Article Text

Abstract
Background Excess visceral adiposity and sleep apnoea are two conditions independently associated with cardiovascular diseases. The two conditions are often combined and are believed to interact in a vicious circle.
Objectives To compare the response of men with visceral obesity with or without sleep apnoea syndrome to a 1-year healthy eating, physical activity/exercise intervention programme.
Methods 77 men, selected on the basis of increased waist circumference (≥90 cm) and dyslipidaemia (triglycerides ≥1.69 and/or high-density lipoprotein (HDL) cholesterol <1.03 mmol/litre), participated in this study. Body composition and fat distribution were assessed by dual-emission X-ray absorptiometry or CT and sleep breathing disorders by home-based polygraphic recording. Cardiorespiratory fitness, plasma adipokines, plasma inflammatory markers, fasting lipoprotein–lipid profile and oral glucose tolerance test were assessed.
Results After the 1-year lifestyle intervention, the mean oxygen desaturation index (ODI) of the whole sample decreased (−3±13 events/h, p<0.05). Men with sleep apnoea syndrome at baseline (ODI ≥10 events/h, n=28) showed smaller reductions in body mass index, waist circumference, triglycerides and smaller increases in HDL cholesterol and adiponectin than men without sleep apnoea (ODI <10 events/h, n=49), despite similar compliance to the programme. The higher the baseline ODI and the time spent under 90% saturation, the lower the reductions in fat mass and visceral adiposity, and the smaller the improvement in glucose/insulin homeostasis indices after 1 year.
Conclusions Men with sleep apnoea syndrome at baseline had smaller reduction in body weight and less metabolic improvements associated with the lifestyle intervention programme than men without sleep apnoea syndrome.
- Intra-abdominal fat
- sleep apnoea syndrome
- diet
- exercise
- cardiometabolic risk
- clinical epidemiology
- sleep apnoea
- respiratory measurement
- respiratory muscles
Statistics from Altmetric.com
- Intra-abdominal fat
- sleep apnoea syndrome
- diet
- exercise
- cardiometabolic risk
- clinical epidemiology
- sleep apnoea
- respiratory measurement
- respiratory muscles
Key messages
What is the key question?
Is the response similar between men with visceral obesity with or without sleep apnoea syndrome to a 1-year healthy eating, physical activity/exercise intervention programme?
What is the bottom line?
Excess visceral adiposity and sleep apnoea are two conditions independently associated with an increased risk of cardiovascular diseases. The two conditions are often combined and are believed to favour a reciprocal worsening.
Why read on?
Sleep-induced disordered breathing of men with visceral obesity was improved after a 1-year healthy eating, physical activity/exercise programme. The presence of sleep-disordered breathing at baseline attenuated the reduction of body weight and the improvement of the cardiometabolic risk profile in response to the 1-year lifestyle intervention.
Introduction
Excess visceral adipose tissue (VAT) and obstructive sleep apnoea syndrome (OSAS) are two conditions independently associated with an increased risk of cardiovascular diseases and mortality.1 ,2 Both conditions are linked with increased insulin resistance, inflammatory cytokines and blood pressure levels.3–6 Moreover, excess VAT and OSAS are often associated conditions which are believed to interact with each other in a vicious circle.6 ,7 For instance, Peppard et al8 demonstrated that 10% weight gain or weight loss were respectively associated with a 32% increase and a 26% decrease in the apnoea + hypopnoea index (AHI), whereas the level of physical activity was inversely associated with the level of AHI.9 Of importance, the treatment of OSAS by continuous positive airway pressure (CPAP) has been associated with a VAT loss, independent of the change in body weight.10
Three recent studies have tested the efficacy of lifestyle intervention programmes to reduce AHI in patients with OSAS.11–13 All these studies found that the body weight loss related to lifestyle interventions was associated with a decrease in AHI. These results were sustained after 1 year of follow-up.14 ,15 However, whether the benefit of such lifestyle intervention programmes to improve the cardiometabolic risk profile could be affected by the presence and severity of sleep-disordered breathing has not been addressed.
We recently investigated a group of men with visceral obesity, defined as abdominal obesity and the dyslipidaemia of insulin resistance,13 that is, high triglyceride and/or low high-density lipoprotein (HDL) cholesterol levels, who were involved in a healthy eating, physical activity/exercise lifestyle modification programme. In this study, we addressed the presence and severity of sleep breathing disorders in an ancillary study conducted to compare the response of men with visceral obesity with or without OSAS to a 1-year lifestyle intervention; that is, to test whether having sleep-disordered breathing could impede the improvement of the cardiometabolic risk profile in response to a 1-year healthy eating, physical activity/exercise lifestyle modification programme.
