1999 than in 1994. However, these savings (Euro 26 million) are offset by the increased drug costs.
EARLY TRACKING SURVEY
An asthma barometer survey of the follow up of the programme at the patient level was conducted in 550 pharmacies during two consecutive days in June 1998. A questionnaire was given to all subjects purchasing asthma medication for themselves or for their children. The structured questions concerned frequency of asthmatic symptoms, use of health services due to asthma, current medication, and opinions on the quality of treatment. 2860 patients (59% female) responded (14% <16 years, 61% 16–64 years, and 25% >65 years). According to the national prescription register, they were a fairly good geographical and demographic representation of the Finnish population with asthma.
The severity of asthma was assessed by asking about the frequency of symptoms during the preceding year (0 = no breathing difficulties or wheezing, 1 = less frequently than once a week, 2 = 1–2 times per week, 3 = 3–4 times per week, and 4 = daily or almost daily). Answers 0–2 were considered to indicate mild asthma, 3–4 moderate to severe asthma. Of the 2851 responders, 9% did not have these symptoms at all. Asthma was considered mild in 65% and moderate to severe in 35% of the patients. The proportion of mild cases was highest among children and lowest among the elderly. Seventy seven per cent of the patients reported that they had their “own” asthma doctor who took care of their treatment; 44% of these doctors were specialists, 36% were GPs in health centres, and 10% were in occupational health care. Seventy eight per cent of the patients reported that they were satisfied with the organisation of their treatment (range 67–82% in different districts).
The survey showed that patients worried most about adverse effects of their asthma medication; 29% mentioned adverse effects as a major problem and 19% had actually experienced side effects. Patients also had problems remembering to take their anti-inflammatory medication regularly (18%), and many felt it was difficult to use inhalers in a public place. Only 8% reported difficulties in the actual inhalation technique.
What have we learned?
During the 1990s many important asthma management guidelines have been produced.21-26 They aim to improve the standard of asthma care, but still “the current level of asthma control in Europe falls far short of the goals for long term asthma management”.27
The Finnish concept was to develop a multidisciplinary action programme which included not only strategies for prevention and treatment, but also an operational plan for their dissemination and implementation. Effective strategies involve multiple methods, decision support systems, and interactive education.28 Production of guidelines is meaningless if they are not used in practice.29 State officials, representatives of patient organisations, nurses, pharmacists, and GPs took part in the steering group of the programme. They were the keys to the successful creation of a network of contacts in local health centres as well as regional and local treatment programmes. This network included as many nurses as doctors, which was considered beneficial. The feasibility of the programme was good, as shown by the rapid build up of the contact person network and the high rate of participation in the educational activities.
The extra costs of planning and implementing the programme have been small, mainly because most of the activities have been carried out as part of the routine work of the clinicians and administrators. The Ministry of Social Affairs and Health has shown a political commitment towards the programme by allocating financial resources to cover the salary (Euro 50 000 annually) of one pulmonologist based in the Lung Health Association to coordinate the activities.
Asthma care has shown considerable improvement in Finland. One indicator of improved care in health centres is the need for acute hospital admissions. For instance, in 1996–8 in North Karelia (population 140 000) the percentage of acute asthma admissions of all admissions varied in 19 communities from 35% to 80%. Interestingly, one of the most active asthma contact doctors worked in the community with the lowest percentage. In a 2 year period (1995–6) 2.4% of children living in Turku hospital district and 1.2% in Tampere district used inhaled corticosteroids regularly. Hospital admissions were more rare in the Turku area. In the two districts 21% of those children on regular corticosteroid treatment were hospitalised because of a severe wheezing episode compared with 47% of those who were not.30
From 1994 to 2000 the number of asthma drug users in Finland increased by 42% from 233 000 to 332 000. This indicated improved detection and treatment of asthmatic symptoms in the population, even though there may also have been some increase in the occurrence of asthma. The major increase (75%) in the use of inhaled steroids was a direct consequence of the programme which promoted their introduction as first line treatment after diagnosis. In 1994 Finland was the first Nordic country in which the ratio of preventive to relief medication exceeded 1.0. In general practice the high ratio of steroids to bronchodilators in asthma treatment has been associated with decreased morbidity.31
The number of children and young adults with new special reimbursements for drug costs in 1997 was smaller than in previous years for the first time, which may mean better disease outcome. A child treated effectively at an early stage usually becomes free of symptoms and needs only intermittent treatment.32 On the other hand, the severity of asthma may be decreasing, which might in part explain these trends.
