Article Text

Abstract
Background Pseudomonas aeruginosa chronic pulmonary infection is an unfavourable event in cystic fibrosis. Bacterial clearance is possible with an early antibiotic treatment upon pathogen isolation. Currently, no best practice exists for early treatment. The efficacy of two different regimens against initial P aeruginosa infection was assessed.
Methods In a randomised, open-label, parallel-group study involving 13 centres, the superiority of inhaled tobramycin/oral ciprofloxacin compared with inhaled colistin/oral ciprofloxacin (reference treatment) over 28 days was evaluated. Patients were eligible if they were older than 1 year with first or new P aeruginosa isolation. Treatments were assigned equally by centralised balanced randomisation, stratified by age and forced expiratory volume in 1 s values. The participants and those giving the intervention were not masked to arm assignments. The primary endpoint was P aeruginosa eradication, defined as three successive negative cultures in 6 months. Analysis was by intention to treat. This trial was registered with EudraCT, number 2008-006502-42.
Results 105 patients were assigned to inhaled colistin/oral ciprofloxacin (arm A) and 118 to inhaled tobramycin/oral ciprofloxacin (arm B). All patients were analysed. P aeruginosa was eradicated in 66 (62.8%) patients in arm A and in 77 (65.2%) in arm B (OR 0.90, 95% CI 0.52 to 1.55, p=0.81). Following treatment, an increase in Stenotrophomonas maltophilia was noted (OR 3.97, 95% CI 2.27 to 6.94, p=0.001) with no differences between the two arms (OR 0.89, 95% CI 0.44 to 1.78, p=0.88).
Conclusions No superiority of treatment under study was demonstrated in comparison to the reference treatment. Early eradication treatment was associated with an increase in S maltophilia.
- P aeruginosa
- cystic fibrosis
- early eradication treatment
- inhaled antibiotics
- aspergillus lung disease
- bacterial infection
- cystic fibrosis
- opportunist lung infections
- paediatric lung disease
- respiratory infection
- bacterial infection
- clinical epidemiology
- cystic fibrosis
Statistics from Altmetric.com
- P aeruginosa
- cystic fibrosis
- early eradication treatment
- inhaled antibiotics
- aspergillus lung disease
- bacterial infection
- cystic fibrosis
- opportunist lung infections
- paediatric lung disease
- respiratory infection
- bacterial infection
- clinical epidemiology
- cystic fibrosis
Key messages
What is the key question?
-
To clarify the efficacy of two different eradication treatments, oral ciprofloxacin and inhaled tobramycin (test treatment), compared with oral ciprofloxacin and inhaled colistin (reference treatment) over 28 days against initial Pseudomonas aeruginosa infection in cystic fibrosis.
What is the bottom line?
-
To date, there is no clearly identified best practice for early treatment of P aeruginosa infection.
Why read on?
-
To verify the efficacy of test treatment compared with reference treatment in eradicating P aeruginosa, increasing forced expiratory volume in 1 s values and modifying airways flora.
Introduction
Chronic pulmonary infection by Pseudomonas aeruginosa is an unfavourable event in patients with cystic fibrosis (CF) associated with an increase in morbidity and mortality. Once chronic infection is established, P aeruginosa is virtually impossible to eradicate.1–4 However, various studies have shown that bacterial clearance from the respiratory tract is possible with early antibiotic treatment upon isolation of this pathogen,4–16 so aggressive antibiotic treatment of initial P aeruginosa infection is now recommended.2 Several strategies exist to treat early P aeruginosa infection using inhaled colistin with oral ciprofloxacin or inhaled tobramycin or intravenous antibiotics.1–17 To date, there is no clearly identified best practice for early treatment of P aeruginosa infection. Few studies have compared the efficacy of different treatments.1 ,6 ,7 ,10 ,14–16 The ELITE trial compared the efficacy of a 28-day regimen with a 56-day regimen of inhaled tobramycin and showed no differences.10 The EPIC study investigated the efficacy of four anti-pseudomonal regimens in children aged 1–12 years with recently acquired infection. No difference was found between cycled and culture-based therapies. Adding oral ciprofloxacin produced no benefits.17
The primary aim of this multicentre, randomised study was to evaluate the efficacy of two different eradication treatments (oral ciprofloxacin and inhaled tobramycin compared with oral ciprofloxacin and inhaled colistin) over 28 days against initial P aeruginosa infection. Eradication is defined as three negative cultures within a 6-month period.3
The secondary aims were to verify if the treatment is equally effective in patients with first-ever P aeruginosa infection and previously treated patients; to evaluate FEV1 at baseline and following treatment; to determine if differences exist between the two types of treatment referring to the P aeruginosa-free period; and to determine whether the eradication treatment is associated with the emergence of Burkholderia cepacia complex, other non-fermenter Gram negatives and Aspergillus spp.
