Article Text

Abstract
Background: The phase of the menstrual cycle is thought to influence the course of asthma in women. One recent study reported a large increase in exacerbations during the perimenstrual phase, while another found a preovulatory increase. A study was undertaken to determine the relation between phase of the menstrual cycle and acute asthma in patients presenting to the emergency department (ED).
Methods: All women aged 18–54 years presenting with a diagnosis of acute asthma exacerbation were considered for enrolment in the study. Women who were pregnant, postmenopausal, following hysterectomy, with a >28 day menstrual cycle or incomplete reproductive history were excluded. The 792 eligible women were classified by menstrual phase based on both date of symptom onset and date of ED visit.
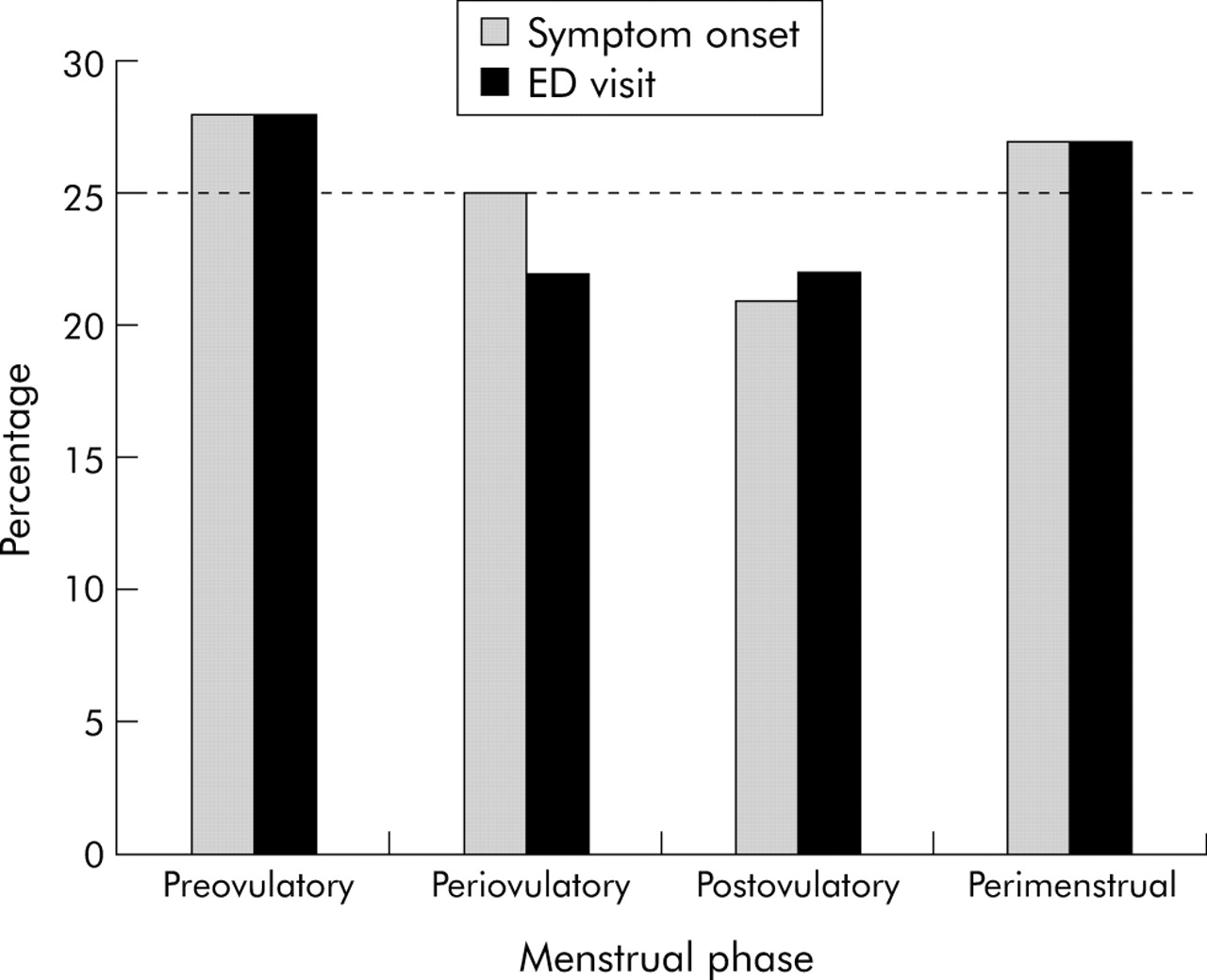
Results: When classified by date of symptom onset, 28% were preovulatory (days 5 to 11), 25% were periovulatory (days 12 to 18), 21% were postovulatory (days 19 to 25), and 27% were perimenstrual (days 26 to 4; p = 0.03). When classified by date of ED visit, 28% were preovulatory, 22% were periovulatory, 22% were postovulatory, and 27% were perimenstrual (p = 0.004). Using either approach, there were no significant differences in demographic factors or in asthma severity of women in the various menstrual phase groups.
