Article Text

Abstract
Background: Several studies suggest that the periphery of the lung is the major site of inflammation in asthma. Fractional exhaled nitric oxide (Feno) and 8-isoprostane have been proposed as biomarkers of inflammation and oxidative stress. We therefore hypothesised that small airway dysfunction in asthma is of inflammatory origin that can be detected by molecular markers in exhaled air. To test this hypothesis, we examined the relationship of Feno and 8-isoprostane in exhaled air with small airways function as assessed by the single breath nitrogen test.
Methods: Sixteen patients (14 women) with mild atopic asthma (forced expiratory volume in 1 second >80% predicted) of mean (SD) age 23.0 (5.5) years participated in a cross sectional study. Feno was recorded by chemiluminescence and 8-isoprostane was measured by ELISA in concentrated exhaled breath condensate. The slope of phase III (δN2) and the closing volume (CV) were assessed from the single breath washout curve.
Results: The median Feno level was 30.4 ppb (range 10.1–82.8), the median 8-isoprostane concentration in exhaled breath condensate was 2.2 pg/ml (range 1.6–2.7), and the mean (SD) δN2 value was 1.1 (0.4)% N2/l. Feno was positively associated with δN2 (rs = 0.54, p = 0.032) while 8-isoprostane was inversely correlated with FEV1% predicted (rs = −0.58; p = 0.017) and CV as a percentage of vital capacity (rs = 0.58; p = 0.019).
Conclusions: Feno and 8-isoprostane in exhaled air are associated with small airways function in mild asthma. This suggests that these markers reflect small airway inflammation and favours a role for them as disease markers that is complementary to spirometry in the monitoring of patients with asthma.
- CV, closing volume
- EBC, exhaled breath condensate
- Feno, fractional exhaled nitric oxide
- FEV1, forced expiratory volume in 1 second
- FVC, forced vital capacity
- PC20MCh, provocative concentration of methacholine causing a 20% fall in FEV1
- nitric oxide
- oxidative stress
- exhaled markers
- 8-isoprostane
- asthma
Statistics from Altmetric.com
- CV, closing volume
- EBC, exhaled breath condensate
- Feno, fractional exhaled nitric oxide
- FEV1, forced expiratory volume in 1 second
- FVC, forced vital capacity
- PC20MCh, provocative concentration of methacholine causing a 20% fall in FEV1
Asthma is a chronic airway disease characterised by episodic symptoms of variable severity that are associated with functional alterations and pathological abnormalities such as airway inflammation and remodelling.1 Airway inflammation is present in all forms of asthma including mild and asymptomatic cases,2 and involves central as well as peripheral airways.3 In cases of fatal and non-fatal asthma the central as well as the distal airways exhibit profound pathology,4,5 infiltration with T lymphocytes and eosinophils being most prominent in the distal part of the respiratory tract.3 However, other authors have reported relatively large numbers of inflammatory cells or structural alterations in the proximal bronchi.6
It has recently been shown that molecular markers can be assessed in exhaled breath and that these may detect airway inflammation in asthma.7 Exhaled nitric oxide (NO) is currently the most widely used marker in exhaled breath. Indeed, fractional exhaled nitric oxide (Feno) levels are increased in asthma even in mild and asymptomatic conditions.7,8 Feno derives from endogenous NO production by NO synthases present in airway epithelium and inflammatory cells.9 Even though it is likely that Feno originates from the intrapulmonary airways in asthma,10 it is still unclear whether it mirrors small airways inflammation in this disease. Exhaled breath condensate (EBC) is another source of products of airway inflammation and oxidative stress,7 and it has been shown that exhaled 8-isoprostane, a marker of lipid peroxidation, is increased in asthmatic patients compared with controls.11 Again, it is unknown whether markers detected in the EBC arise from large or small airways.