Methods
Further information on the methods is presented in an online supplementary file.
Study design
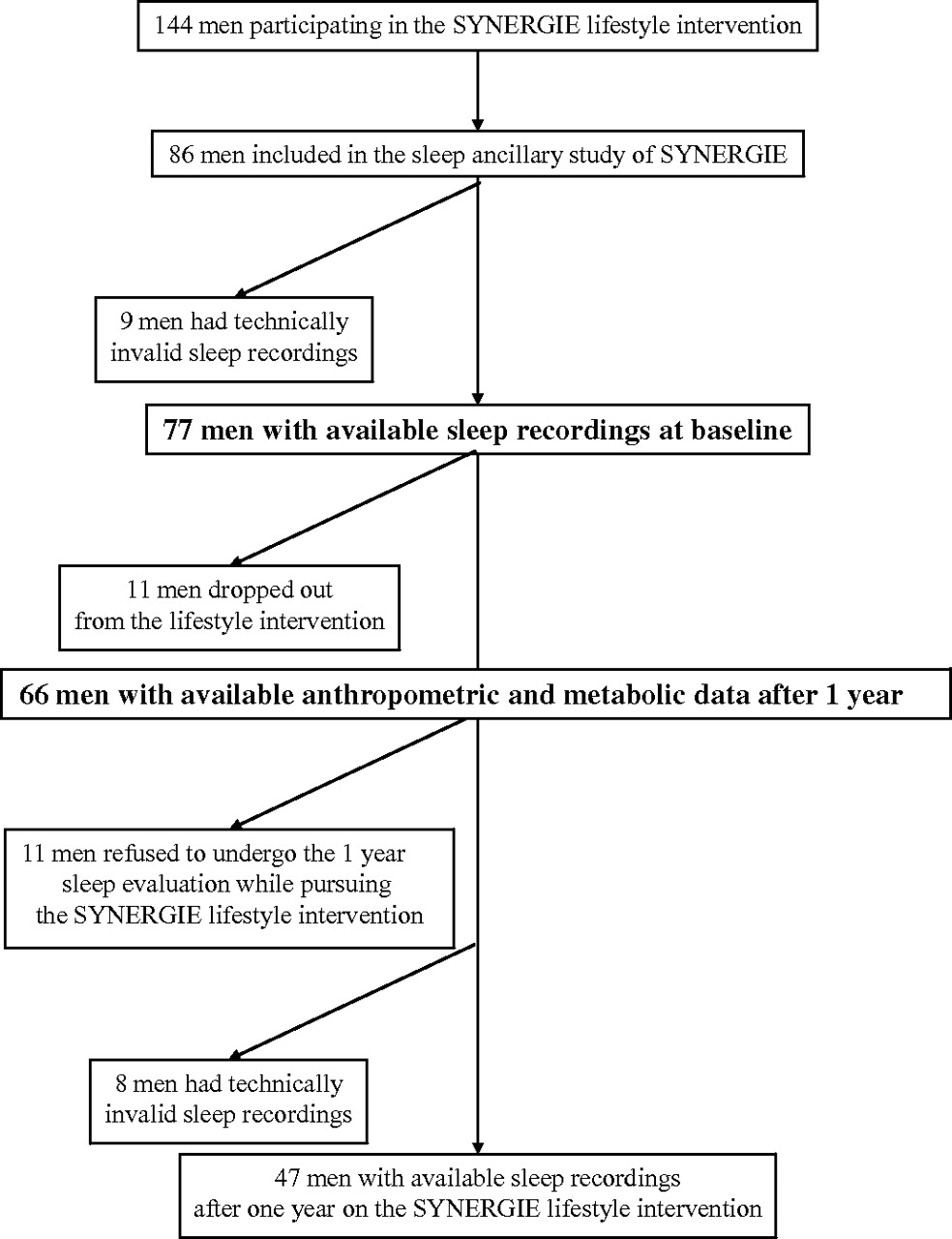
Men (n=144) between 30 and 65 years old, presenting with a waist circumference ≥90 cm, triglyceride levels ≥1.69 mmol/litre and/or HDL cholesterol <1.03 mmol/litre were recruited in the general community to take part in a 3-year lifestyle modification programme (the ‘SYNERGIE’ study, to emphasise the synergism between healthy eating and increased physical activity/exercise). From these 144 men, 86 volunteered to participate in an ancillary study addressing nocturnal respiratory disturbances at baseline and after 1 year. From these 86 men, 77 had a technically acceptable sleep home-recording, and were kept for baseline analyses, whereas data on 66 men were available for the 1-year analyses (figure 1). Written consent was obtained for every study participant which was approved by the Medical Ethics Committees of Université Laval and of the Institut universitaire de cardiologie et de pneumologie de Québec.

