Article Text

Abstract
The authors report a novel case of exercise-induced haemoptysis with an unexpected underlying pathology. The report discusses the case and provides a pragmatic overview of the diagnosis and management of the pulmonary vein stenosis.
- Exercise
- Histology/Cytology
- Imaging/CT MRI etc
- Interstitial Fibrosis
Statistics from Altmetric.com
Case discussion
Dr J H Hull (JHH): A 43-year-old immunocompetent man has been referred with a 1-year history of intermittent left-sided pleuritic chest pain and exercise-associated haemoptysis. There is no history of systemic symptoms, and he is clinically well between episodes. The only medical history of note is of atrial fibrillation, treated successfully 18 months earlier with ablation therapy. There is no history of infection, pneumotoxic exposures or symptoms suggestive of an autoimmune disease or systemic vasculitis. He is taking no regular medication.
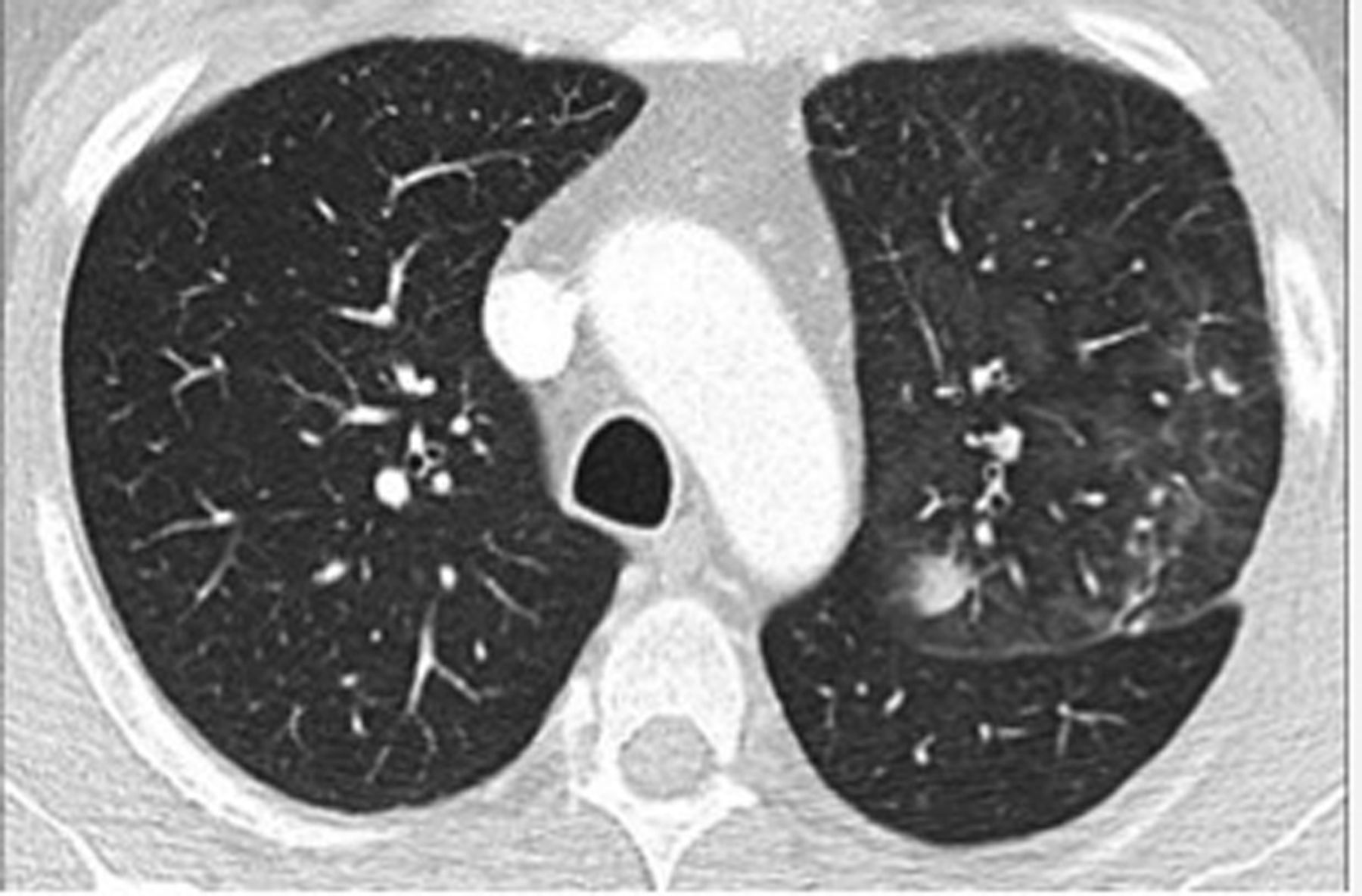
There is no laboratory evidence of coagulopathy or blood dyscrasia. Chest radiograph was normal; however, high-resolution CT images of the thorax, performed following an acute episode of the haemoptysis, demonstrated multifocal ground-glass opacities confined to the left upper lobe (figure 1). Mediastinal structures were normal, and there was no lymphadenopathy.