Methods
This was a multicentre, open-label, parallel-group study to evaluate the superiority of inhaled tobramycin and oral ciprofloxacin compared with inhaled colistin and oral ciprofloxacin considered as the reference treatment for eradication.3 ,4 ,6 ,12 ,18
Patients in regular clinical and microbiological follow-up were considered eligible if older than 1 year with first or new P aeruginosa infection. New infection was defined as P aeruginosa isolation following bacterial clearance documented by three negative cultures in the previous 6 months.3
CF diagnosis was based on clinical features of the disease and concentration of chloride in sweat >60 mmol/litre.1–3
Exclusion criteria were concomitant infection by other non-fermenter Gram negatives, respiratory exacerbations, P aeruginosa resistance to any of the antibiotics used in the study, concomitant use of quinolones, chronic macrolide use, abnormal kidney or liver function tests.
Thirteen CF Centres participated in this trial. The study received ethical approval from the Meyer Hospital Ethics Committee and was registered with EudraCT, number 2008-006502-42.
Randomisation
A balanced randomisation sequence was created using statistical software to assign treatments within permuted blocks of size 10. Randomisation assignment was organised by email. Patients were allocated 1:1 and distributed into two groups, stratified according to age and FEV1 values as an expression of illness severity:
-
age 1–5 years
-
age >5–12 with FEV1 <70%
-
age >5–12 with FEV1 >70%
-
age >12 with FEV1 <70%
-
age >12 with FEV1 >70%.
The people involved in randomisation and in the treatment assignments were kept separate.
Procedures
Microbiological analyses were performed following published literature.19 Strain typing in the case of next P aeruginosa isolation was performed with repetitive PCR.20 FEV1 values were measured according to American Thoracic Society–European Respiratory Society standards.21
Patients received one of the two types of treatments for 28 days: twice-daily inhalation of 2 000 000 IU colistin and 30 mg/kg/day of oral ciprofloxacin, divided into two doses (arm A or active comparator) or twice-daily inhalation of 300 mg tobramycin solution for inhalation and 30 mg/kg/day of oral ciprofloxacin divided into two doses (arm B or test treatment). Colistin was reconstituted immediately before use and administered in isotonic solution (two phials of 1 000 000 IU in 2 ml of water for injections plus 2 ml of 0.9% sodium chloride).3 Tobramycin solution for inhalation was dispensed as a ready-to-use solution in either 300 mg/5 ml or 300 mg/4 ml phials. This trial was conducted using jet nebulisers.3
