Article Text

Abstract
Objective: To provide a comprehensive update of the clinical picture of lymphangioleiomyomatosis (LAM) using two large patient registries.
Methods: A cross sectional questionnaire survey which included questions on 14 LAM symptoms, pneumothorax, tuberous sclerosis complex (TSC), date of diagnosis, and pulmonary function tests (PFTs).
Results: The response rate was 70.5% (n = 328). The mean age at the time of the survey was 46.7 years. The mean age at diagnosis was 42.7 years for women diagnosed 1 year before the survey and 35.8 years for women diagnosed 10 years previously. The main symptoms were dyspnoea (74%), fatigue (72%), cough (47%) and chest pain (44%); younger patients (<40 years) were less likely to report dyspnoea (p = 0.02). Patients with TSC (n = 51) were less likely to report dyspnoea (p = 0.05) and 76.5% reported angiomyolipoma (p<0.0001) compared with patients with sporadic LAM. Patients with pneumothorax (63.0%) were less likely to report dyspnoea or fatigue (p⩽0.05) than patients without pneumothorax. PFT results showed that low forced expiratory volume in 1 second and carbon monoxide transfer factor were highly associated with dyspnoea (p<0.0001), but not with fatigue or history of pneumothorax.
Conclusion: Previously considered a condition of women of childbearing age, more older women (50% without pneumothorax) are now being diagnosed with LAM. LAM should be considered in women over 40 with unexplained dyspnoea. LAM patients with pneumothorax have less fatigue and less dyspnoea than those without pneumothorax. Fatigue has been overlooked as a symptom of LAM and appears across the spectrum of pulmonary function.
- AML, angiomyolipoma
- FEV1, forced expiratory volume in 1 second
- FVC, forced vital capacity
- LAM, lymphangioleio-myomatosis
- PFT, pulmonary function test
- RV, residual volume
- TLC, total lung capacity
- Tlco, carbon monoxide transfer factor
- TSC, tuberous sclerosis complex
- lymphangioleiomyomatosis
- tuberous sclerosis
- pneumothorax
- dyspnoea
- pulmonary function tests
Statistics from Altmetric.com
- AML, angiomyolipoma
- FEV1, forced expiratory volume in 1 second
- FVC, forced vital capacity
- LAM, lymphangioleio-myomatosis
- PFT, pulmonary function test
- RV, residual volume
- TLC, total lung capacity
- Tlco, carbon monoxide transfer factor
- TSC, tuberous sclerosis complex
Lymphangioleiomyomatosis (LAM) is generally described as a “rare disease affecting exclusively women of childbearing age”.1 While LAM is a systemic disease, the main manifestations are pulmonary, characterised by the presence of abnormal smooth muscle cells (LAM cells) that infiltrate the lungs and airways leading to lung cysts and pneumothoraces. Extrapulmonary features include renal angiomyolipomas (AML) and lymphangioleiomyomas.1–3 Currently there are no proven efficacious treatments for LAM; in advanced cases, supplemental oxygen and lung transplantation are options for patients.4,5 LAM occurs either in sporadic form (S-LAM) or in association with tuberous sclerosis complex (TSC-LAM). Women with TSC have a high incidence of LAM when screened by CT scanning.6–9 TSC and LAM are linked to mutations in the TSC1 and TSC2 genes.6,10
Since LAM is a rare disorder, most of the early clinical studies about LAM patients were small case reports. Recently, as more patients have been identified, clinical papers on LAM have been published from tertiary care centres around the world with larger numbers of patients.3,11–15 Given the increasing numbers of women being identified with the condition, it is timely to revisit the clinical picture of LAM. Case series in reports from tertiary care may not be representative of all LAM patients since local referral patterns and index of suspicion of LAM may vary. In this report we have used a different approach. We drew upon two large registries that include international groups of LAM patients to undertake the most comprehensive survey of LAM patients to date. This large sample allowed us to examine relationships across subgroups of LAM patients not previously possible. The main aims of the study were to determine whether previously reported series of LAM patients from tertiary centres (often involving small numbers of patients) truly reflect the clinical phenotype of the disease and to examine the clinical characteristics of the full range of patients. Specific questions guiding the research were:
-
Is LAM truly characterised as a condition of “women of childbearing age” or is the age spectrum changing?