High-resolution CT images of the thorax demonstrating multifocal ground-glass opacities confined to the left upper lobe.
T M Maher (TMM): The imaging is striking for the localised nature of the parenchymal changes. What other investigations have been performed?
JHH: Following a non-diagnostic transbronchial biopsy, a surgical lung biopsy was performed at the referring unit.
Professor A G Nicholson (AGN): This demonstrated focally fibrinous organising pneumonia (OP) and moderate haemosiderosis (figure 2).
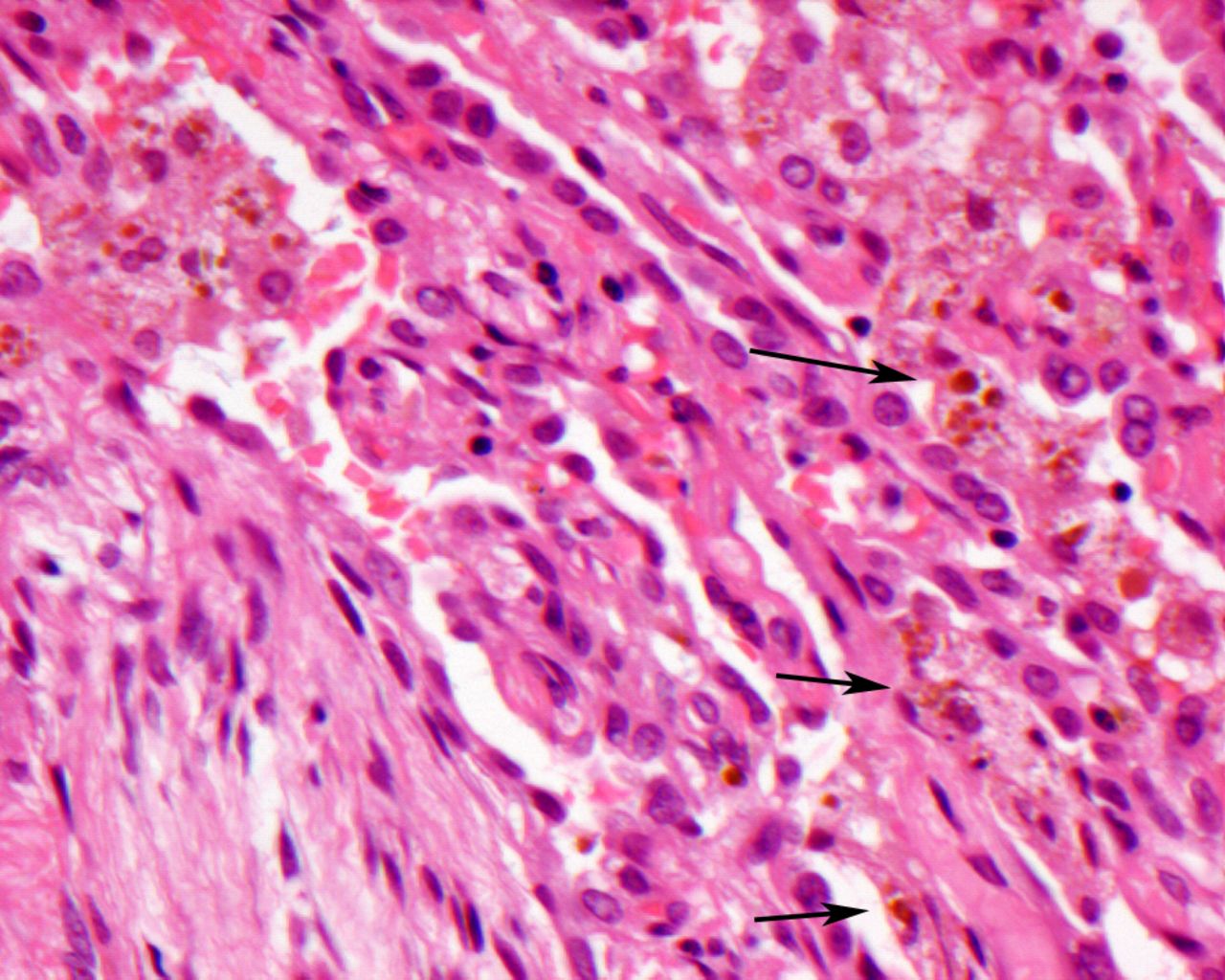
The lung shows focally fibrinous organising pneumonia (lower left) and moderate haemosiderosis (arrows). H&E stain, ×200.