Each physician in the respective centre provided the patients' clinical management, according to standards of care.18 The treatment was suspended in the case of adverse effects or pulmonary exacerbation.22
Nebulisers and drugs for treatment were covered by the Italian Health Service at no charge to the patients.
Outcomes
Treatment efficacy was evaluated according to the UK CF Trust criteria.3 Results of cultures and clinical records were used to assess secondary aims. P aeruginosa microbiological status was evaluated using the Leeds criteria23 after a median follow-up time of 16 months since recruitment.
Statistical analyses
This trial was designed calculating the sample size as a balance between statistical considerations and experience regarding epidemiology of first or new P aeruginosa infection.24 We calculated sample size assuming 65% response to early eradication treatment lasting 4 weeks in the active control arm. We hypothesised recruiting 200 patients in a 2-year trial. The α (type I) error was set at 0.05, the β (type II) error at 70%. A 13% greater rate of eradication in arm B in comparison with arm A was considered as the level of superiority.
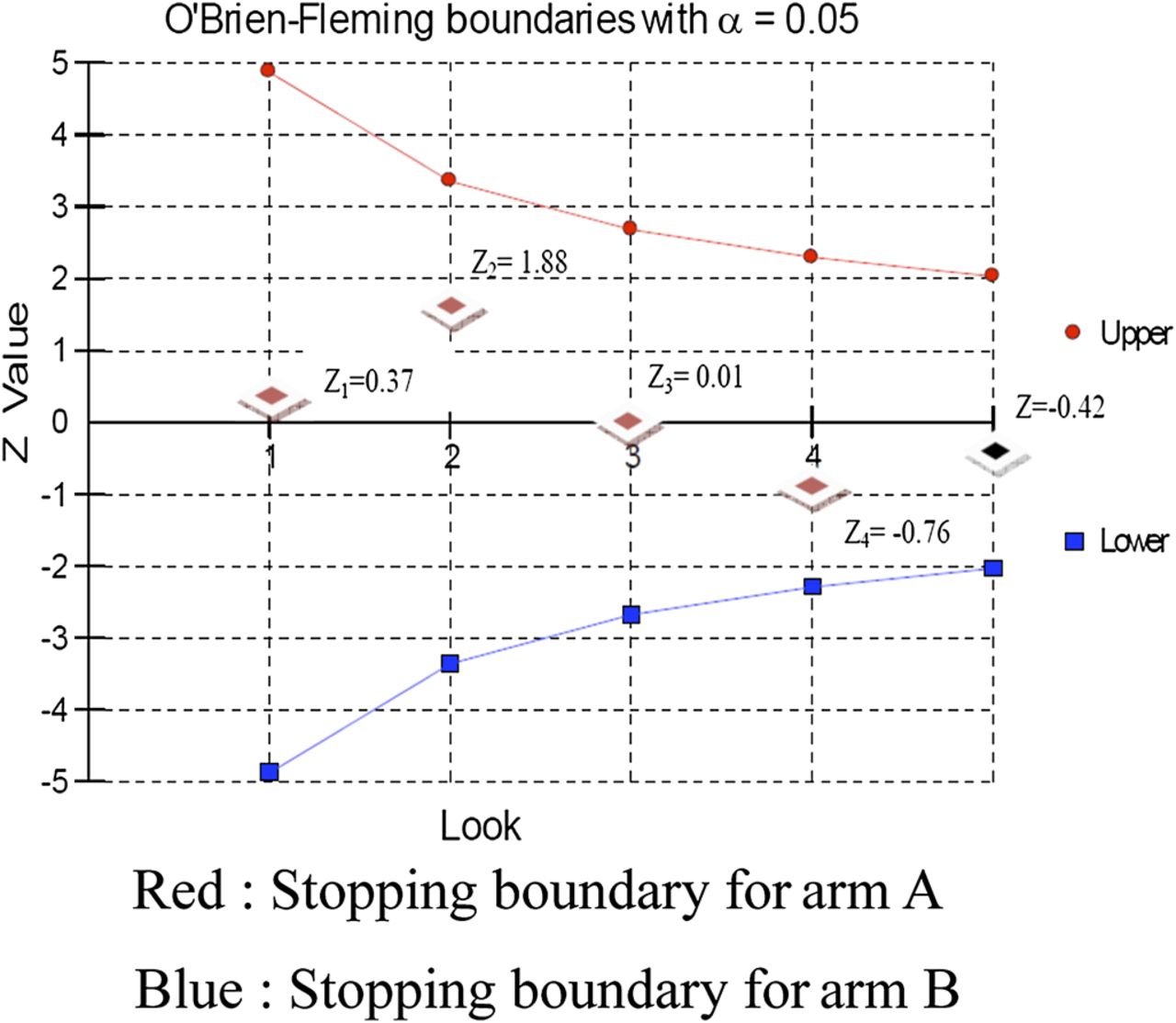
In relation to the primary aim of the study (bacterial eradication), a sequential statistical analysis using O'Brien-Fleming boundaries was used to determine the appropriate rules for trial interruption.24 Four interim analyses (every 6 months) were planned before the start of the trial. The results of the interim analyses were presented to the Data Safety Monitoring Board overseeing the study to consider the option of early termination. The association of patients' baseline demographical and clinical characteristics on the primary outcome was evaluated using a test for interaction. For all subgroup analyses, unadjusted OR and relative 95% CI were used as a measure of treatment effect. Data regarding the primary aim was independent, with one observation per participant, and evaluated according to intention-to-treat analysis.24
For secondary aims, differences in continuous and categorical variables between groups were evaluated using descriptive statistics, χ2 test, and t test. P aeruginosa-free time after treatment was calculated according to the Kaplan–Meier product-limit method. Comparisons of estimated P aeruginosa-free curves were performed by means of the log-rank test. HRs and appropriate 95% CIs were also calculated by means of Cox's proportional hazard model.
