Article Text

Statistics from Altmetric.com
- eNOS, endothelial nitric oxide synthase
- Cmax, maximum serum concentration
- PAP, pulmonary arterial blood pressure
- PH, pulmonary hypertension
- PVR, pulmonary vascular resistance
- VSMC, vascular smooth muscle cell
Pulmonary hypertension (PH) is characterised by progressive elevation of pulmonary artery pressure and pulmonary vascular resistance. Pathohistological findings have demonstrated that PH is associated with abnormal vascular structures, including medial and/or intimal hypertrophy, concentric or eccentric intimal fibrosis, obstruction in the arterial lumen, and aneurysmal dilatation.1 Patients with PH are currently treated with anticoagulant agents, vasodilators including continuous intravenous prostacyclin (prostaglandin I2) and oral sildenafil or bosentan, and in end stage, with lung transplantation,1 when applicable. Endothelial dysfunction of pulmonary arteries and enhanced pulmonary vasoconstriction contribute to the development of PH.1 Endothelial nitric oxide synthase (eNOS) expression is reduced in patients with PH and therefore nitric oxide inhalation and sildenafil are useful for those patients. However, more effective treatments remain to be developed.1
We have recently demonstrated that Rho-kinase is substantially involved in the pathogenesis of a wide range of cardiovascular disease.2,3 Rho-kinase suppresses myosin phosphatase activity by phosphorylating the myosin binding subunit of the enzyme and thus augments vascular smooth muscle cell (VSMC) contraction at a given intracellular calcium concentration.4 Indeed, we have demonstrated that a Rho-kinase inhibitor, fasudil, suppresses abnormal hyperconstriction of forearm and coronary arteries in animals and humans.2,3 Moreover, we have recently demonstrated that Rho-kinase inhibition increases eNOS expression and decreases inflammatory cell migration or anigiotensin II induced mRNA expression of monocyte chemoattractant protein-1 and plasminogen activator inhibitor-1 in vivo and in vitro.3 Our in vivo study also indicated that long term oral treatment with fasudil notably ameliorates monocrotaline induced PH and pulmonary vascular lesions in rats.5 In the present study, we thus examined the acute vasodilatory effects of pulmonary circulation by intravenous administration of fasudil in patients with severe PH.
METHODS
The ethical committee of the Kyushu University Hospital approved this study and all patients provided informed consent before the study. Nine patients with severe PH (mean age 53 years; range 26–76 years, three men and six women) were prospectively enrolled to examine the acute effects of a Rho-kinase inhibitor, fasudil hydrochloride, on pulmonary circulation at the Kyushu University Hospital. All patients underwent right heart cardiac catheterisation while they continued all medications, including oral or intravenous prostaglandin I2. We measured pulmonary vascular resistance (PVR), systemic and pulmonary arterial blood pressure (PAP), and cardiac index, using a Swan-Ganz catheter. We examined the response to intravenous administration of fasudil hydrochloride (30 mg for 30 minutes).
Blood samples were taken before and 1, 2, 4, and 8 hours after intravenous administration of fasudil hydrochloride to measure serum concentrations of fasudil and hydroxyfasudil, an active metabolite of fasudil (Daiichi Chemical and Pharmacological Company, Ibaragi, Japan).2
RESULTS
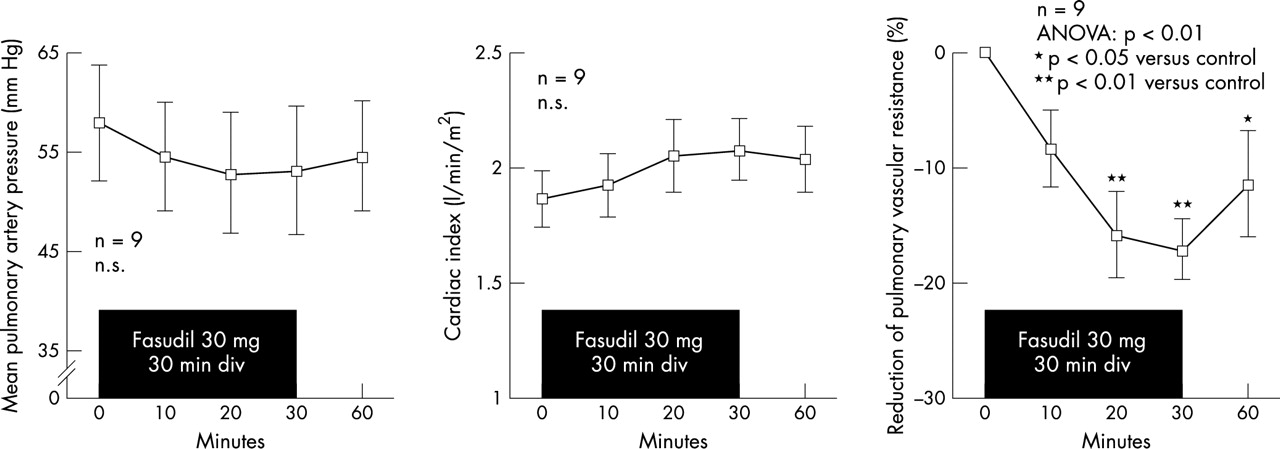
Mean systolic/diastolic/PAP at baseline was 94/36/58 mm Hg and mean PVR index was 2429 dyne*sec*cm−5*m2. Figure 1⇓ shows that intravenous administration of fasudil slightly decreased PAP and increased cardiac index in these patients, although there were no significant differences; however, it significantly reduced PVR by 17% in nine patients. There were no side effects, including systemic hypotension.
{kind=link}
Intravenous administration of fasudil slightly decreased pulmonary artery pressure (left panel) and increased cardiac index (middle panel), although there were no significant differences. However, fasudil significantly reduced pulmonary vascular resistance (right panel). Data are expressed as mean (SD) and analysed by ANOVA followed by a Fisher’s post hoc test.
Intravenous administration of fasudil achieved maximum serum concentration (Cmax) of 278.9 (150.5) ng/ml of fasudil and 173.2 (10.3) ng/ml of hydroxyfasudil. Time to achieve half of Cmax (T½) was 0.5 (0.6) hours for fasudil and 3.6 (1.6) hours for hydroxyfasudil.
DISCUSSION
Based on our findings in animals, we examined the possible involvement of Rho-kinase in the pathogenesis of PH in humans in the present study and the results indicated that it is indeed involved. Increased PVR may be caused by both pulmonary vascular remodelling and sustained pulmonary vascular vasoconstriction.1 The mechanisms involved in the latter include endothelial dysfunction and VSMC hyperconstriction.1 In the present study, fasudil reduced PVR, indicating that VSMC hyperconstriction in PH is partially caused by increased Rho-kinase activity. Our series of experiments suggest that long term blockade of Rho-kinase causes a regression of vascular remodelling,3,5 although the Cmax of fasudil/hydroxyfasudil in the present study indicates its vasodilatory effect but not its antiproliferative one.3 We plan to examine whether additional long term oral treatment with fasudil further decreases PAP and improves quality of life and survival of patients with severe PH.
Acknowledgments
This study was supported in part by the grants-in-aid (numbers 13307024, 13557068) and the grant for the 21st Century COE Program from the Japanese Ministry of Education, Culture, Sports, Science and Technology, Tokyo, Japan and from the Program for Promotion of Fundamental Studies in Health Sciences of the Organization for Pharmaceutical Safety and Research of Japan.