Conclusion: Acute asthma exacerbations do not markedly increase during the perimenstrual phase. The results support the suggestion that both preovulatory and perimenstrual phases are actual triggers of asthma exacerbation in some women, or that these two phases serve as “co-factors” that worsen other recognised triggers of acute asthma.
- asthma
- sex hormones
- menstruation
- emergency department
Statistics from Altmetric.com
Asthma is a significant chronic illness in the US that has been increasing in prevalence for at least two decades.1 Asthma related healthcare utilisation has increased throughout this same period. For example, the annual age adjusted rate of emergency department (ED) visits for asthma has increased in the US from 57 per 10 000 population in 1992 to 73 per 10 000 population in 1999.2
In studying the increase, several groups have found sex differences in the prevalence of asthma across the life cycle.3 Asthma is more common initially in boys but then becomes more common among women of reproductive age. According to the 2000 Behavioral Risk Factor Surveillance System, the prevalence of asthma is 9.1% in adult women and 5.1% in men.4 ED visits follow the same pattern, with a predominance of boys among children presenting to the ED with acute asthma5 and a predominance of women among adults.6
These life cycle differences suggest that reproductive hormones influence the development of asthma and its severity. In population based studies, rates of admissions to hospital for asthma are similar by sex in the early teenage years7,8 but three times higher in women than in men aged 20–50 years. This pattern continues until menopause when the incidence of asthma falls and equalises with men.8
Reproductive hormones may have beneficial or deleterious effects on women with asthma for unclear reasons.9 For example, differential effects of pregnancy on asthma are well described, with one third improving, one third remaining unchanged, and one third worsening.10,11 Female sex of the fetus exacerbates asthma during pregnancy.12 In contrast the anti-gonadotrophic androgenic agent danazol, or agents which induce a reversible menopause, gonadotrophic releasing hormone analogues, improve even severe menstrual asthma symptoms.13–15 Asthma exacerbation during the menstrual cycle might be a marker for the subset of patients who respond adversely to reproductive hormones such as oestrogen, progesterone, or anti-gonadotrophic hormones.
As early as the 19th century physicians began considering the menstrual cycle as a possible trigger for asthma.16 The hypothesis that hormonal fluctuations during the menstrual cycle might have a role in the pathophysiology of asthma has been advanced by several investigators.17–23 The results from two previously published studies were inconsistent as to the relation between phase of the menstrual cycle and ED presentation with asthma exacerbation.24,25 This study provides a much larger patient population than previous studies. The purpose of this prospective study was to determine if there is an association between phase of the menstrual cycle and both frequency of ED visits and the severity of the asthma exacerbation.
METHODS
The study was conducted at the Brooklyn Hospital Center emergency department between January 1997 and December 1999. Patients were enrolled and interviewed 24 hours per day, 7 days per week throughout the study period by trained research assistants. All acute asthma patients were screened for inclusion. Patients were asked the date of their last menstrual period during the triage process in the emergency department, whether they were pregnant, their medications such as birth control pills, and about surgical history such as hysterectomy. No other questions were asked about their menstrual cycle. Inclusion criteria were female sex, age 18–54, physician diagnosis of acute asthma, and last menstrual period within 28 days of the ED visit. Since the cycle was idealised to 28 days, patients were sorted into their respective menstrual phase based on the range from their last menstrual period. Patients were excluded if they were pregnant, on oral contraceptives, had a surgical or physiological menopause, or the visit was not their first ED visit for an asthma exacerbation during the study period.