Results
Figure 1 shows the trial profile. A total of 263 patients were assessed for eligibility in the period from 1 February 2008 to 31 March 2010 and 223 patients were randomised—105 (47.1%) patients were assigned to arm A (oral ciprofloxacin and inhaled colistin) as active controls and 118 (52.9%) patients were assigned to arm B (oral ciprofloxacin and inhaled tobramycin) as test treatment. Two patients in each arm refused the treatment after randomisation. Table 1 shows patients' clinical characteristics.
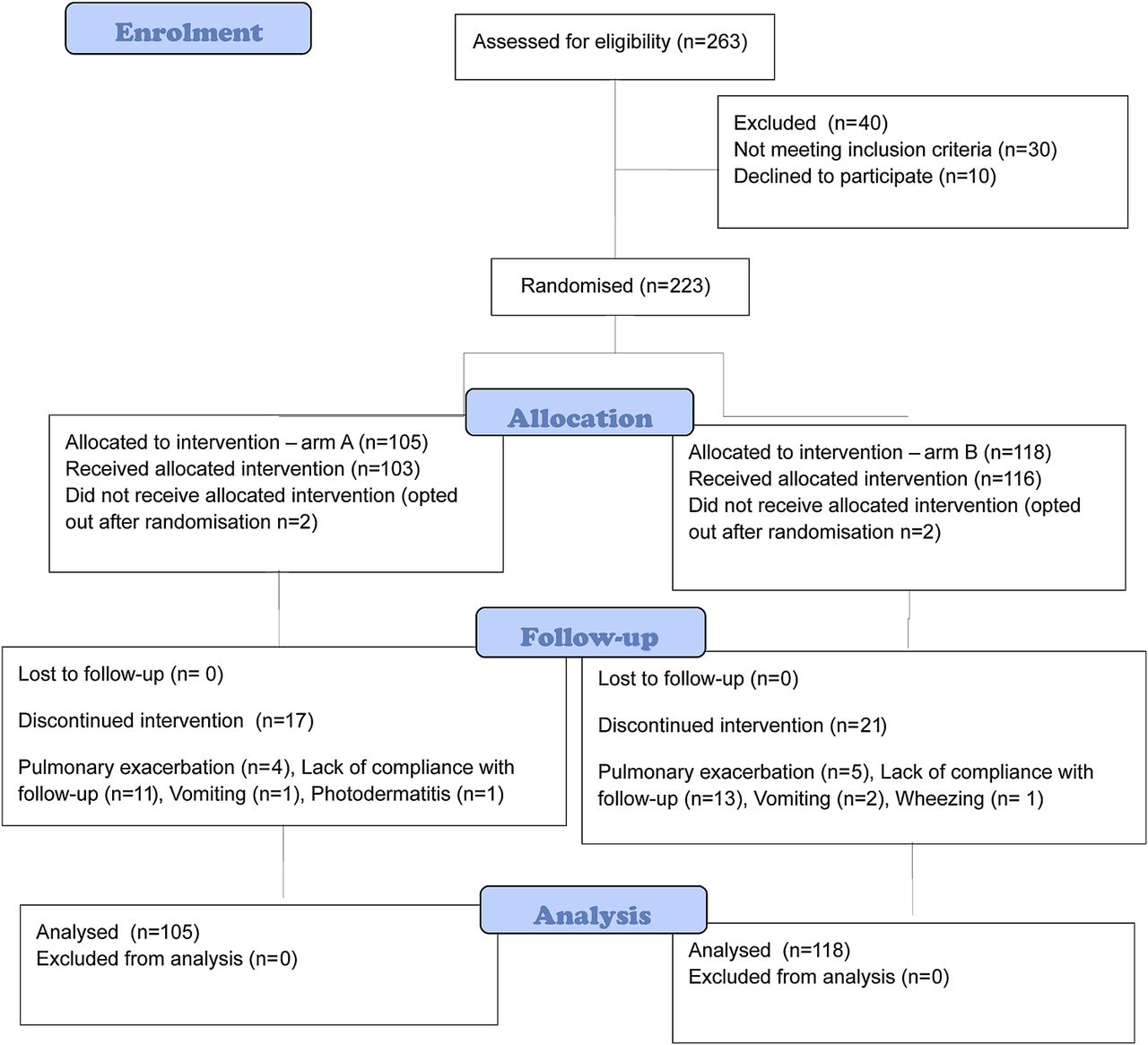
Trial profile.
Baseline demographic and clinical characteristics of patients
Microbiological cultures were performed on pharyngeal swab specimens in 132 of 223 patients (59.2%) and sputum in 91 of 223 patients (40.8%). At baseline, P aeruginosa phenotype was non-mucoid and all strains were susceptible to ciprofloxacin, colistin and tobramycin.
One hundred and twenty-one of 223 patients (54.3%), 57 in arm A and 64 in arm B, had first-ever P aeruginosa infection while 102 (45.7%), 48 in arm A and 54 in arm B, had previously had P aeruginosa infection cleared with early eradication treatment. The age (mean ± SD) of patients with first-ever P aeruginosa infection was significantly lower than in patients who had undergone previous eradication treatment (7.89±7.4 years; 11.33±8.5 years; difference: 3.44, 95% CI −5.54 to 1.34, p=0.001). For the age (mean ± SD) at first-ever P aeruginosa infection, we observed no statistically significant difference between females and males (7.12±5.7 years; 8.51±8.5 years; difference: 1.39, 95% CI −3.31 to 0.53, p=0.15).
One hundred and twenty-eight of 223 patients (57.3%) 5 years or older, 60 in arm A and 68 in arm B, were able to perform spirometry.
Thirty-eight of 223 randomised patients (17%) dropped out of the study. Causes of dropout are shown in table 2.
Adverse events leading to treatment discontinuation and other causes of dropout per arm
Primary endpoint
P aeruginosa was eradicated in 66 of 105 patients (62.8%) in arm A and in 77 of 118 patients (65.2%) in arm B. The proportion of P aeruginosa eradication between the two groups was not statistically significant (OR 0.90, 95% CI 0.52 to 1.55, p=0.81).
The results of interim analyses and the final analysis are shown in figure 2.