Flow chart.
Subjects were individually counselled once every 2 weeks during the first 4 months of management with subsequent monthly visits to improve their nutritional and physical activity/exercise habits. Each visit included an interactive session with a registered nutritionist followed by a meeting with a kinesiologist. The nutritional counselling was adapted to elicit a 500 kcal daily energy deficit during the first year, which was the ‘moderate weight loss’ phase of SYNERGIE. The daily caloric intake was estimated at baseline and at 1 year by a 3-day dietary record including a non-working day. The physical activity programme aimed to reach 160 min/week of moderate intensity endurance exercise. Men received a personalised training programme elaborated according to subjects' history and preferences and based on results to a maximal treadmill test and on the rating of self-perceived exhaustion (modified Borg scale16). Men had free access to an on-site fitness centre and were allowed to perform exercise on site or outside at their convenience. To help participants to be more active and to monitor themselves between exercise sessions, they were asked to wear a pedometer and to reach a target of 10 000 daily steps.
CT scan
Partial volumes of VAT and subcutaneous abdominal adipose tissue were calculated17 from cross-sectional areas assessed at L2–L3 and L4–L5 by CT.18 ,19
Cardiorespiratory fitness
A submaximal treadmill standardised exercise test evaluated cardiorespiratory fitness using two indices: the subject's heart rate (mean of the last 3 min) at a submaximal treadmill workload (3.5 mph, 2% slope); and the estimated16 metabolic equivalent of task reached by the subject at a heart rate of 150 beats/min.
Oral glucose tolerance test
Participants were subjected to a standard, 3 h, 75 g oral glucose tolerance test (OGTT).
Nocturnal respiratory recording
Daytime sleepiness was evaluated with the Epworth Sleepiness Scale.20 Presence of nocturnal respiratory disturbances was assessed at home (Remmers Sleep Recorder Model 4.2; Saga Tech Electronic, Calgary, Alberta, Canada). The oxygen desaturation index (ODI) (number of oxygen saturation (SpO2) decreases ≥4%/recording time), mean SpO2, minimal SpO2, time spent under 90% of SpO2 and total monitoring time were automatically determined.21 Apnoea and hypopnea lasting ≥10 s were scored to determine the respiratory disturbance index (RDI). ODI was used to establish sleep apnoea phenotype using the 10/h ODI cut-off to separate participants with or without moderate to severe OSAS, as previously described.21 ,22
Statistical analysis
The primary outcome of the SYNERGIE study was the VAT volume change after the intervention. In the present ancillary study, the primary outcome was the change in ODI after the 1-year lifestyle intervention. Baseline and 1-year results were expressed as mean (SD) for normally distributed variables and as median (IQR) for non-normally distributed variables. One year changes are expressed as mean (95% CI).
Statistical significance of changes after 1 year was evaluated using mixed linear models with the time of measurement (baseline and 1 year) as a repeated measure on the 77 patients who completed the sleep recording at baseline (table 1).
Characteristics of men with visceral obesity at baseline and after 1 year on the lifestyle intervention programme
Men were then classified according to baseline ODI value, below or above 10 events/h. Comparisons between the two groups at baseline were made by mixed linear model. The two groups were also compared for the 1-year changes with the same mixed linear model. One-year changes were then adjusted for baseline VAT volume and baseline daily step count and compared with analysis of covariance models (table 2).
Response to the 1-year healthy eating, physical activity/exercise lifestyle modification programme according to oxygen desaturation index level at baseline
Linear regressions were quantified between baseline ODI (log transformed) with 1-year changes of cardiometabolic risk markers. Spearman rank correlations were computed between baseline time spent under 90% SpO2 and 1-year changes of cardiometabolic risk markers. ODI, RDI, time spent under 90% of SpO2, triglycerides, homeostatic model assessment—insulin resistance, C-reactive protein, tumour necrosis factor α (TNFα) and interleukin-6 values were log transformed because of skewed distribution, and all analyses involving these data used log transformed data. Significance was set at p values <0.05. Analyses were carried out using SAS, V.9.2.
