Article Text

Statistics from Altmetric.com
Introduction
Occupational asthma is the most frequently reported work-related respiratory disease in many countries. It is defined as asthma that is caused by a specific workplace exposure to certain substances and not to factors outside the workplace. In a recent review, the population attributable risk for adult onset asthma being caused by occupational exposures was 17.6%. Occupational asthma can lead to decreased quality of life, sickness absence and increased costs for the patient, the employer and society. Common causes of occupational asthma include exposure to high molecular weight (HMW) agents such as wheat, latex and animal proteins, or to low molecular weight (LMW) agents such as di-isocyanates, acid anhydrides, platinum salts and plicatic acid. There are no systematic reviews of controlled studies of workplace interventions for occupational asthma. Therefore, we conducted a Cochrane systematic review to evaluate the effectiveness of workplace interventions on the outcome of occupational asthma.1
Methods
We searched the Cochrane Central Register of Controlled Trials (CENTRAL), MEDLINE, Embase, NIOSHTIC-2, CISDOC and HSELINE up to February 2011.
We intended to include randomised controlled trials, controlled before and after studies and interrupted time series of workplace interventions for occupational asthma, but we only identified studies with a controlled before–after design. Other inclusion criteria were being diagnosed with occupational asthma, outcomes measured as asthma symptoms or lung function at follow-up and any workplace intervention. For asthma symptoms, we used both the absence of symptoms and the improvement of symptoms as outcome measures. For lung function, we used both the forced expiratory volume in the first second (FEV1) as a percentage of a predicted or reference value and non-specific bronchial hyper-reactivity (NSBH) as outcome measures. Two authors independently assessed study eligibility and trial quality, and extracted data. The results of the studies for homogeneous comparisons were combined in a meta-analysis.
We included 21 controlled before and after studies with 1447 participants that reported on 29 comparisons. Of the 21 studies, only two were intentionally designed as an intervention study. The others were follow-up studies.
Results
Fifteen studies compared workers who were removed from exposure with those who continued to be exposed. In six studies, reduction of exposure was compared with continued exposure and in another eight studies workers who were removed from exposure were compared with those for whom exposure was reduced. The causal agent was of HMW in four studies, LMW in 14 studies, both HMW and LMW in two studies and pot room gases in one study. The mean follow-up time was 3.8 years and ranged from 5 weeks to 11.5 years. The mean duration of exposure prior to diagnosis was 7.2 years and the mean duration of symptoms prior to diagnosis was 5.5 years. Both were mentioned only in half of the studies and varied considerably within a single study. The diagnosis of occupational asthma was based on specific inhalation challenge with the suspected causative agent in 17 studies. The number of participants in the included studies varied from nine to 201.
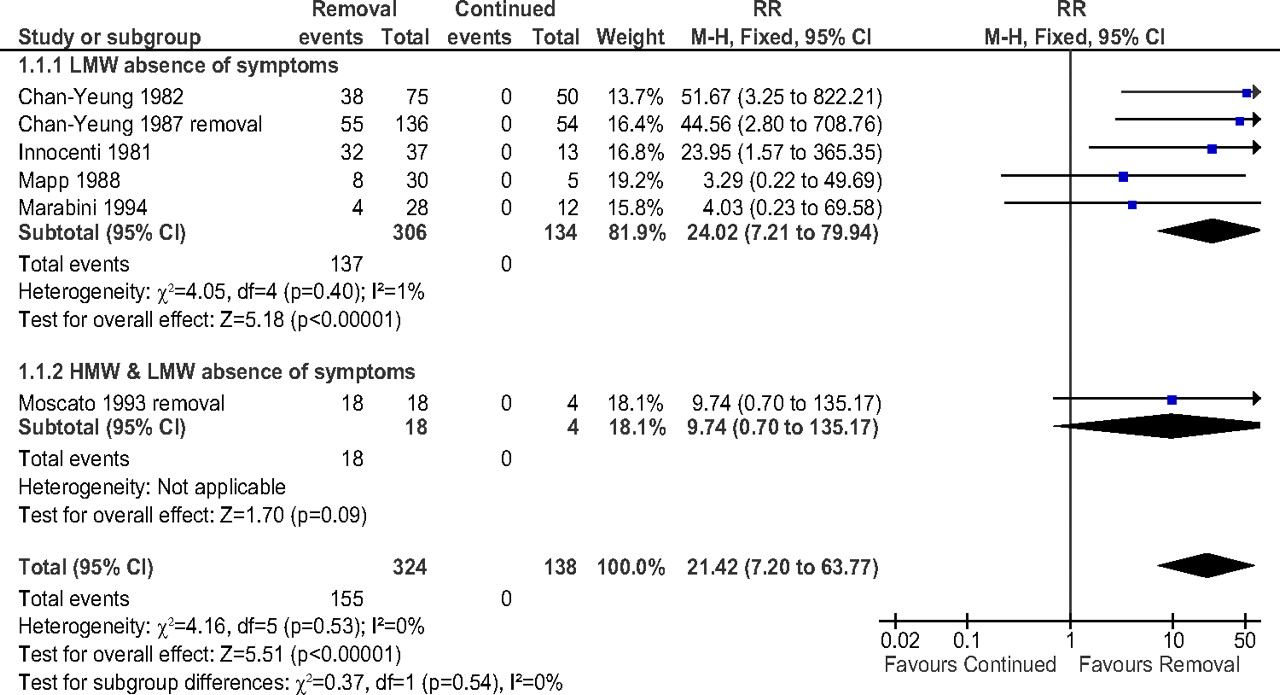