The role of peripheral airway pathology in asthma is incompletely understood because of the sporadic availability of surgical lung tissue. Pathological changes in the small airways can be detected indirectly by physiological tests.12 Among these, the single breath nitrogen test can be used to evaluate the presence of uneven ventilation.13 In smokers the single breath nitrogen test has strongly been anchored to peripheral airways pathology, being more sensitive than any other physiological measurement in detecting early small airways pathology.14 In asthma In’t Veen et al15 recently showed that airway closure as measured by the single breath nitrogen test can discriminate between severe asthmatic patients with and without recurrent exacerbations, even when measured during clinically stable episodes. This is indicative of functional impairments in the periphery of the lung in asthma.
On this basis, we postulated that small airway dysfunction in asthma is of inflammatory origin that can be detected by molecular markers of inflammation in exhaled air. We addressed this hypothesis by examining the association of Feno and 8-isoprostane in EBC with functional impairment in the periphery of the lung as measured by the single breath nitrogen test in patients with asthma.
METHODS
Subjects
Twenty non-smoking or ex-smoking (<5 pack-years) atopic subjects with a doctor’s diagnosis of intermittent or mild persistent asthma were recruited. All patients reported one or more asthma symptom during the previous 12 months. The patients had a baseline forced expiratory volume in 1 second (FEV1) >80% of predicted and they all had bronchial hyperresponsiveness as shown by a provocative concentration of methacholine causing a 20% fall in FEV1 (PC20MCh) of <8 mg/ml.16 Their atopic status was determined by skin prick tests (Soluprick, ALK, Benelux). The patients were clinically stable for at least 1 month before the study and none had a history of a recent (⩽4 weeks) respiratory infection. The patients had not used inhaled or oral corticosteroids for at least 2 months before the study and 13 of them had used short acting β2 agonists on demand only.
We subsequently performed an additional control experiment in 15 healthy subjects to examine whether any of the observed associations between exhaled markers and small airways function were confined to asthma. All the control subjects were free from chronic respiratory symptoms, without current or previous diagnosis of asthma, and were lifelong non-smokers except for one ex-smoker who had smoked 2.5 pack-years.
The study was approved by the Leiden University Medical Center ethics committee and all patients gave their written informed consent.
Study design
The study was of a cross sectional design and was performed on 2 days. The first day was a screening day to check all inclusion and exclusion criteria. During the screening a clinical questionnaire, skin prick test, spirometric tests, and a methacholine challenge were performed in each patient. On the second day exhaled Feno measurements, a single breath nitrogen test, body box plethysmography, baseline spirometric tests, and collection of EBC were performed in this sequence.
Lung function
Spirometric testing was performed with a dry rolling seal spirometer (Morgan Spiroflow, Morgan, UK). Acceptability and reproducibility of FEV1 and forced vital capacity (FVC) were evaluated according to European Respiratory Society (ERS) guidelines.17 FEV1 was reported in litres, as percentage of predicted value (FEV1 % pred), and as percentage of FVC (FEV1/FVC%). Reference values were obtained from Quanjer et al.17 Total lung capacity (TLC), residual volume (RV), and functional residual capacity (FRC) were measured using a constant volume plethysmograph (Jaeger, Germany) by panting at 1 Hz, also according to ERS recommendations.17
Methacholine challenge was performed following standardised methodology16 using serial doubling concentrations of methacholine bromide (0.03–8 mg/ml, Janssen Pharmaceutica, Beerse, Belgium).