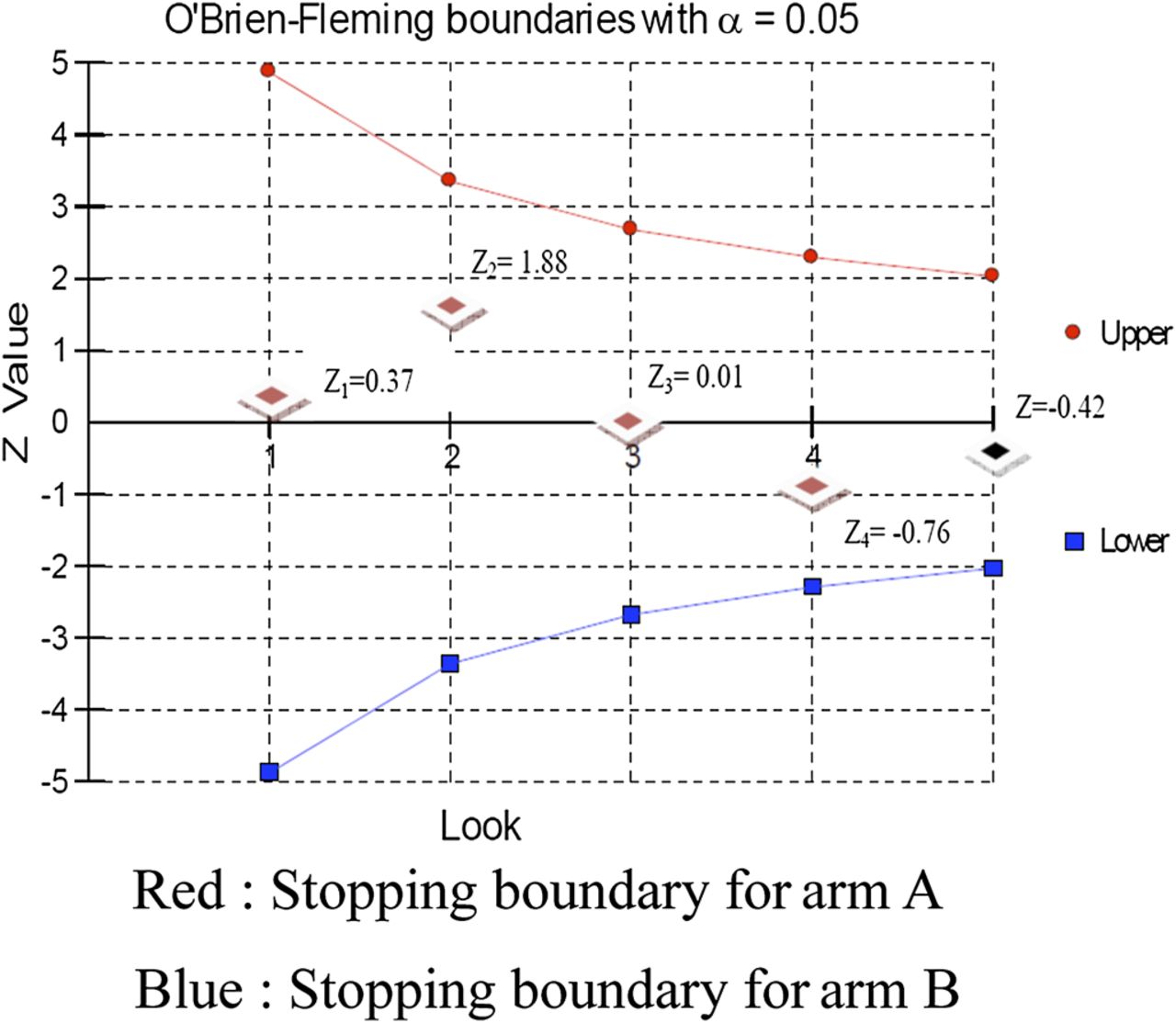
Sequential analysis graph showing results of four interim analyses and the final analysis.
Treatment result by age and FEV1 values is shown in table 3. We observed no statistically significant difference in P aeruginosa eradication in the strata considered (Pearson χ2=4.45, p=0.35).
Intention-to-treat analysis by strata
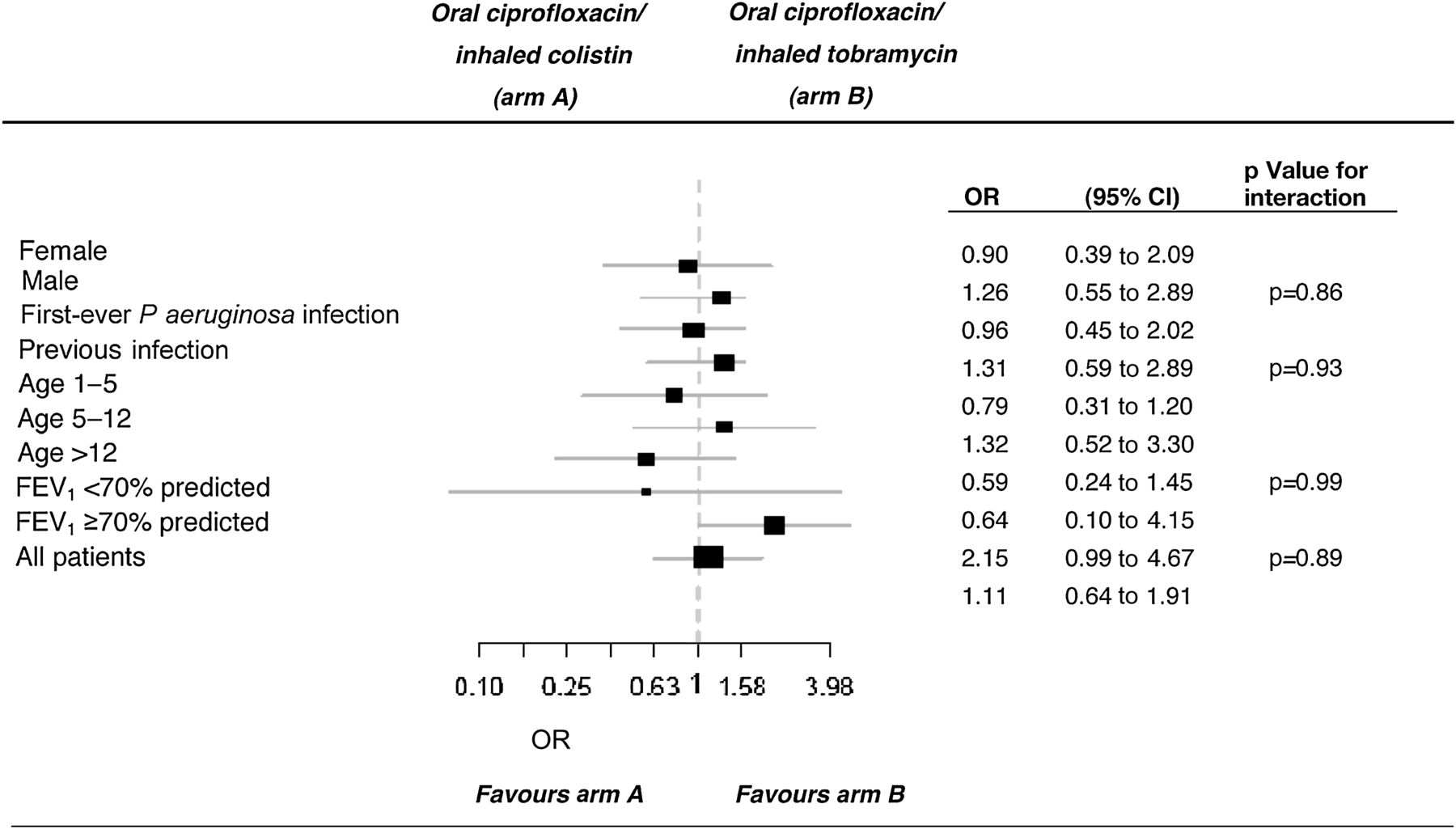
Subgroup analyses are reported in figure 3. In patients with FEV1 > 70%, the proportion of P aeruginosa eradication was higher although not statistically significant in patients in the test treatment arm in comparison to the active control arm (unadjusted OR 2.14, 95% CI 0.99 to 4.67, p=0.07).

{kind=link}
{kind=link}
{kind=link}
Subgroup analyses of variables among patients receiving oral cipofloxacin and inhaled colistin (arm A) compared with those receiving oral ciprofloxacin and inhaled tobramycin (arm B). FEV1, forced expiratory volume in 1 s.
Secondary endpoints
Effectiveness of treatment
At the end of the follow-up period, having performed cultures and patients' clinical examination at 2, 4 and 6 months, early eradication treatment was found to be effective in 80 of 121 patients (66.1%) with first-ever P aeruginosa infection (failure in 41 patients) and in 63 of 102 patients (61.7%) who had successfully undergone early eradication treatment (failure in 39 patients). Difference was not statistically significant (OR 1.20, 95% CI 0.69 to 2.09, p=0.59).
FEV1 change following treatment
Following treatment, after a mean time of observation of 54±39 days, the mean FEV1 (±SD) relative change (percentage of predicted) from baseline was 2.15% (±8.50) in arm A and 4.55% (±11.54) in arm B (p=0.18).
Period in which patients remained P aeruginosa free
After 6 months 143 of 223 patients (64.1%) were P aeruginosa free, 66 in arm A and 77 in arm B (HR 0.95, 95% CI 0.58 to 1.56 p=0.85).