-
Do patients with TSC-LAM have a different symptom profile from patients with sporadic LAM?
-
Does a history of pneumothorax alter the symptom and pulmonary function profile compared with those without a history of pneumothorax?
-
Are common symptoms of LAM reflected in respiratory function?
METHODS
Following ethical approval from the University of Toronto and Trent multicentre research ethics committees, a mailed questionnaire was sent to all women who agreed to be contacted by researchers in the US LAM Foundation database (n = 448) and women listed with the UK LAM Action (n = 59). Women listed were from the USA, UK, Canada and other countries. Participants were given stamped addressed envelopes to return the survey and the LAM Foundation and LAM Action removed any potential identifying information and returned the completed surveys to the researchers. To increase the response rate, non-respondents were mailed a second survey followed 3 months later by a postcard reminder. Participants were also asked to send copies of their most recent pulmonary function tests (PFTs).
The survey included questions on date of birth, age at diagnosis of LAM, age of first LAM symptoms, and whether the respondent had a diagnosis of TSC. Women were asked if they were currently experiencing any of 14 LAM associated symptoms or if they had a history of pneumothorax. We also enquired whether respondents had had any change in their symptoms over the past year (no change, symptoms got worse, symptoms got better). A more in depth examination of the relationship between dyspnoea and fatigue was also performed. The frequency of dyspnoea was determined (never, almost never, a little of the time, some of the time, a good bit of the time, most of the time, and all of the time). To measure fatigue, respondents were asked to mark their level of fatigue on a 10 cm visual analogue scale (VAS) with 1 = least fatigued/tired and 10 = most fatigued/tired.
Statistical analysis
We determined the distribution of age, TSC status and geographical residence for all participants, and the number and proportion of women who reported each symptom. The proportion of respondents with each symptom was calculated by age group (<40, 40–49, 50–59, and 60+ years), by TSC status, and by history of pneumothorax. Differences across age groups, TSC status and pneumothorax history were determined by χ2 test (p⩽0.05). Pulmonary function results by age group, TSC status, or presence/absence of symptoms were compared using t tests or analysis of variance (ANOVA).
The duration of LAM symptoms was calculated by the differences in current age from the age of first LAM symptoms. Duration of symptoms was classified as: <5 years, 5–10 years, and >10 years. Logistic regression was used to determine the association of pneumothorax with dyspnoea at rest, dyspnoea on exertion, and fatigue, controlling for TSC status and duration of symptoms. To determine the relationship between dyspnoea and fatigue we compared the distribution of the frequency of dyspnoea by the mean fatigue score (ANOVA, p<0.05).
For PFT results the mean, median and range for actual and percentage predicted values are reported. Not all women had each test so the sample size varies across PFTs. To test the relationship between PFT results and LAM symptoms we compared mean PFT values with dyspnoea on exertion, fatigue, and a history of pneumothorax (t test, p<0.05).
RESULTS
A total of 328 usable questionnaires were received (overall response rate 70.5%). Most respondents were from the US (63.7%); 14.9% were from the UK, 6.7% from Canada, and 14.6% from other countries. PFT results were received from 111 women. Of the respondents, 51 (16.0%) had been diagnosed with TSC. Sixty nine women (21.6%) had been evaluated for lung transplantation and 30 (10.0%) were on a waiting list. Ten women (3.1%) had received a lung transplant. 101 of the respondents (31.7%) used supplemental oxygen.
The mean (SD) age of the respondents was 46.7 (10.5) years (median 46.0; mode 44.0); 4.3% were aged <30 years, 22.6% were 30–39 years, 34.3% were 40–49 years, 27.8% were 50–59 years, 8.9% were 60–69 years, and 2.1% were >70 years. Age was moderately correlated with duration of LAM symptoms (r = 0.45, p<0.0001). The mean age varied significantly by country of residence (US 47.1 years, UK 47.3 years, Canada 51.4 years, other countries 42.0 years; p<0.0001). There was no difference in the proportion of TSC patients by country.