Data collected about each study subject included demographic factors, past medical history (including asthma triggers and menstrual history), current medications, compliance, and details of the current asthma episode. Measures of asthma severity included history of intubation, oral steroids, or ED visit within the past year, initial peak expiratory flow (PEF), final PEF, and proportion admitted to the hospital.
As in two earlier studies,24,25 the menstrual cycle was assumed to have a duration of 28 days and women were divided into the following four categories with day 1 considered to be the onset of menstruation: preovulatory (days 5 to 11), periovulatory (days 12 to 18), postovulatory (days 19 to 25), and perimenstrual (days 26 to 4). Unique to this study, patients were classified into a phase based on two points in time: both the day of symptom onset and the day of the ED visit. Patients were excluded from that specific analysis if the date of symptom onset was missing (9%), or the date of symptom onset produced a cycle that was greater than 28 days or a cycle that was unable to be classified (91%). This resulted in a difference in sample size depending on method of classification (n = 560 for date of symptom onset, n = 792 for date of ED visit).
Statistical analysis
All analyses were performed using SPSS (Chicago, Illinois). Density of symptom onset (or ED visits) was plotted as a function of day of menstrual cycle using Splus 4.0 (MathSoft Inc, Seattle, WA). The χ2 goodness of fit test was used to assess the association between phase of the menstrual cycle and asthma exacerbation. We chose a priori that women would be distributed equally across the four phases of the menstrual cycle and the analysis was done to compare the actual proportions in the four phases to 0.25. All tests are two tailed with p values <0.05 considered statistically significant.
RESULTS
There were 4987 patient visits to the ED for an asthma exacerbation during the study period of which 3208 (64%) were women. A total of 2161 women were excluded because their menstrual period was longer than 28 days (n = 522), surgical or physiological menopause (n = 420), multiple visits (>2 ED visits, n = 729), oral contraceptives (n = 275), and no menstrual date listed (n = 215). Of the remaining 1047 women, another 255 were excluded because the present visit was the second visit to the ED for asthma during that menstrual cycle leaving 792 women with acute asthma. When the data were analysed including all ED visits (that is, more than one ED visit by a single patient), the results did not materially differ from results obtained with the dataset based on only the first ED visit. Moreover, there were no significant differences in mean age, race, median family income (based on home ZIP code), or percentage actively smoking between the study group and those excluded for the reasons cited above.
Figure 1 shows the relative proportion of ED visits according to phase of menstrual cycle when classified by either symptom onset or day of ED visit. The two methods of classification yielded similar results. Asthma exacerbations began more often during the preovulatory (28%) and perimenstrual phases (27%) of the cycle than in the periovulatory or postovulatory phases (p = 0.03). Likewise, ED visits occurred more commonly among women in the preovulatory (28%) and perimenstrual (27%) phases (p = 0.004). Figure 2 shows the density of ED asthma visits plotted as a function of the day of menstrual cycle.