Compared with continued exposure, removal from exposure increased the likelihood of reporting absence of symptoms (RR 21.42, 95% CI 7.20 to 63.77), improved FEV1% (mean difference (MD) 5.52 percentage points, 95% CI 2.99 to 8.06) and decreased NSBH (standardised mean difference (SMD) 0.67, 95% CI 0.13 to 1.21) (figure 1).

{kind=link}
Meta-analysis of the effect of removal from exposure versus continued exposure on absence of asthma symptoms at follow-up. Fixed: fixed effects model; LMW: studies that included participants exposed to low molecular weight agents; HMW and LMW: studies that included participants exposed to low and to high molecular agents; M-H: Mantel-Haenzel method for synthesising studies.
Compared with continued exposure, interventions to reduce exposure also increased the likelihood of reporting absence of symptoms (RR 5.35, 95% CI 1.40 to 20.48) but did not affect FEV1% (MD 1.18 percentage points, 95% CI −2.96 to 5.32). No data were available for hyper-reactivity.
Compared with interventions to reduce exposure, removing workers totally from their exposure at work increased the likelihood of reporting absence of symptoms (RR 39.16, 95% CI 7.21 to 212.83) but did not affect FEV1% (MD 1.16 percentage points, 95% CI −7.51 to 9.84). No data were available for hyper-reactivity.
Two studies reported that the risk of unemployment after removal from exposure was increased compared with reduction of exposure (RR 14.3, 95% CI 2.06 to 99.16). Three studies reported loss of income of about 25% after removal from exposure.
Discussion
As all studies were observational studies, we rated the quality of the evidence as moderate. In addition, all studies had a high risk of bias which we considered an additional serious limitation. Therefore, we downgraded the quality of evidence for all comparisons to ‘very low’.
We concluded that removal of individuals with occupational asthma from exposure when compared with continued exposure is associated with a beneficial effect on asthma symptoms and lung function including both FEV1 and NSBH. This is especially apparent for occupational asthma due to LMW agents.
Interventions to reduce exposure are also associated with beneficial effects on symptoms, but there was no significant effect on lung function when compared with continued exposure.
Removal from exposure improved asthma symptoms more than reduction of exposure, but there was no significant difference in lung function. However, one unintended consequence of removal from exposure is a much higher risk of loss of work and income than following reduction of exposure.
Further randomised controlled trials are needed to determine which interventions to reduce exposure provide most benefit.
Acknowledgments
This review was conducted under the auspices of the Cochrane Occupational Safety and Health Review Group. We thank Leena Isotalo for her assistance with the searches and Jani Ruotsalainen for all the editorial services.
Reference
Footnotes
This paper is based on a Cochrane Review published in The Cochrane Library 2011, Issue 51 (see http://www.thecochranelibrary.com for information). Cochrane Reviews are regularly updated as new evidence emerges and in response to feedback, and The Cochrane Library should be consulted for the most recent version of the review.
Competing interests None.
Provenance and peer review Not commissioned; internally peer reviewed.