Results
Eighty-six per cent of men with visceral obesity involved in this ancillary study completed the 1-year intervention. The 11 men who dropped out of the lifestyle intervention did not differ at baseline from the 66 men who completed the programme, except for body mass index (BMI) (28.9±2.1 vs 30.9±3.2 in men who dropped out vs men who did not, p=0.04), TNFα (1.47±0.74 vs 1.02±0.47, p=0.01) and daily caloric intake (2608±538 vs. 3069±579, p=0.02). The 19 men with visceral obesity who completed the 1-year lifestyle intervention but did not have the 1-year sleep evaluation presented with lower heart rate (65±7 vs 70±8 for men who did not have the 1-year sleep evaluation compared with the others, p=0.05), triglycerides (2.20±1.02 vs 2.54±0.81, p=0.03) and fasting plasma insulin (151±89 vs 174±78, p=0.03) than other men at baseline. However, they were no different from the others after 1 year of intervention, except for fasting insulin which remained lower (100±60 vs 109±37, p=0.04).
One-year response to the lifestyle modification programme and changes in sleep-disordered breathing variables
Baseline characteristics of men with visceral obesity and their 1-year responses to the lifestyle intervention programme are reported in table 1. After 1-year of lifestyle intervention, they had lost 26.7% of VAT and had improved their cardiorespiratory fitness by 21.3%. When considering absolute changes, Epworth score, time spent under 90% of SpO2, ODI and RDI all decreased after 1 year of lifestyle intervention, whereas mean SpO2 increased.
Results of the lifestyle intervention in men with visceral obesity with baseline ODI below or above 10 events/h
To assess whether nocturnal oxygen desaturations could alter the response to a 1-year healthy eating physical activity/exercise lifestyle intervention, men with visceral obesity were classified into two groups according to their baseline ODI with a 10 events/h cut-off. Twenty-eight out of 77 men presented an ODI above 10 events/h at baseline (36%).
At baseline, men with nocturnal oxygen desaturations above 10 events/h (ODI 24±18 events/h) presented with a lower mean SpO2 (93±3 vs 95±1% for men with baseline ODI above vs below 10 events/h at baseline, respectively, p<0.001) and minimum SpO2 (80±8 vs 86±3%) than those with less frequent nocturnal oxygen desaturations (ODI 5±2 events/h), whereas they presented with higher RDI (32±21 vs 13±5 events/h) and time spent under 90% of SpO2 (8±13 vs 1±1% of sleep recorded time). There were no differences in Epworth scores. There were no differences at baseline between the two groups for anthropometric and metabolic variables, except for a higher area under the curve for glucose and a lower daily step count in those with baseline ODI above 10 events/h (table 2).
After 1 year of intervention, men with visceral obesity and a baseline ODI above 10 events/h showed smaller decreases in BMI, waist circumference, fat mass and triglyceride, and smaller increases in adiponectin and HDL cholesterol levels than men with baseline ODI below 10 events/h. Changes in daily step counts and in reported daily caloric intake after 1 year of intervention did not differ between the two groups.
When these comparisons were adjusted for baseline VAT volume and baseline daily step counts, the differences between subgroups remained for the 1-year changes in BMI, waist circumference, triglycerides and fat mass, whereas differences in 1-year changes in HDL cholesterol and adiponectin levels were no longer significant.