Table 4 illustrates the percentage of P aeruginosa-free patients for each of the three cultures following early treatment in both arms of the study in a 6-month range.
Treatment failure at first, second and third culture for treatment arm
Molecular analyses were performed on paired P aeruginosa samples isolated from 47 patients at baseline and within a 6-month period following treatment. The same P aeruginosa genotype was found in isolates from 36 patients, a different genotype in isolates from 11 patients.
Post-trial follow-up: emergence of other non-fermenter Gram negatives and Aspergillus spp in patients' airways
The post-trial follow-up was completed in 205 of 223 randomised patients (91.9%) (missing data: 18 patients, 8 in arm A and 10 in arm B). After a median observation period of 16 months (range 12–28), 135 patients (60.5%), 61 in arm A and 74 in arm B, were still P aeruginosa free, 56 (25.1%), 28 in arm A and 28 in arm B, were intermittently infected and 14 (6.3%), 8 in arm A and 6 in arm B, chronically infected.
We evaluated the isolation frequency of other Gram-negative pathogens and Aspergillus spp during a period of 16 months (median) pre/post treatment. Following treatment, Stenotrophomonas maltophilia was found in 40 patients (17.9%) and Achromobacter xylosoxidans in 14 patients (6.2%). We observed no emergence of B cepacia complex. Table 5 illustrates the increase in isolation frequency of S maltophilia and A xylosoxidans in the airway cultures of 54 patients in the pre/post observation period indicated above. While the isolation frequency of A xylosoxidans appeared substantially unvaried, following treatment we observed an increase in S maltophilia isolations (OR 3.97, 95% CI 2.27 to 6.94, p=0.001). Twenty-five of 80 S maltophilia isolations (31.3%) were observed in arm A and 55 (68.7%) in arm B.