Small airways function
Small airways function was assessed by the single breath nitrogen test using a dry rolling seal spirometer (Morgan Spiroflow) filled with 100% oxygen and equipped with a nitrogen meter (Morgan) connected to the mouthpiece allowing continuous sampling, as described previously.13,15,18 During the test each patient performed a slow full inspiratory and expiratory vital capacity (VC) manoeuvre at a flow rate of 0.5 l/s. The constant flow was ensured by a mechanical flow regulator. The expiratory nitrogen concentration (%N2) was plotted against lung volume (between TLC and RV) producing the expiratory nitrogen washout curve.13,18 The slope of the nitrogen alveolar plateau (δN2, phase III) was calculated by drawing the best fit line through phase III of the expiratory volume-concentration curve,13 and was expressed as %N2/l. One expert operator (PJS), who was unaware of the patients’ characteristics, manually drew all lines. This procedure has been validated in our laboratory, showing good within and between observer reproducibility in the slope of phase III (intraclass correlation coefficient, Ri = 0.94 and 0.99, respectively) and in closing volume (Ri = 0.93 and 0.94). The first departure from this straight line was considered as indicative of airway closure, allowing the calculation of closing volume (CV, phase IV) and closing capacity (CC = RV+CV).15,18 The measurements were only accepted if the VC during the single breath nitrogen test was within a 10% range of VC measured by spirometric testing. CV and CC were expressed as the ratio of VC (CV/VC) and TLC (CC/TLC), respectively.
Exhaled NO
Exhaled NO (Feno) levels were determined as previously described,19 following guidelines for the online single breath method20,21 and using a chemiluminescence online analyser (Sievers NOA 270B, Sievers, Boulder, Colorado, USA). During the measurement the subjects inspired “NO-free” air (<2 ppb). The subjects were asked to perform a slow vital capacity manoeuvre with a constant expiratory flow rate of 100 ml/s19 using online visual monitoring. Measurements were discarded if the expiratory flow varied by more than 10% from target flow. An expiratory resistance of 5 cm H2O was applied in order to prevent nasal NO contamination. Expired NO was sampled continuously from the centre of the flow with a sample flow of 440 ml/min. The expiratory flow was measured by a pneumotachograph (Lilly principle, Erich Jaeger GmbH, Würzburg, Germany). Exhaled NO concentrations were determined at a 10 second plateau and expressed as parts per billion. Three successive manoeuvres were recorded for each subject at 1 minute intervals and the mean value of the three tests was used for statistical analysis.
EBC collection and analysis
EBC was collected (EcoScreen, Jaeger, Germany) while the patient was breathing room air through a mouthpiece connected to a two way non-rebreathing valve and to a saliva trap. Each patient was asked to breath at a normal frequency and tidal volume for 15 minutes wearing a nose clip. This allowed about 2 ml of condensate to be collected from the patient.
The collected fluid was immediately subdivided into 600 μl aliquots in Eppendorf tubes which were instantaneously cooled with ice cold 2-methylbutane and then directly transferred to −80°C pending analysis.
Pilot experiments performed in our laboratory and studies from other institutes22 have shown very low 8-isoprostane concentrations in EBC samples (close to the detection limit) from subjects similar to those participating in the present study. 8-isoprostane in EBC was therefore concentrated using an affinity sorbent (8-isoprostane affinity sorbent, Cayman Chemical, Ann Arbor, MI, USA). Briefly, 500 μl EBC was incubated with 100 μl sorbent for 60 minutes at room temperature. After centrifugation and washing of the sorbent, bound 8-isoprostane was eluted from the sorbent using 95% ethanol. The eluate was lyophilised by vacuum centrifugation and re-suspended in 165 μl of enzyme linked immunosorbent assay (ELISA) buffer (8-isoprostane EIA kit, Cayman Chemical) to obtain a threefold concentrated solution. The concentration of 8-isoprostane was assessed by ELISA (Cayman Chemical; lower limit of detection 5 pg/ml) and used to calculate the concentration in the original sample before the concentration procedure. All samples were analysed in duplicate and the mean intra-assay coefficient of variation was 7.7% (range 1.0–18.9%). In addition, separate spiking experiments were performed by adding 50 μl 8-isoprostane (500 pg/ml; standard from 8-isoprostane EIA kit) to 450 μl thawed EBC collected from volunteer subjects. These experiments showed good recovery of added 8-isoprostane when the non-concentrated procedure was used (recovery >90%), whereas recovery was low when using the affinity sorbent (about 60%). Interestingly, recovery in the affinity sorbent procedure was near 100% using phosphate buffered saline instead of EBC, suggesting that some components of EBC interfere with binding of 8-isoprostane to the affinity sorbent.