Associations between baseline sleep characteristics and changes in anthropometric and cardiometabolic risk markers
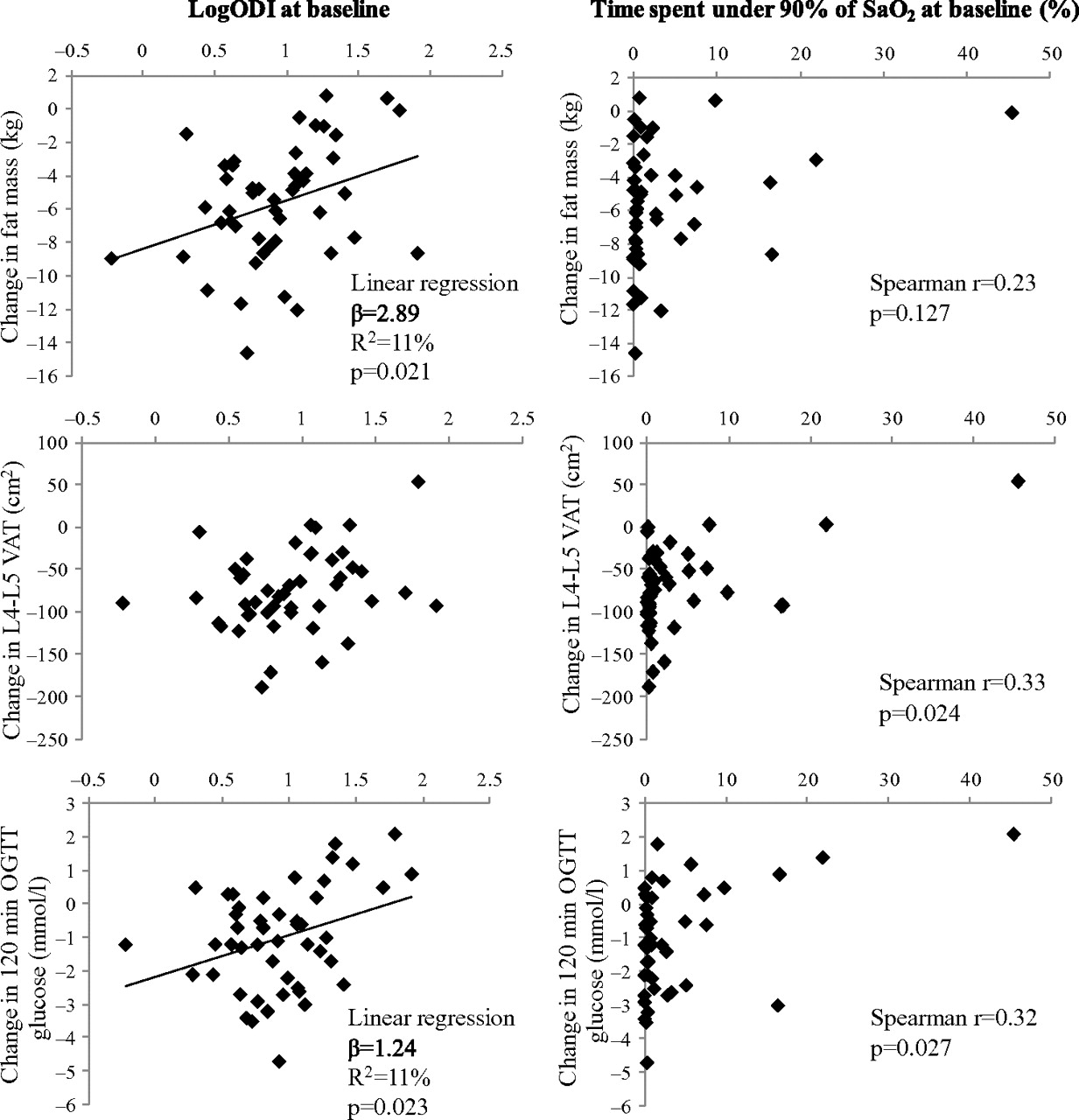
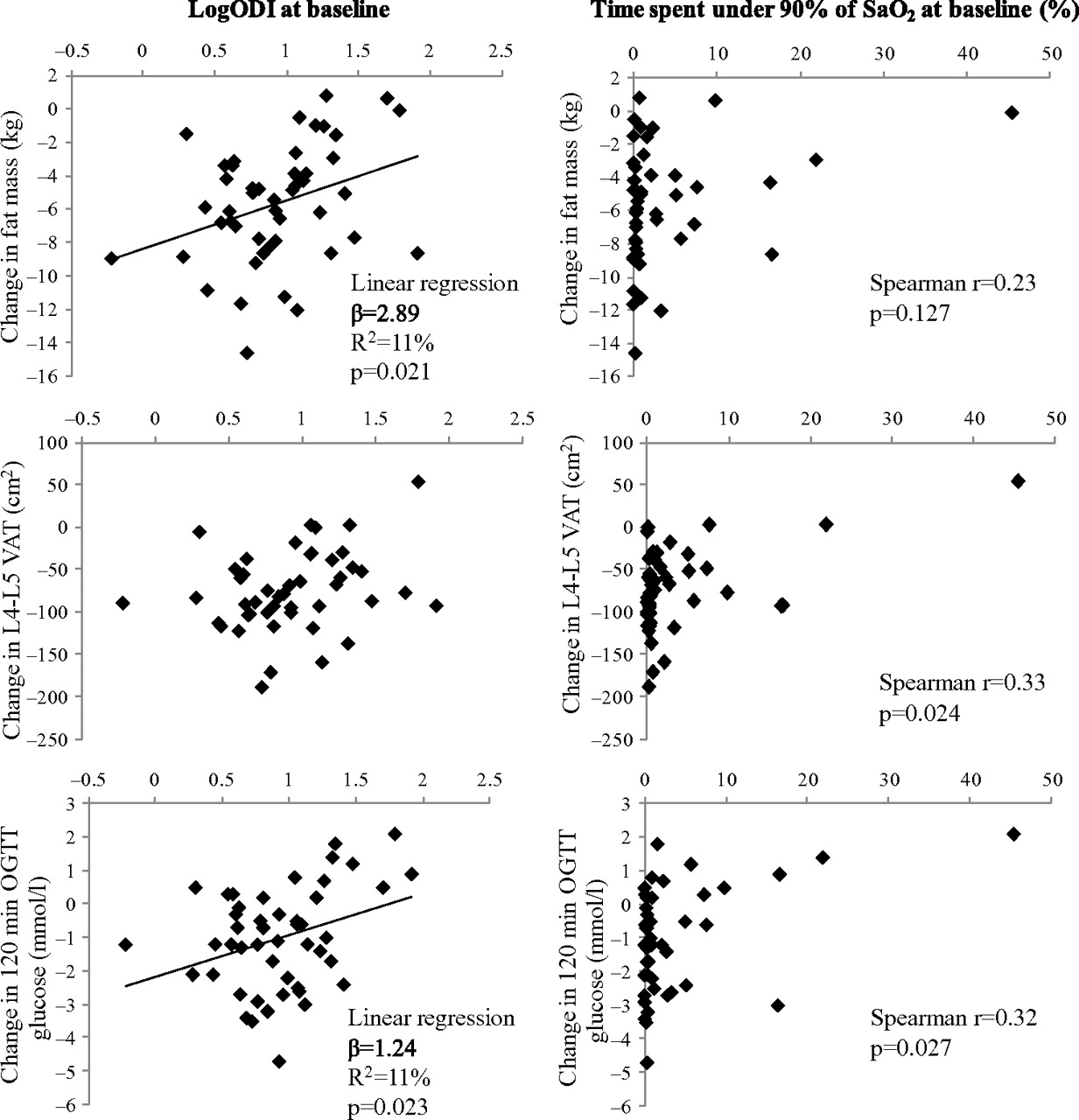
Finally, linear regression was quantified between baseline ODI (log transformed) and 1-year changes of cardiometabolic risk markers. Reductions in fat mass and 120 min OGTT were less substantial after 1 year of lifestyle intervention when baseline ODI was high (figure 2). Furthermore, Spearman rank correlation was analysed between baseline time spent under 90% SpO2 and 1-year changes in cardiometabolic risk markers: the longer the time spent under 90% SpO2 at baseline, the lower the reductions in 120 min OGTT and VAT.
{kind=link}
{kind=link}
Association between baseline sleep variables and 1-year changes in body composition/fat distribution, plasma glucose/insulin homeostasis. Linear regressions (left) were searched between baseline oxygen desaturation index (log transformed, logODI) and the 1-year changes in fat mass, visceral adipose tissue (VAT) and 120 min oral glucose tolerance test (OGTT)-glucose. Spearman rank correlations (right) were searched between time spent under 90% oxygen saturation (SaO2) at baseline and the 1-year changes in fat mass, visceral adipose tissue and 120 min OGTT-glucose.
Discussion