Isolation frequency of Stenotrophomonas maltophilia and Achromobacter xylosoxidans in the cultures of 54 patients in a median time of observation pre and post-treatment of 16 months
Aspergillus spp isolates were found in 20 patients (8%) before treatment and in 31 (14%) after treatment (OR 1.63, 95% CI 0.90 to 2.97, p=0.13).
In the 205 patients completing follow-up there were 52 Aspergillus spp positive cultures of 1025 in the pre-observation period and 59 of 1237 in the post-observation period (OR 1.06, 95% CI 0.72 to 1.56, p=0.81).
As shown in table 6, no statistically significant differences were observed in the emergence of non-fermenters and Aspergillus spp in the two treatment arms (S maltophilia, OR 0.89, 95% CI 0.44 to 1.78, p=0.88; A xylosoxidans, OR 1.52, 95% CI 0.51 to 4.57, p=0.62; Aspergillus spp, OR 0.47, 95% CI 0.21 to 1.07, p=0.10).
Post-trial follow-up (completed in 205 patients): microbiological status for Stenotrophomonas maltophilia, Achromobacter xylosoxidans and Aspergillus spp in the two arms
Discussion
The present study is a comparison of two different schedules of early eradication regimens of inhaled antibiotics associated with oral ciprofloxacin in the treatment of initial P aeruginosa infection. No superiority of the treatment under study was demonstrated when compared with the reference treatment. A follow-up conducted using three cultures per patient over 6 months showed no differences between the two arms in relation to the period in which patients remained P aeruginosa free. Patients previously treated with early eradication treatment had the same microbiological outcome compared with patients with first-ever infection. Early eradication treatment is associated with an increase in S maltophilia in the airways. The high percentage of patients receiving intervention considering the number assessed for eligibility indicates treatment acceptability. The dropout percentage was due more to the lack of compliance with microbiological follow-up than to the treatment itself.
A large number of P aeruginosa infections occurred in the 1–5 age range, as shown by other studies.16
P aeruginosa strains isolated at baseline were susceptible to antibiotics. Only a small percentage of bacterial strains associated with initial infection are resistant to antibiotics.3 ,25 However, as susceptibility in early isolates cannot be presumed, susceptibility tests should continue to be performed to assist the choice of treatment.26
We observed no differences in the primary outcome between patients with first-ever P aeruginosa infection and patients previously treated. This underlines the importance of paying great attention in the initial phases of infection, even in previously treated patients.
The eradication rates in both arms of the study were lower than some other published trials. Eradication rates are not easily comparable as many differences exist in the literature regarding study design, schedule and length of eradication treatments, follow-up period, methods used to collect airway specimens, patients' clinical characteristics and definition of eradication.1–17 In our study the analysis was by intention to treat, which may have affected the percentage of eradication.24 Moreover, patients included in this trial were treated using a single cycle of antibiotics. Experiences published in the literature underline a greater efficacy of oral ciprofloxacin and inhaled colistin when treatment is extended to 3 months.4 ,12 ,27 Recent studies conducted only with inhaled tobramycin showed no improvement in the microbiological outcome when treatment length was extended from 28 to 56 days.10 It is debatable whether such contrasting results for the microbiological outcome after treatment extension depend on associated use of antibiotics rather than using a single drug. The evaluation of treatments beyond 28 days is not included in the aims of the present study.
Following treatment, we observed an increase in FEV1 values in both arms. Limited data exist about the efficacy of early eradication treatment in preventing lung function decline.4 ,10 ,12 A longer follow-up is required to evaluate the effect of this treatment on lung function. Moreover, considering that pulmonary function testing cannot usually be performed on children under 5 years, FEV1 may not be the ideal marker to evaluate lung function in eradication trials.17
Our data confirm that next P aeruginosa isolation within 6 months from the eradication treatment is mainly due to treatment failure.3 The possibility that after early eradication treatment next P aeruginosa infections could be due to different P aeruginosa strains is described in the literature, indicating the efficacy of treatment.8 ,10 ,12 ,28 Considering that molecular typing techniques are not easily carried out in clinical practice, culture results remain the standard for evaluating treatment efficacy.
We observed no substantial differences in the primary outcome regarding sex, patient age and stratification by age and FEV1 values. In the subgroup analyses we observed a trend in arm B towards a greater efficacy in P aeruginosa eradication in patients with FEV1 values >70% of predicted. A higher effectiveness of nebulised tobramycin in comparison with colistin has been described as improving lung function in patients with chronic P aeruginosa infection.29 ,30 The results of such studies cannot be generalised to the treatment of early phases of P aeruginosa infection.