The mean intra-assay coefficient of variation for the subsequent control experiments in healthy subjects was 5.2% (range 0.7–10.3%). In 10 subjects from this control group we assessed the recovery of 8-isoprostane in EBC and observed a mean recovery of 88% (range 57–115%). Because this study was performed separately from the original study in asthmatics, we have not analysed the absolute values of 8-isoprostane between both groups.
Statistical analyses
Data are presented as mean (SD) or median (range) depending on whether they were normally distributed. The relationships between variables are expressed as Spearman rank correlation coefficient (rs); differences at p values of <0.05 were considered to be statistically significant.
RESULTS
Sixteen patients of mean (SD) age 23.0 (5.5) years (male/female ratio 2/14) completed the study. From the initial 20 subjects, one dropped out because of an asthma exacerbation on the test day, one was excluded due to the use of nasal steroids 5 days before the test, and another two subjects were excluded because their VC measured during the single breath nitrogen test differed by more than 10% from the VC measured by baseline spirometry.
The characteristics of the patients who completed the study are shown in table 1. Mean (SD) FEV1 was 97.3 (12.6)% and PC20MCh ranged between 0.05 and 4.18 mg/ml (geometric mean 0.45 mg/ml), which is indicative of mild to severe airway hyperresponsiveness. In accordance with this, Feno levels were high with a median of 30.4 ppb (range 10.1–82.8), whereas the single breath nitrogen test showed mean (SD) δN2 values of 1.1 (0.4)% N2/l and a mean (SD) CV/VC value of 8.6 (5.7)%. As described earlier, 8-isoprostane measurements were obtained from EBC samples that were concentrated threefold; after correction for this, the median 8-isoprostane value was 2.2 pg/ml (range 1.6–2.7).