This study was conducted to assess whether having a sleep apnoea syndrome (defined by a baseline ODI above 10 events/h) at baseline could impede the response to the 1-year lifestyle intervention. Men with visceral obesity and a baseline ODI above 10 events/h presented with a lower decrease in BMI, waist circumference and fat mass after 1-year of intervention than men with a baseline ODI below 10 events/h, in spite of a similar compliance to the programme. Accordingly, these men presented smaller improvements in their cardiometabolic risk markers after 1 year. This study was not designed as a randomised trial to evaluate the effects of a lifestyle modification programme on nocturnal respiratory disturbances. Indeed, the efficacy of lifestyle modification programmes to improve nocturnal respiratory disturbances has already been well documented,11–15 ,23 and as expected, this 1-year lifestyle intervention was efficient in improving the cardiometabolic risk profile and nocturnal respiratory disturbances in these men. The dropout rate was 14% for participation in the lifestyle intervention programme and 19 men had invalid data or refused to undergo the home sleep-recording procedure at 1 year. These missing data are the consequence of the great burden associated with our extensive testing protocol in the SYNERGIE study. Thus, ancillary tests were more often turned down by participants than the tests planned in the main protocol. This is also why sleep respiratory disturbances were assessed by home-recording polygraphy rather than with polysomnography at the sleep clinic.