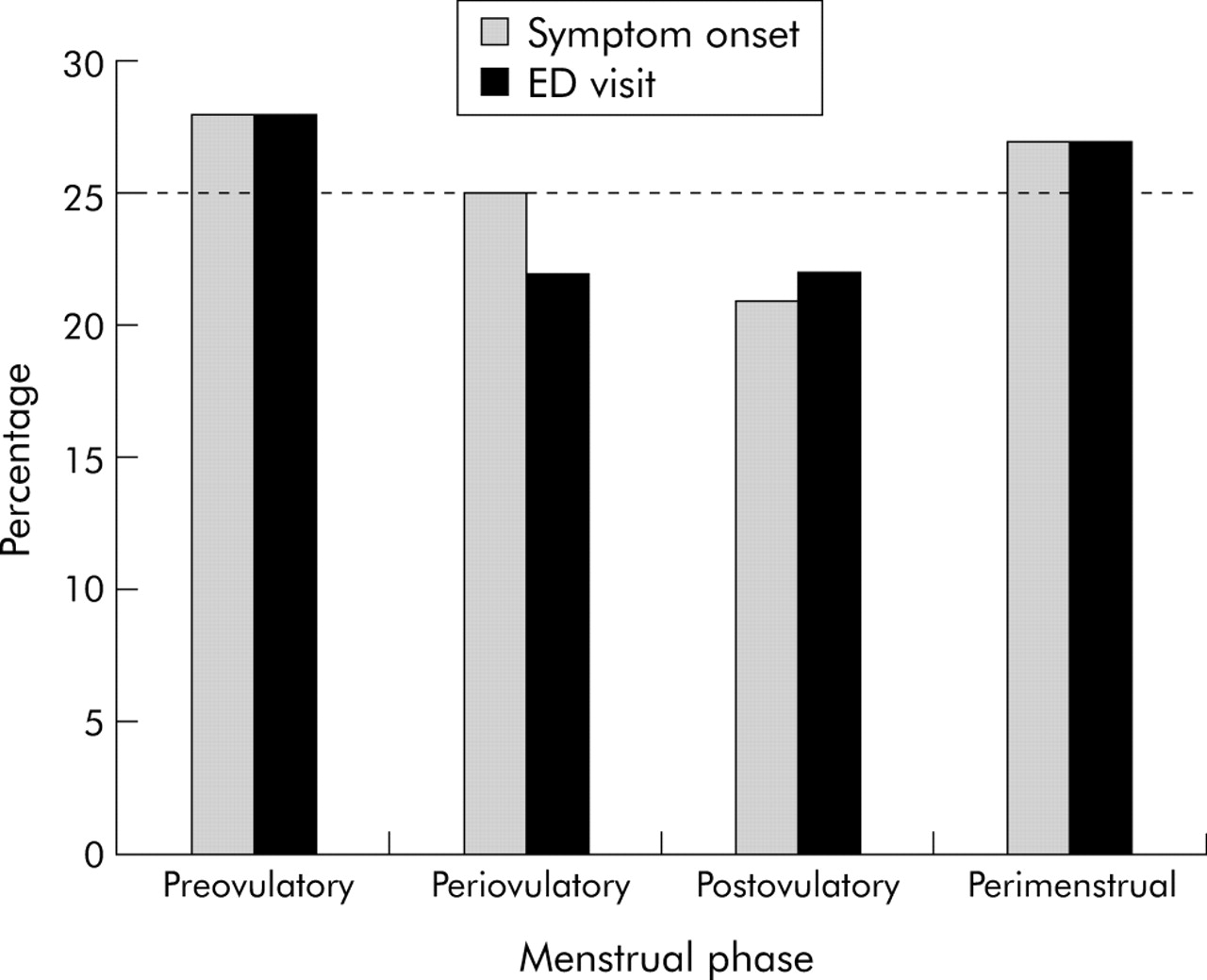
Menstrual phase on day of emergency department (ED) visit and day of symptom onset.

{kind=link}
{kind=link}
Emergency department (ED) visits for asthma. (A) Timing of ED visit for acute asthma in relation to blood hormone levels in idealised menstrual cycle (B).
Using either approach, there were no significant differences in demographic factors or in asthma severity of women according to menstrual phases. To facilitate comparison with prior studies,24,25 table 1 shows data according to date of ED presentation with acute asthma. There were no differences between the four phases of the menstrual cycle regarding income or percentage of active smokers.
Demographic factors and markers of asthma severity by phase of menstrual cycle; classified by date of emergency department visit
DISCUSSION
Our results show that ED visits for acute asthma are slightly more common during the preovulatory and perimenstrual phases of the menstrual cycle. This pattern was present whether the menstrual phase was estimated from the day of symptom onset or the day of the ED visit. These findings differ from Skobeloff et al24 who found that almost 50% of 182 ED visits for acute asthma occurred during the perimenstrual phase. Our results are more consistent with the recent study by Zimmerman et al25 on behalf of the Multicenter Airway Research Collaboration (MARC) investigators (www.emnet-usa.org). They found that only 21% of 288 ED visits for acute asthma exacerbation occurred in the perimenstrual phase, whereas 33% occurred in the preovulatory phase. In the present study involving 792 ED visits for asthma, we noted more modest increases in both the preovulatory (28%) and perimenstrual (27%) phases.