Characteristics of study subjects
Interestingly, Feno levels were positively correlated with δN2 values (rs = 0.54, p = 0.032; fig 1A), whereas there was no significant correlation between Feno and baseline FEV1% pred (fig 1B), PC20MCh, CV/VC, or CC/TLC (lowest p value = 0.16).

(A) Correlation between exhaled nitric oxide (Feno) concentration in ppb and uneven ventilation (δN2 (%N2/l)). (B) Correlation between exhaled nitric oxide (Feno) concentration in ppb and FEV1 (% of predicted value).
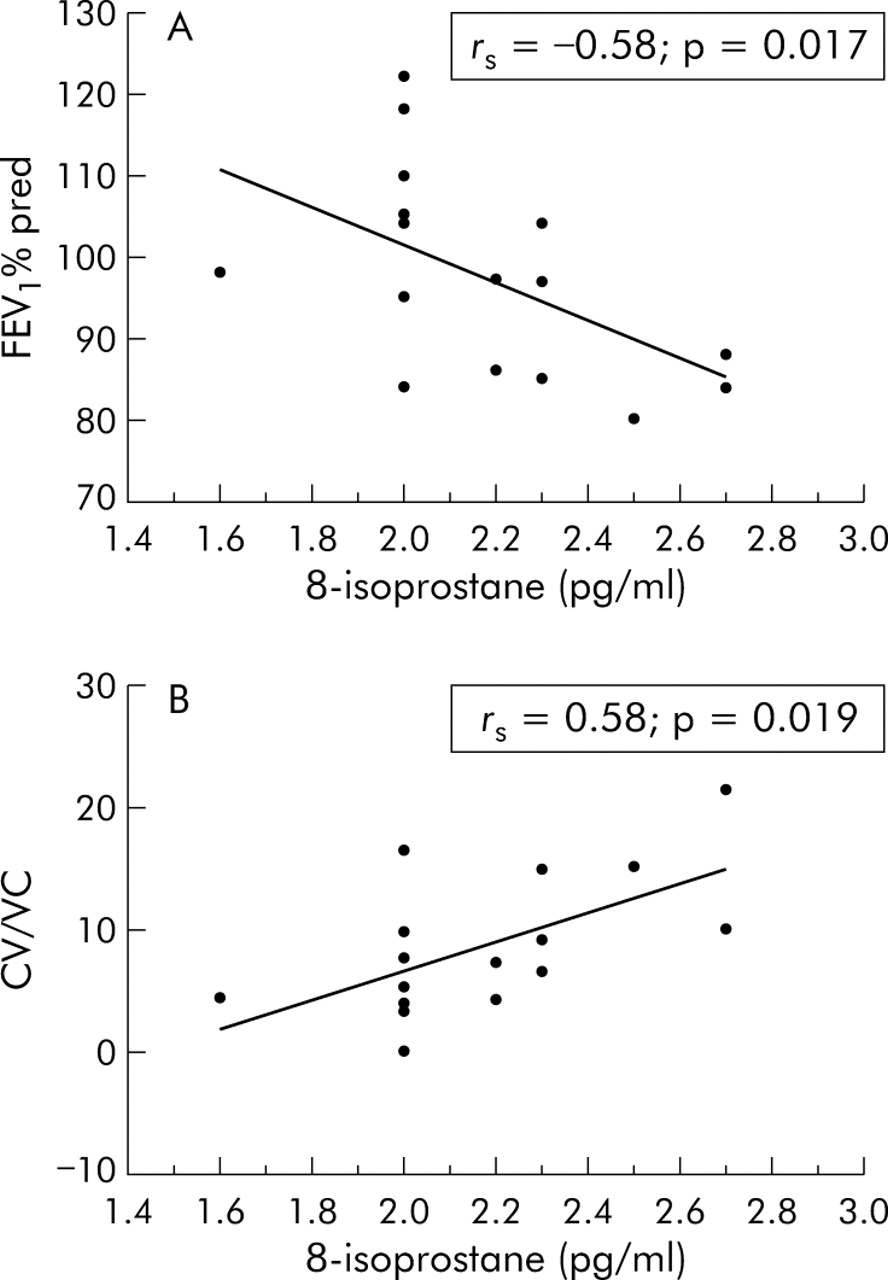
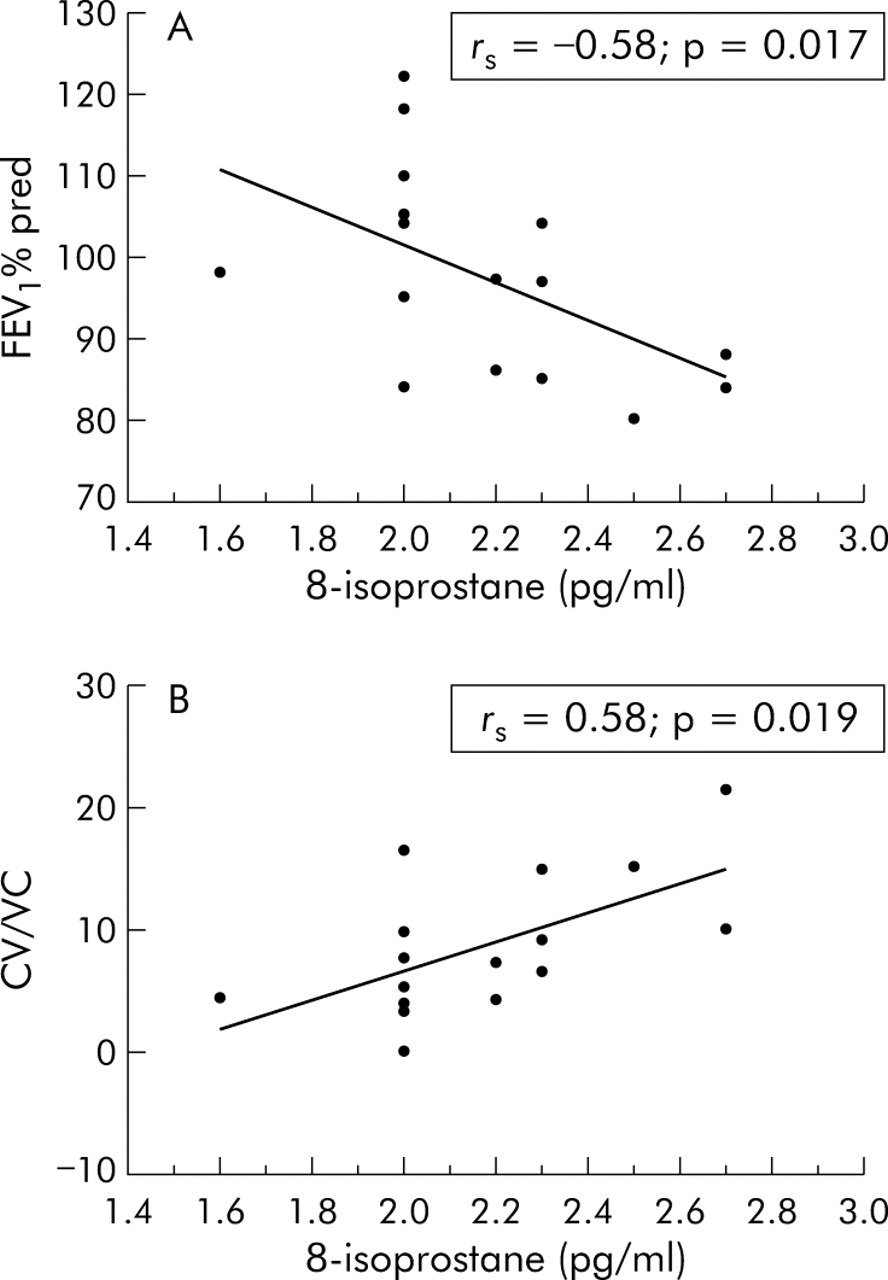
The concentration of 8-isoprostane in EBC was inversely correlated with FEV1 % pred (rs = −0.58, p = 0.017; fig 2A) and positively correlated with CV/VC (rs = 0.58, p = 0.019; fig 2B). There were no correlations between 8-isoprostane and Feno, δN2, CC/TLC, or PC20MCh (lowest p value = 0.051).
{kind=link}
{kind=link}
(A) Correlation between 8-isoprostane in exhaled breath condensate (pg/ml) and FEV1 (% of predicted value). (B) Correlation between 8-isoprostane in exhaled breath condensate (pg/ml) and closing volume as percentage of vital capacity (CV/VC).
In the control group mean (SD) FEV1 % pred was 105.1 (10.7)%, Feno levels ranged from 0.6 to 17.0 ppb (median 8.6 ppb), the single breath nitrogen test showed a mean δN2 value of 1.2 (0.4)% N2/l and a CV/VC of 9.3 (5.2)%. The median 8-isoprostane value was 3.6 pg/ml (range 2.9–7.6) after correction for the threefold concentration used in the sample preparation. There were no significant correlations between the exhaled markers and lung function measures in the healthy subjects (lowest p value = 0.54).
DISCUSSION
Our results indicate that exhaled molecular markers of inflammation and oxidative stress are associated with functional evidence of small airway involvement in intermittent/mild persistent asthma. Exhaled NO levels are positively correlated with non-homogeneous emptying of lung units, as reflected by a steeper slope of phase III, but are not correlated with spirometric measurements. Furthermore, 8-isoprostane levels in EBC are increased in patients with more prominent airway closure, as shown by a positive correlation with CV/VC. This suggests that Feno and 8-isoprostane may originate in part from small airways, thereby potentially providing complementary information to spirometry in the management of intermittent/mild persistent asthma.
The novel finding of this study is the association of exhaled markers of inflammation and oxidative stress (Feno and 8-isoprostane) with indices of small airways function (δN2 and CV/VC, respectively). Interestingly, we observed an inverse correlation between 8-isoprostane in EBC and FEV1, whereas Feno levels did not correlate with 8-isoprostane. The latter result differs from previous studies on EBC in adult asthmatics,11 and is presumably due to differences in clinical characteristics, age, or EBC analysis. Moreover, we have shown that the association of markers in exhaled air (Feno and 8-isoprostane) with lung function was only observed in asthmatic subjects and not in healthy controls.