LAM and age at diagnosis
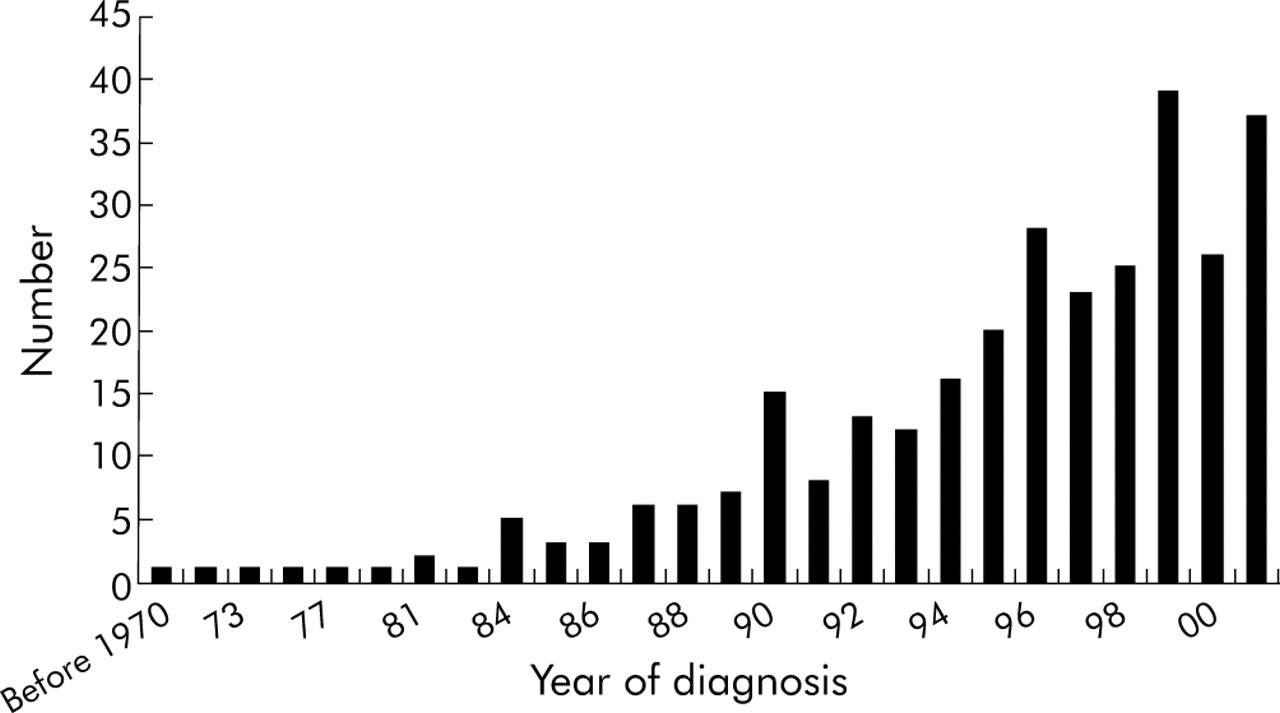
The number of women diagnosed with LAM who contacted the two patient registries increased markedly over the years (fig 1). There were many long term survivors: the proportion of women diagnosed within 1 year or less of the survey was 19.6%, 34.6% were diagnosed 2–5 years before the survey, 26.9% were diagnosed 6–10 years before the survey and 19.0% were diagnosed more than 10 years ago (table 1). The mean age of women diagnosed 1 year before the survey was 42.7 years compared with a mean age of 35.8 years for women diagnosed more than 10 years before the survey. For those in our study, prior to 1980 the mean age at diagnosis was 30.2 years (range 20–47). The mean age at diagnosis was 40.8 years for the US, 43.3 years for Canada, 38.9 years for the UK, and 35.5 years for other countries (p = 0.006). The age at diagnosis was significantly higher for the US and Canada than for other countries (p<0.05).