Efficiency of the lifestyle intervention programme in improving sleep-disordered breathing
There is strong evidence that body weight excess is a causal factor in OSAS.24 While most studies addressing the effect of weight loss on AHI have examined the effects of surgically induced body weight loss,7 ,23 data regarding the feasibility of a non-surgical body weight loss programme as a means to improve OSAS have also been reported.11 ,12 ,25 Recently, three randomised clinical trials have tested the efficiency of lifestyle intervention to improve sleep-disordered breathing. Tuomilehto et al11 have shown that in patients with mild OSAS (AHI 9.3 events/h at baseline), a lifestyle intervention programme based on a very low caloric diet for 3 months with subsequent dietary counselling for 1 year was efficient to induce significant decreases in body weight, waist circumference and AHI compared with patients receiving only non-specific information. Body weight and waist circumference losses were strongly related to reduction in AHI during the 12-month follow-up period, with a linear dose–response. In the Tuomilehto study, the mean decrease in AHI was 4 events/h in patients who lost 5–10 kg after 1 year of intervention. In the present study, we observed a decrement of 3 events/h in ODI in response to the same range of body weight loss. Foster et al12 conducted an ancillary study of the look AHEAD study, which included a polysomnographic study at baseline and after 1 year. Adults who were overweight or obese and had type 2 diabetes were randomised to intensive diet and exercise lifestyle intervention or to diabetes support and education. Patients in the first group lost more weight and had a greater decrease in AHI than patients assigned to the conventional support and education group. Baseline AHI was higher in patients enrolled in the look AHEAD ancillary study (22.9 events/h) than in those enrolled in the Tuomilehto study. Johansson et al13 conducted a 9-week very low caloric diet intervention consisting of liquid meals for 7 weeks followed by 2 weeks of progressive return to normal food in men with mild to severe OSAS (baseline AHI 37 events/h). Subjects also received counselling to help them increase their physical activity. Subjects of the intervention arm lost a mean of 20 kg in 9 weeks with a decrease in AHI of 23 events/h compared with subjects in the control arm. Following a 1-year weight maintenance programme, the mean body weight loss was 12 kg and the decrease of AHI was 17 events/h compared with baseline.15 In this study, the range of baseline ODI values was large, from 0.6 to 82.0 events/h. Our finding that nocturnal breathing disturbance indices could be improved by a healthy eating and physical activity/exercise programme in men with visceral obesity is in accordance with the results of the above-mentioned diet and exercise lifestyle intervention studies conducted in subjects with mild to severe OSA and in those who are overweight or obese and have type 2 diabetes.
Why OSAS impaired the response to the lifestyle intervention
Current opinion is that OSAS is a condition associated with a particular difficulty to lose weight and may even have a causal role in weight gain.7 Nevertheless, such an assumption is not based on robust evidence from the literature. Phillips et al26 showed that weight gain in the year preceding the diagnosis of OSAS was significantly higher than that observed in matched subjects free of OSAS, whereas Traviss et al27 found that 84% of patients having OSAS self-reported weight gain following the onset of symptoms. Both studies assessed body weight changes based on self-reported, retrospective data. However, a recent randomised controlled crossover study published by Sharma et al28 found that CPAP therapy improves features of the metabolic syndrome and body weight and VAT in patients with mild to severe OSAS, suggesting that OSAS has a deleterious independent effect on these parameters. This study found new evidence that despite similar compliance to the healthy eating, physical activity/exercise programme (the sleep apnoea status did not influence the decrease in daily caloric intake or the increase in daily step counts after 1 year), subjects having a baseline ODI above 10 events/h showed a smaller reduction in body weight, waist circumference and fat mass, and had less substantial improvements in cardiometabolic risk markers than those with a baseline ODI below 10 events/h.