In this study particular attention was paid to methodological aspects such as patient selection. None of the patients used steroids and all had well documented disease by previous doctor’s diagnosis, presence of symptoms during the last 12 months, and hyperresponsiveness to methacholine. The patients had intermittent/mild persistent asthma which is compatible with the Feno levels being higher than 10 ppb (that is, above the range for normal subjects).21 Although it may be argued that δN2 values overlapped the normal range as reported from general population subjects,13,18 it should be considered that these values ranged 3.6-fold from 0.5% to 1.8% N2/l (table 1), which can be considered sufficient to reveal mild uneven ventilation in patients with mild asthma.
Levels of 8-isoprostane in EBC in asthmatics ranged from 1.6 to 2.7 pg/ml. These levels are lower than those previously reported by Montuschi et al11 for EBC (mean 33.7 pg/ml in mild asthma). However, in a more recent study the latter investigators also found lower 8-isoprostane concentrations in mild asthmatics (mean values 10.4–12.8 pg/ml at baseline).23 Moreover, 8-isoprostane (or 8-epi-PGF2α) is one of the F2-isoprostanes, which have a mean (SE) basal concentration of 0.9 (0.2) pg/ml in bronchoalveolar lavage fluid.24 Furthermore, in some previous studies the values of non-concentrated samples in which no 8-isoprostane was detected were arbitrarily set at the lower limit of detection of the assay. We cannot exclude the possibility that this may have led to an overestimation of mean values, so the EBC levels of 8-isoprostane seen in this study seem to be consistent with the literature.
In our study particular attention was paid to laboratory methods using internal standard operating procedures specifically designed for EBC collection and storage as well as for 8-isoprostane measurements. The study was preceded by repeated pilot experiments which showed that it was essential to include a concentration step (threefold) in the procedure to analyse 8-isoprostane in EBC; the 8-isoprostane values reported in this study were therefore obtained after correcting for the concentration factor. Using non-concentrated samples we obtained very low values that were just above or around the detection limit of the assay, yielding inconsistent data as also observed by others.22 With regard to the recovery of added 8-isoprostane in spiking experiments, we observed a recovery of about 60% in subjects with asthma and 88% in healthy controls. This indicates that recovery in EBC from healthy subjects is higher than in asthmatics, with a large inter-subject variability. This may suggest that 8-isoprostane levels are underestimated in asthmatics. Future studies need to include assessment of recovery of 8-isoprostane levels in each individual EBC, which should be used for correction of the measured values. Finally, given the fact that the recruitment and all measurements of the control group were done on a separate and subsequent occasion, we did not analyse the differences between asthmatics and controls.
Our findings support previous observations on changes in peripheral lung function in asthma as assessed by multiple breath nitrogen washout, which is a test specifically designed to quantify impaired acinar ventilation distribution.25 Validation of the single breath nitrogen test in relation to histological features of small airways inflammation is lacking in asthma because of the limited availability of peripheral lung tissue in this disease. However, this has been studied in detail in smokers14 in whom non-homogeneous ventilation was observed, not only in the presence of emphysema and/or severe small airways disease, but also in patients with mild small airways disease.14 Even if non-homogeneous ventilation in the central airways might have influenced our results, the data in smokers indicate that δN2 is the physiological marker that is most strongly associated with small airways disease.14
How should we interpret the association between small airways function and Feno/8-isoprostane levels in exhaled breath? Exhaled NO reflects endogenous production of NO by NO synthases, which are present in the (large) airways of patients with asthma.26 The main site of inducible (type II) NO synthase expression is the airway epithelium, and it is also observed in several inflammatory cells.27 It is therefore conceivable that epithelial cells of small airways and inflammatory cells infiltrating peripheral airways wall contribute to the levels of NO measured in expired air. Chronic inflammation can be associated with modified structure of the small airway walls, which contributes to the non-homogeneous obstruction of small airways.4 This condition is likely to induce non-homogeneous emptying of peripheral lung units28 which can be measured as a steeper phase III (δN2).29 Although a significant statistical correlation does not directly indicate that Feno and 8-isoprostane originate from the small airways, we believe that our findings may provide indirect support for the hypothesis that this is the site of origin of these markers. However, we cannot exclude alternative hypotheses. Firstly, Feno and δN2 might reflect abnormalities of distinct areas in the lung while both being driven by shared but widespread inflammatory mechanisms. Secondly, it is possible that uneven ventilation by itself affects Feno in asthma. This could be addressed by including uneven ventilation in validated mathematical models.30 Thirdly, even the correlations between 8-isoprostane and lung function tests could have occurred by chance. However, we believe that the biological plausibility of the observed inverse correlation between 8-isoprostane levels and FEV1 % pred and its positive correlation with CV/VC indirectly support the accuracy of our measurements. Taken together, our data support the need to compare directly Feno and 8-isoprostane levels with small airways disease, even in the very limited resection material available from young patients with mild asthma.