The programme recommended a simple treatment regimen. Concomitant use of many drugs decreases compliance, increases the risk of side effects and costs, and is a challenge to self-management programmes. In 1996 58% of patients of working age used two drugs—usually an inhaled corticosteroid as a preventer and a short acting β2agonist as a reliever. The better the disease is controlled with inhaled steroids, the smaller is the need for β2 agonists which could be used as a control indicator. This simple regimen has been completed (and partly complicated) by increasing the use of long acting β2 agonists and recently by combination preparations. A condensed version of the present Finnish expert opinion on the asthma medication to be used in all health care is shown in box 2.33
Principle 1: Start effective treatment early, win the patient's confidence, and improve the outcome.
Start with anti-inflammatory medication and adjust the dose according to the need for the reliever, short acting β2 agonist
Start with an inhaled steroid (e.g. beclomethasone 200 μg, 2–4 inhalations twice daily) for 2–8 weeks. Step down to maintain the result (200 μg, 1–2 inhalations twice daily) for several months. Step down to find the lowest dose able to control the symptoms
If treatment is insufficient, check the inhalation technique and compliance
Principle 2: Treat according to disease severity
Intermittent symptoms: inhaled steroids 2–8 week courses. Short acting β2 agonist as needed
Mild persistent symptoms: inhaled steroids regularly (e.g. beclomethasone 200 μg, two inhalations twice daily). Short acting β2 agonist as needed
Moderate persistent symptoms: inhaled steroids regularly. If necessary, add long acting β2 agonist, low dose theophylline (200–300 mg), or a leukotriene modifier. Short acting β2 agonist as needed
Severe persistent symptoms: add prednisolone tablets in the morning to the above regimen
Principle 3: Treat exacerbations early
Double the dose of inhaled steroid for 2 weeks. If necessary, add long acting β2 agonist, low dose theophylline, or a leukotriene antagonist
If the patient does not improve in 2 days, add prednisolone 20–40 mg in the morning for 1 week
Prevent further exacerbations by adjusting the regular treatment
Principle 4: Educate the patient, a written self-management plan is preferred
Guide the patient to use PEF measurements at home if disease control is not optimal
If morning PEF decreases by more than 30% or by more than 15% on two consecutive mornings, treat like an exacerbation
Box 2 Four essential principles in asthma medication for adults. Modified from Haahtela et al.33
Approximately 70% of asthma is mild and may need only intermittent drug treatment. Patients free of symptoms are not compliant with regular use of preventive medication. Should they be? For most patients the risks of a clinically significant decline in lung function because of irreversible structural changes of the bronchi (remodelling) is probably small. We should rethink the concept of treatment compliance in order to advise patients successfully.34 ,35 The patients should feel that they are managers of their treatment, which is supported not dictated by healthcare professionals. Cooperation and listening are the key words.
The basic question remains: how to prevent asthma in the first place? There is no evidence based means for primary prophylaxis. Stopping the “atopic march” in early childhood could be an option to decrease the incidence of atopic asthma. Modifying the gastrointestinal microflora by lactobacillus GG in newborn infants with high allergy risk was recently shown to reduce the occurrence of atopic dermatitis at 2 years of age.36 Prevention could be improved by focusing on the clinical phenomenon that occurs even before asthma. Antihistamine (cetirizine) treatment of 1–2 year old children with signs of atopic dermatitis sensitised to airborne allergens may have some preventive effect.37 Treatment of allergic rhinitis with specific immunotherapy may also prevent asthma.38 Effective prevention will only be possible when we learn more of the genetic background of asthma and allergies39 and of the complex interaction of genes and the environment.