Time since diagnosis by age at diagnosis
{kind=link}
Number of LAM patients by year of diagnosis.
LAM symptoms
No change in symptoms over the past year was reported by 139 of the participants (43.6%), 142 (44.5%) reported worsening of symptoms, and 38 (11.9%) thought their symptoms had improved. Breathlessness with exertion was the most common symptom and was more common in older patients (p = 0.02, table 2). The next most common symptom (fatigue) did not differ by age. Other frequent symptoms were cough and chest pain; cough was reported more frequently by older patients (p = 0.06).
Reported signs and symptoms of LAM by age group (age at time of survey) and TSC status
Thirty eight percent reported having a kidney angiomyolipoma (AML). Other prominent symptoms included wheezing, abdominal bloating, and abdominal pain (more frequently in women aged 40–59 years; p = 0.06). Less commonly reported symptoms were abdominal pain, oedema of the arms or legs, coughing chyle, fluid in the chest/chylothorax, or weight loss; respiratory failure was seen infrequently. Twelve percent of respondents said they were short of breath never/almost never, 13.4% said a little of the time, 32.9% said some of the time, and 41.6% said a good bit of the time/all of the time. The duration of LAM was significantly related to the presence of several symptoms at the time of the survey—namely, dyspnoea on rest or exertion, wheezing, fatigue, and AML. The other symptoms were not related to duration of LAM.
Tuberous sclerosis complex (TSC)
Women with TSC presented a similar profile of signs/symptoms to those without TSC (table 2), with a few key differences. Women with TSC (mean age 42.9 years) were significantly younger than women without TSC (mean age 47.3 years; p = 0.006). The mean age at diagnosis for women with TSC (36.9 years) was also significantly younger than women without TSC (40.5 years; p = 0.02). The most frequently reported symptoms for patients with TSC-LAM were AML and fatigue. Women with TSC-LAM were less likely to report breathlessness on exertion (p = 0.05) and were more likely to claim oedema in the arms or legs (p = 0.006). Other symptoms occurred with similar frequencies. The mean number of symptoms (7.0) was slightly higher for women with TSC than for women without (5.3; p = 0.097).
History of pneumothorax
A history of pneumothorax was reported by 63.0% of women and was more common in younger patients (p = 0.008); only 50% of those aged ⩾60 years reported a pneumothorax compared with 77% of women aged <40 years. Seventy five percent of women diagnosed with LAM before 1994 had had a pneumothorax compared with 59.2% of women diagnosed after 1995 (p = 0.004). Of the respondents with a history of pneumothorax (table 2), 71.4% reported dyspnoea on exertion compared with 78.5% of women who did not have a pneumothorax (p = 0.07). After controlling for the presence of TSC and duration of symptoms (age), women with a pneumothorax were significantly less likely to report breathlessness on rest, dyspnoea on exertion, or fatigue (p<0.05, table 3).
Relationship between symptoms and history of pneumothorax, tuberous sclerosis complex (TSC), and duration of symptoms: logistic regression
Fatigue
The frequency of dyspnoea was significantly related to mean fatigue scores (table 4). The mean fatigue score was 1.7 for those reporting dyspnoea “never” and 6.9 for women reporting dyspnoea “all of the time” (p<0.0001). The correlation between dyspnoea and fatigue was 0.33 for the group. However, even LAM patients who reported dyspnoea “almost never” had a mean fatigue score of 4.6.
Relationship between dyspnoea and fatigue
Pulmonary function tests (PFTs)
The PFT results were as follows: mean forced expiratory volume in 1 second (FEV1) 67.4% predicted (range 19–128); mean forced vital capacity (FVC) 83.9% predicted (range 31–129); mean FEV1/FVC 61.9% (range 28–92); mean total lung capacity (TLC) 98% predicted (range 61–140); mean residual volume (RV) 122% predicted (range 57–294); mean RV/TLC 42% (range 23–73); mean single breath carbon monoxide transfer factor (Tlco,sb) 65.3% (range 15–116). These were lower than for age matched general female populations. The range of PFT values suggests that there is a spectrum of pulmonary function with some patients with LAM being in the normal range and others being severely limited.