It is unclear whether the observed associations represent a hormonal effect on a certain subset of the female asthmatic population or the effect of confounding factors such as differential smoking, infection, or exposure to allergens. In the MARC study only 13% (95% CI 9 to 18) of women reported reproductive factors as personal asthma triggers.25 Exactly how the normal menstrual cycle (fig 1) interacts with the pathophysiology of asthma is unknown, but it seems clear that the initial ED study25 overstated the importance of perimenstrual asthma and the benefits of oestrogen. In some premenopausal women administration of oestradiol has decreased symptoms, cyclic variability in PEF, and airway reactivity.22,26 However, in postmenopausal women, oestrogen replacement therapy can cause worsening of some asthma symptoms.27 In addition, in non-asthmatic women, oestrogen replacement therapy is associated with an increased chance of developing asthma.28 Nevertheless, comparisons of endogenous hormonal fluctuations with exogenous hormonal administration require cautious interpretation; uncritical mixing of these concepts may contribute to apparent contradictions in the literature.
Objective evaluations of airway function during the menstrual cycle in women with stable asthma have yielded inconsistent results. Some studies have noted worsening symptoms and decreases in PEF in the premenstrual and menstrual period,17,18,20 while others found no changes in symptoms or spirometric parameters.29 Other studies found a discordance between symptoms and spirometric measurements during the menstrual cycle.20,21 In asthmatic women responsiveness to methacholine30 and adenosine monophosphate31 increases in the luteal phase (days 24 to 28) compared with the follicular phase (days 12 to 16) of the menstrual cycle.
Few studies have distinguished between women who report perimenstrual worsening of asthma and those who do not. In a prospective study Shames et al32 found increased use of bronchodilators and decreased morning PEF during the perimenstrual phase in women with reported menstrual asthma compared with women without menstrual asthma. However, daily symptom scores, evening PEF, differences in forced expiratory volume in 1 second between the luteal and follicular phases, and results of methacholine challenge were not significantly different for the two groups. Agarwal and Shah found significant cyclical differences in PEF in asthmatic women who perceived a menstrual linked deterioration which was not noted in women without such deterioration.23 In a small study Chandler et al22 noted that, although only a small percentage of patients noted a priori premenstrual exacerbations, all had a fall in PEF or exacerbation in symptoms which improved with oestradiol. This amelioration was not mediated, however, by β2 receptors since there was no change in β2 receptor density during the menstrual cycle in those with premenstrual asthma. Even if one considers that airway function worsens in the perimenstrual period, our data suggest that it does not result in more asthma exacerbations requiring acute medical care.
This study has some potential limitations. Although the sample size is relatively large, all the subjects were from one site in an urban location which may limit the generalisability of the findings. Two hundred and fifteen women were excluded because their menstrual data were missing. Only women with physiological reproductive cycle were included, so women with hysterectomies but intact ovaries were excluded as well as those on birth control pills. In addition, inaccurate reporting of the subjects’ last menstrual period could have resulted in misclassification of the phase of the menstrual cycle. Only laboratory analyses could provide more accurate classification and allow the inclusion of women with menstrual cycles longer than 28 days. Finally, we note the possibility that perimenstrual and preovulatory presentations with acute asthma may have been increased by the patients’ concomitant ingestion of aspirin or other analgesics that worsen asthma. We were unable to test this hypothesis, which merits further study.
In conclusion, our data do not support claims that asthma exacerbations markedly increase during the perimenstrual phase. It is possible that both preovulatory and perimenstrual phases may have some adverse impact. For specific subsets of women, these phases could be actual triggers of an asthma exacerbation or they might serve as “co-factors” that worsen other recognised triggers of acute asthma. These menstrual phase findings, together with a growing body of evidence for sex differences in asthma,5–9 support efforts to explore hormonal influences on asthma in women.
REFERENCES
Footnotes
-
Dr Camargo is supported in part by NIH grant AI-52338 (Bethesda, MD).
-
Competing interests: none declared.
Linked Articles
- Airwaves