JHH: Treatment with oral corticosteroid and antibiotics was administered following biopsy and symptoms improved initially. However, when these recurred, the patient was referred for further investigation.
TMM: The differential diagnosis for paroxysmal haemoptysis is broad; however, in this case, the focal nature of the CT changes and medical history make one particular diagnosis stand out. I would proceed to arrange magnetic resonance angiography (MRA) of the pulmonary vasculature.
Dr R H Mohiaddin (RHM): MRA scan demonstrated significant focal stenosis of the left common pulmonary vein (figure 3).

{kind=link}
{kind=link}
{kind=link}
Surface-rendered image reconstructed in the right anterior oblique view from contrast-enhanced magnetic resonance angiography acquisition showing significant focal stenosis of the left common pulmonary vein (arrow). L, left atrium.
TMM: Pulmonary vein stenosis (PVS) is a recognised complication of pulmonary venous ablation therapy for atrial fibrillation.1 The endoluminal generation of lesions encircling the pulmonary veins, undertaken through application of a radiofrequency signal to the pulmonary vein ostia, represents a modification of the maze procedure and has a 70% efficacy in curing atrial fibrillation.2 However, PVS arising from focal necrosis at the site of ablation is a recognised complication between 0.4%3 and 5%4 of the cases. The risk of the PVS appears dependent upon the technique employed and is less common with current approaches. This likely relates to the development of more advanced pulmonary vein mapping procedures and improved targeting of the anatomical segments.5
The clinical presentation of postablation PVS is varied, and many patients remain asymptomatic despite the development of significant stenosis.6 In other cases, the presentation may coincide with cessation of anticoagulation therapy, resulting in local thrombosis.5 Accordingly, some centres5 advocate screening for PVS at 3 months following the index treatment. This is on the basis that early intervention may obviate occlusion and maximise an opportunity to restore functional pulmonary flow; it has been argued that delayed intervention, even with a good restoration of pulmonary flow, may not lead to significant improvements in perfusion of an affected segment.5
It is noteworthy, however, that PVS may develop and progress over several months following ablation, thus giving rise to a lag between the time of procedure and the onset of symptoms. This temporal dissociation often makes diagnosis challenging and thus a high diagnostic index of the suspicion is required when new cardiorespiratory symptoms develop weeks to months after an ablation procedure. This time lag may also, in at least part, explain why diagnosis is often delayed and PVS has been misdiagnosed as pulmonary embolus, atypical pneumonia, lung malignancy or, as in this case prior to referral to our unit, cryptogenic organising pneumonia.1 ,5 It is a novel presentation in that his symptoms were principally confined to exercise.
JHH: It is possible that the increased cardiac output and locally altered pulmonary vascular resistance during exercise resulted in capillary extravasation. This could be considered akin to the proposed pathophysiology of the exercise-induced pulmonary haemorrhage in equine thoroughbreds; during exercise, venous occlusion increases regional pulmonary capillary pressure, likely causing capillary rupture and haemoptysis.7 This is manifested as haemosiderosis with coexistent OP on biopsy, but no evidence of capillaritis or distal venous pathology on biopsy. A similar phenomenon has been reported to occur in individuals with severe mitral valve stenosis and undoubtedly reflects similar pathomechanisms, albeit affecting the whole of the pulmonary vasculature.7
RHM: A number of imaging modalities have been used to successfully detect and characterise PVS, including contrast CT, transoesophageal echocardiography and MRA. The latter is attractive in that it allows high-quality and detailed three-dimensional anatomical characterisation non-invasively and without x-ray radiation.8
TMM: There is a lack of consensus on therapeutic strategies for postablation PVS. There is general agreement that patients with symptomatic severe PVS should be treated with pulmonary vein angioplasty with or without stenting.5 In this case, following diagnosis, the patient underwent balloon dilatation of the left common pulmonary vein (see ref. 9 for description of the procedure). It is recognised that the pulmonary veins are susceptible to in-segment restenosis;5 ,9 however, patients often remain asymptomatic if this occurs. A year on from balloon dilatation, our patient remains well, without further exercise-induced haemoptysis and with resolution of the previously noted radiographic changes on chest x-ray.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online video
Footnotes
-
Contributors All authors contributed to the conception, design, analysis and interpretation of data.
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; internally peer reviewed.