The PFT results were significantly different for women who did and did not report dyspnoea with exertion (table 5). FEV1, FEV1/FVC, Tlco corrected for haemoglobin (Tlco,c) and Tlco,sb were significantly lower for women reporting dyspnoea with exertion and RV, TLC and RV/TLC were significantly higher. There was no difference in mean FVC % predicted. Women reporting fatigue had lower FEV1 % predicted values (p = 0.05), lower FEV1/FVC (p = 0.0017), and higher RV/TLC (p = 0.054); however other PFT values were not very different between women reporting and not reporting fatigue. There were no significant differences in PFT results between women with and without TSC (data not shown), but the number of respondents with TSC was low. Women with a history of pneumothorax had significantly lower values for FVC and TLC than women without pneumothorax.
Relationship between pulmonary function test (PFT) results, dyspnoea, fatigue, and pneumothorax
DISCUSSION
The main finding in this study is that more women over the age of 40 years are being added to LAM registries with the result that the mean age at diagnosis is increasing over time. The main symptoms of LAM in the study participants were dyspnoea with exertion and fatigue. While dyspnoea appears to be age related, the presence of fatigue is not; fatigue and dyspnoea are only moderately correlated (r = 0.33) and fatigue is a feature across the spectrum of respiratory function. Patients with TSC-LAM were younger and less likely to report dyspnoea with exertion. About 40% of women with LAM do not have a history of pneumothorax, especially among those who are older when diagnosed. Women with a history of pneumothorax are less likely to report dyspnoea or fatigue. There was a significant relationship between FEV1 and Tlco and dyspnoea on exertion, but not with the presence of fatigue or a history of pneumothorax.
Although this is the largest study of LAM patients reported to date, it is not possible to determine definitively if the findings of this study are applicable to all patients with LAM. Patients worldwide are listed with the US LAM Foundation and UK patients are listed with the UK LAM database, but non-English speaking women from other countries are not included. The large number of respondents strongly implies that the study patients are descriptive of the general population of LAM patients.
CT scanning is increasingly used for diagnosis and a higher index of suspicion among physicians in pulmonary medicine means that the picture of the “typical LAM patient” is changing. The most dramatic presentations of pneumothorax during pregnancy or air travel are still found but, in recent years, LAM no longer fits the description in the seminal article by Taylor et al:16 “women of childbearing age present with a spontaneous pneumothorax, chylothorax, hemoptysis, and slowly progressive dyspnoea”. As more patients are identified, LAM is becoming equally a condition of women aged 45–60 years (in this study the modal age was 44 years) and, among the older age groups, fewer women had a history of pneumothorax. This age distribution of women with LAM suggests that the former description of “women of childbearing age” needs to be amended and broadened to include women in their middle years.
It is possible that women who had LAM before 1995 have died and therefore this cross sectional study would not include these women. If this were the case, then the mean age of diagnosis before 1995 would be higher. However, since there is no registry of deaths for women with LAM, we do not know the magnitude of such a possibility. We cannot state that the incidence of LAM is increasing. A more likely scenario is that, in the past, women who had LAM but did not meet the “classic profile” of being of childbearing age presenting with pneumothorax were either not diagnosed at all or were incorrectly labelled as asthma or emphysema. For women under 40 years of age without a catastrophic incident such as a pneumothorax or problem pregnancy, it is unlikely that LAM would have been suspected. Women over 40 years of age may have had asymptomatic LAM for many years and it is only when sufficient lung tissue is destroyed that these women sought medical attention for dyspnoea. It is possible that only in the current climate of newer diagnostic techniques and a higher index of suspicion are women over 40 who present with dyspnoea without pneumothorax being increasingly recognised as having LAM. Furthermore, the differential mortality rate among women with LAM and the length of time undiagnosed will need to be considered in determining the true incidence of LAM.