The role of peripheral airways disease in asthma is largely unknown, partly because of the relative sporadic availability of peripheral lung tissue. Several authors have therefore proposed alternative methods for studying small airways in asthma, such as bronchoalveolar lavage, transbronchial biopsy, ultrathin bronchoscopy, induced sputum, high resolution computed tomography, or magnetic resonance imaging with hyperpolarised 3He gas.12 Some of these methods are invasive and are therefore potentially more hazardous to patients than simple physiological measurements. However, these methods may explore different aspects of small airways physiology, biology and pathology and therefore may be considered as complementary techniques in assessing peripheral airways.
What are the clinical implications of our study? Firstly, our findings underline the relevance of assessing small airways function even in patients with mild degrees of asthma. Secondly, our results favour a role for exhaled markers (Feno and 8-isoprostane) as indices of the functional status of small airways that appears to be complementary to spirometry in monitoring patients with asthma. It needs to be emphasised that our study was performed in patients with atopic intermittent/mild persistent asthma; caution should be taken in extrapolating the present observations to non-atopic patients or to those with different degrees of disease severity.
In conclusion, in patients with mild atopic asthma not using inhaled steroids we have shown that exhaled NO levels increase with increasing unevenness of ventilation and 8-isoprostane levels in EBC are higher in patients with more prominent airway closure. These data suggest that exhaled molecular markers of inflammation and oxidative stress reflect small airways function in asthma. Further investigations are needed to assess a direct link between Feno and 8-isoprostane and the morphology and inflammatory activity in the small airways.
Acknowledgments
The authors thank A C van der Linden for expert technical assistance.
REFERENCES
Footnotes
-
† Deceased December 2004.
-
This study was funded by Università di Palermo and Leiden University Medical Centre (LUMC), Valeas Italy and Italian Nitric Oxide Club (INOC).
-
Competing interests: SB has received unrestricted educational grants from Valeas Italy, GlaxoSmithKline and AstraZeneca. HdH, MCT, SPGL have no competing interests. AMV has been a consultant, participated in advisory board meetings and received lecture fees from GlaxoSmithKline and AstraZeneca. KFR has been a consultant, participated in advisory board meetings and received lecture fees from AstraZeneca, Boehringer, Pfizer, Novartis, AltanaPharma, MSD, and GlaxoSmithKline. VB has participated in advisory board meetings and received lecture fees from GlaxoSmithKline. The Department of Pulmonology (and thereby KFR, PSH and PJS as staff members) have received grants from AltanaPharma, Novartis, Bayer, AstraZeneca, Pfizer, MSD, Exhale Therapeutics and GSK in the years 2001–2004. The Istituto di Medicina Generale e Pneumologia (and thereby AMV and VB as staff members) have received grants from Bayer, Rhone Poulenc, AstraZeneca, MSD, and Aventis Pharma in the years 2001–2004.