The clinical meaning of the emergence of other non-fermenter Gram negatives has yet to be established. Data regarding A xylosoxidans are limited19 and as far as S maltophilia is concerned, contrasting opinions exist about pathogenicity.31–33 The causes of the increased isolations of non-fermenter Gram negatives are not clear. It has been hypothesised that selective pressure exerted on bacterial populations by aerosolised aminoglycosides could determine the emergence of S maltophilia, but results from previous studies are contrasting. While the ELITE trial showed no S maltophilia increase during the follow-up, the EPIC trial observed the emergence of the pathogen in up to 20% of patients.10 ,17 Quinolones have also been associated with an increased risk of S maltophilia.33 We cannot exclude that the increasing isolation of such pathogens may be caused by cross-infections among patients in CF centres or by contamination of aerosol devices.34 However, molecular studies to evaluate the possibility of cross infections among patients and microbiological surveillance of aerosol devices were not part of our study. The duration of the follow-up and the lack of internationally accepted definitions for the chronicity of such infections make clinical outcome evaluation difficult.
By delaying chronic P aeruginosa infection, early eradication treatment constitutes a positive result for patients. Currently, we lack direct evidence of the effect of eradication on patients' survival. According to recently published data, even mucoid P aeruginosa strains can be eradicated, but with a lower percentage of success compared with the treatment of non-mucoid phenotype strains.13 ,35
Further research is necessary to assess the effect of early antibiotic treatment on respiratory exacerbations and antibiotic use. Even though a gold standard has yet to be established, data from our study indicate that treatment efficacy does not seem to depend on the drugs used, or having previous eradication treatment, or the patients' stratification according to age and FEV1 values.
The extent to which treatment timelines can affect the microbiological outcome needs to be established.
Acknowledgments
We thank the following CF Centres Directors/Medical doctors for having made this study possible: R Gagliardini (Ancona); R Padoan (Brescia); L Ratclif (Cerignola); M Ambroni (Cesena); C Braggion (Firenze); L Minicucci (Genova); A Cosimi (Gualdo Tadino); A Negri, E. Micheletti (Livorno); F Forte (Matera); G Magazzù (Messina); C Colombo (Milano); F Pardo, M.Collura (Palermo); V Lucidi, E Fiscarelli (Roma - Ospedale Bambino Gesù). We give grateful thanks to Dr Sergio Zuffo and all the physiotherapists of the Cystic Fibrosis Centres who took part in the study.
References
Footnotes
↵* All members mentioned as Italian Group for P aeruginosa eradication in cystic fibrosis contributed to the interpretation of the data, commented extensively, revised the report critically, and approved the final version. GT had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Microbiological analyses were performed in their respective CF Centres by E Manso (Ancona), A D'Aprile (Cerignola), T Borio (Gualdo Tadino), S Campana, N Ravenni, D Dolce, P Cocchi, G Mergni (Firenze), L Cariani, G Defilippi (Milano), T Pensabene (Palermo), E Fiscarelli (Roma—Ospedale Bambino Gesù). L Cariani and G Defilippi performed molecular analyses on P aeruginosa strains.
Funding Italian Cystic Fibrosis Research Foundation (Grant FFC#17/2007) with the contribution of ‘Delegazione FFC di Vicenza’.
Competing interests None.
Patient consent Obtained.
Ethics approval Ethics Committee of Meyer Hospital (Florence, Italy).
Provenance and peer review Not commissioned; externally peer reviewed.
Members of Italian Group for P. aeruginosa eradication in cystic fibrosis Rolando Gagliardini, Esther Manso, Ospedali Riuniti di Ancona, Ancona, Italy; Rita Padoan, Elena Soncini, Clinica Pediatrica, Ospedale dei Bambini, AO Spedali Civili Brescia, Brescia, Italy; Angelica D’Aprile, Luigi Ratclif, Ospedale G Tatarella, Cerignola, Italy; Maura Ambroni, Divisione di Pediatria e Patologia Neonatale, Ospedale Bufalini, Cesena, Italy; Rosaria Casciaro, Laura Minicucci, Ospedale G Gaslini Divisione Pediatria I Genova, Italy; Tatiana Borio, Angelo Cosimi, Ospedale di Gubbio-Gualdo Tadino, Gualdo Tadino, Italy; Vanessa Boni, Gemma Braccini, Priscilla Cocchi, Daniela Dolce, Filippo Festini, Valeria Galici, Gianfranco Mergni, Novella Ravenni, Sergio Zuffo, Anna Meyer Children's University Hospital, Department of Sciences for Woman and Child's Health - University of Florence Florence, Italy; Amalia Negri, Divisione di Pediatria, Ospedale di Livorno, Livorno, Italy; Fabio Forte, Divisione di Pediatria e Neonatologia Dipartimento Donna, Maternità e Infanzia, Ospedale di Matera, Matera, Italy; Giuseppe Vieni, Clara Zinnarello, Ospedale “G Martino”, Messina, Italy; Laura Claut, Gloria Defilippi, Divisione Pediatria dell'Università degli Studi di Milano Fondazione IRCCS, Ca' Granda - Ospedale Maggiore Policlinico, Milano, Italy; Ersilia Fiscarelli, Ospedale Pediatrico Bambino Gesù, Roma, Italy; Mirella Collura, Tiziana Pensabene, Divisione Pediatria Ospedale dei Bambini "G. Di Cristina", Palermo, Italy.
Linked Articles
- Airwaves