Both children and adults can have episodes of eosinophilic bronchial inflammation during respiratory infections or allergen exposure, but most of the time lung function is normal or close to normal.13 These patients could be intercepted even before asthma develops (as defined in terms of abnormal lung function). Whether interventions at that stage could prevent asthma is, however, not known. Asthma is a man-made definition and is quite arbitrary. In real life there is a biological continuum from mild episodes of “asthmatic” inflammation to fatal attacks. We need handy and practical diagnostic tools for detecting early signs of asthmatic inflammation and to monitor its course. Lung function tests such as peak flow measurements are useful in monitoring patients with moderate to severe persistent asthma.
Strict anti-smoking legislation and campaigns have been successful in decreasing regular smoking by Finnish adults. Passive smoking has decreased accordingly. However, 15–29 year old asthmatic subjects smoked even more than the rest of the population of this age, which calls for better focused anti-smoking campaigns. Overall, smoking is an important cause of COPD but is less significant in asthma.
Several factors have contributed to the positive trends of asthma in Finland. Although the disease may have become milder, the active national programme has contributed to this favourable development. Because the whole healthcare system has been involved in improving asthma care in Finland, the programme does not have a control. This is an argument which large scale community actions always face. We do not know what would have happened without the programme.
Where are we now?
The programme was aimed for the period 1994–2004. The present assessment highlights the situation in the middle of that period.
GOAL 1: RECOVERY OF AS MANY PATIENTS AS POSSIBLE WITH EARLY ASTHMA
We are moving in the right direction. The number of children and young adults with new special reimbursement for drug costs has reached a turning point and is decreasing. This probably means that patients who have previously received entitlement to special reimbursement do not need it any longer after successful treatment.
GOAL 2: PATIENTS SHOULD FEEL WELL, AND THEIR ABILITY FOR WORK AND FUNCTIONAL CAPACITY SHOULD CORRESPOND WITH THEIR AGE
This goal has been partly reached. The numbers of hospital days, disability pensions, and allowances for days off work have decreased substantially, and the number of patients having rehabilitation courses has also decreased. The use of relievers has not grown during the late 1990s.
GOAL 3: DECLINE IN THE PERCENTAGE OF PATIENTS WITH SEVERE AND MODERATE ASTHMA FROM 40% TO 20%
This goal has been at least partly achieved. In 1989 lung specialists estimated that 40% of Finnish patients having special reimbursement for drug costs suffered from moderate or severe asthma.40 In 1998 the figure was 35%, when the estimate was based on patient reported symptoms. These figures cannot be directly compared, but several indicators show that the proportion of patients with severe complications has decreased.
GOAL 4: DECREASE IN THE NUMBER OF BED DAYS BY 50% BY THE YEAR 2000
This goal has not been fully reached. The number of days has fallen by 35% from 110 000 in 1994 to 72 000 in 1999, and the trend is downwards.
GOAL 5: REDUCTION IN ANNUAL COSTS PER PATIENT BY 50%
If all the direct and indirect costs are taken into account (drugs, hospital days, outpatient doctor visits, rehabilitation, disability pensions), it is our rough estimate that the total costs per patient have decreased by 10–20% even though the costs of medication have increased substantially (fig 6).
References
Footnotes
Other members of the Working Group: E Ahonen, P Hulkkonen, K Juntunen-Backman, M Kolimaa, S Koskivuori, E Kukkonen, A Lahdensuo, R Muotka, T Nurmi, S Peura, M Turpeinen, E-L Vakkilainen.