Although further studies are needed to confirm these findings, OSAS-related resistance to weight loss strategies may be associated with alterations in sleep duration and/or continuity.29–31 Indeed, OSAS is characterised by recurrent episodes of partial or complete upper airways collapse occurring during sleep, which lead to sleep fragmentation, nocturnal oxygen desaturation and shorter total sleep time. Evidence from epidemiological studies suggests that short sleep duration is associated with weight gain.32 ,33 This observation has been reinforced by mechanistic studies evaluating the effect of sleep restriction on appetite and metabolism. These works have shown that sleep restriction is associated with increased appetite, increased ghrelin and decreased leptin levels.30 ,31 Beside the effect of sleep restriction by itself, some studies have shown that sleep fragmentation is associated with a decrease in insulin sensitivity and glucose utilisation in relation to increased sympathetic activity and cortisol levels.34 ,35 Indeed, OSAS is associated with an activation of the hypothalamic–pituitary–adrenal axis in response to stress caused by recurrent intermittent hypoxia, sleep fragmentation and frequent cerebral arousals during apnoeic events. This activation, which is corrected by CPAP treatment,36 could explain body weight gain or difficulty to achieve body weight loss in patients having OSAS. Finally, some studies suggest that patients characterised by a pronounced recurrent transient oxygen desaturation profile have a smaller energy expenditure relative to their body weight.37 This phenomenon could eventually be explained by the presence of a decrease in thermogenesis associated with an increase in oxygen desaturation severity of OSAS.38 However, this observation is controversial since one other controlled study found an increase in 24 h energy expenditure in patients with OSAS.39
The findings from these studies suggest why OSAS could affect body weight loss and improvement in cardiometabolic risk variables in people on a lifestyle intervention programme. However, further studies are needed to examine whether the effects demonstrated by sleep restriction and sleep fragmentation studies on energy metabolism are extendable to patients presenting with the intricate pathophysiology of OSAS. In light of these results, whether sleep apnoea treatment would improve the efficiency of a lifestyle intervention programme in patients with OSAS should also be examined. Kajaste et al25 conducted a 2-year cognitive-behavioural weight loss programme in patients with obesity (BMI>35 kg/m2) and OSAS. They randomised 16 and 15 subjects into two groups with or without concomitant CPAP therapy during the first 6 months. No difference in body weight loss was found between the two groups at 6 months or thereafter, although compliance to CPAP treatment was not controlled. Further trials are clearly needed extending the duration of CPAP treatment to the total duration of the weight loss programme and with adequate assessment of compliance and efficiency of CPAP treatment.
Study strengths and limitations
The primary outcome of this ancillary study was the changes in ODI after 1 year of lifestyle intervention in men with visceral obesity. Men having baseline ODI above or below 10 events/h were studied in post hoc analyses. The results have allowed us to identify the need for future studies that will address the response to lifestyle intervention of men with visceral obesity and untreated OSAS versus those of similar body weight and visceral fat without OSAS. Another limitation associated with this post hoc design is the imbalance between the two groups: 42 men having an ODI of less than 10 events/h and 24 having more than 10 events/h.
The particular strength of this study is the application of an integrated and synergistic lifestyle intervention programme which combined long-term moderate caloric restriction with an increase in moderate-intensity endurance exercise and occupational activity. This lifestyle modification programme was designed to be conducted in routine clinical practice, thus conclusions are extendable to the routine care of patients.
Conclusion
The findings of this study suggest that sleep-related breathing disorders are likely to impede the efficiency of a lifestyle intervention programme. Men with OSAS (ODI ≥10 events/h) at baseline had a smaller reduction in body weight and smaller metabolic improvements associated with the lifestyle intervention programme than men without OSAS (ODI <10 events/h). Further studies should address whether CPAP treatment should be administered during the period of the lifestyle intervention programme to increase body weight loss and improve the cardiometabolic risk markers associated with such programmes in people with visceral obesity and OSAS.
Acknowledgments
Dr Borel is a post-doctoral fellow supported by a fellowship from Agiràdom (Meylan, France) and the Rhône-Alpes region (France). Dr Paul Poirier is a senior clinical researcher of the Fonds de recherche en santé du Québec (FRSQ).
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Download Supplementary Data (PDF) - Manuscript file of format pdf
- Download Supplementary Data (PDF) - Manuscript file of format pdf
Footnotes
Funding This study was supported by the Canadian Institutes of Health Research: CIHR grant 89985 and the National Institute for Public Research.
Competing interests None.
Patient consent Obtained.
Ethics approval Ethics approval was provided by the Medical Ethics Committees of Université Laval and Institut universitaire de cardiologie et de pneumologie de Québec.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Airwaves