The second most frequently reported symptom in this study (fatigue) is not mentioned in previous clinical descriptions of LAM.1,12,17–19 In our study fatigue was reported by a high number of patients and was the most frequent symptom for older patients and those with TSC. It was reported by LAM patients of all age groups and, unlike dyspnoea, was not strongly related to PFT results; this suggests that fatigue is independent of pulmonary function in LAM. Moreover, even women with LAM reporting a low frequency of breathlessness had high fatigue scores.
Fatigue is a common feature of chronic diseases and occurs at higher rates than in control populations.20 The presence of fatigue was found to reduce the quality of life for patients with chronic obstructive pulmonary disease.21 In fact, many patients with chronic disease list fatigue as their most troubling symptom.22 Fatigue is a symptom that needs to be seriously considered for LAM patients as it affects one’s motivation, concentration, and everyday activities of living,23 and research is needed on how to reduce fatigue for patients with LAM.
Our finding of a much higher proportion of TSC-LAM patients in the study with AML compared with non-TSC patients may be a reflection of the fact that not all patients with LAM are screened for AML Although LAM and TSC were known to coexist for many years, recent studies have shown that 20–40% of adult women with TSC may have LAM, although the majority of these are asymptomatic.6–8 Clinicians seeing patients with TSC are now being advised to check their patients for pulmonary LAM.7,9 If more TSC patients were screened, then they would be diagnosed with LAM at an earlier (asymptomatic) phase and this would explain our findings that TSC patients were younger and less likely to have dyspnoea than non-TSC patients. The TSC patients in this study are, for the most part, probably those with symptomatic lung disease or those who have already been “screened” for LAM and have therefore contacted the LAM Foundation or UK LAM Action.
Another finding in this study was that a history of pneumothorax was not associated with dyspnoea and fatigue, even after considering age and duration of LAM symptoms. It is possible that pneumothorax per se is not leading to increased breathlessness in many women with LAM. The reasons for this are unknown and this finding requires further study. Participants who reported a history of pneumothorax had lower FVC predicted and lower TLC predicted than women without pneumothorax. This may be the result of pleural interventions such as pleurectomy causing a restrictive process to lung expansion.
The main PFT abnormalities reported in previous series were reduced FEV1 and transfer factor.19,24,25 This was also true in our study. However, pulmonary function varied widely with some having normal or near normal PFT values while others were severely impaired. PFT results were significantly worse in patients reporting dyspnoea on exertion than in those who did not report dyspnoea.
This is the largest survey of LAM patients to date and illustrates the clinical variability of this disease. There are four main findings from this study. (1) More women over 40 years are being diagnosed with LAM often without “classical” features such as pneumothorax; the reason for this is unknown but may reflect the increased index of suspicion among pulmonary physicians and the use of newer diagnostic tests. LAM should no longer be considered exclusively a disease of young women, but also a condition affecting women in their middle years. (2) Fatigue is an overlooked common symptom among LAM patients; it affects the quality of life of patients with chronic disease and research is needed to help explain and decrease fatigue among LAM patients. (3) The women in this survey with TSC-LAM had more LAM symptoms, were younger than non-TSC women, were more likely to have AML, and were less likely to have dyspnoea on exertion. This strengthens the recommendation that LAM patients should be screened for AML and that TSC patients should be screened for LAM. (4) PFTs showed a pattern of reduced FEV1, increased RV, and decreased Tlco, similar to other studies. However, this study is the first to show the relationship between patient reported symptoms and PFT results.
Acknowledgments
The authors are grateful to Professor Anne Tattersfield for cooperation in using the UK LAM database.
REFERENCES
Footnotes
-
Published Online First 29 July 2005
-
This study was funded by the LAM Foundation, Cincinnati, USA and a doctoral fellowship award to SPB from the Social Sciences & Humanities Research Council of Canada. The LAM Foundation kindly provided access to their patient database but had no involvement otherwise in the research.
-
Competing interests: none declared.