Article Text

Abstract
Background: Timeliness is an important dimension of health care quality. It is unclear whether timeliness improves clinical outcomes in patients with lung cancer.
Methods: This study systematically reviewed studies that described timeliness of care, examined associations between timeliness and clinical outcomes or tested an intervention to improve timeliness of care in patients with lung cancer. English language studies published between 1 January 1995 and 1 June 2007 were included. Two reviewers independently abstracted data on study methods, population, sample size, relevant time intervals and outcomes.
Results: 49 studies were identified that reported at least one time interval in lung cancer care, 18 studies that examined the association between timeliness and clinical outcomes and 8 studies that described interventions aimed at improving timeliness. Most studies were performed in European Union member countries, including 24 studies performed in Great Britain and Ireland. Median times to diagnosis (range 8–60 days) and times to treatment (range 30–84 days) often exceeded published recommendations. Three studies found that timely care was associated with better survival, eight found no association and four reported better survival in patients who received less timely care. Interventions that improved timeliness included nurse-led care coordination, multidisciplinary meetings via teleconference and a standardised expedited “two-stop” diagnostic process.
Conclusions: Times to diagnosis and treatment of lung cancer are often longer than recommended. Factors associated with timeliness have been incompletely examined, and it remains unclear whether more timely care improves outcomes.
Statistics from Altmetric.com
The care of patients with lung cancer requires complex coordination of services by medical and surgical specialists, healthcare administrators and social service providers. At the same time that health care in general is shifting towards more outpatient care, with fewer services requiring inpatient hospital stays, the complexity of lung cancer care has increased as more diagnostic and treatment options become available. The traditional approach of referring patients for consultation with multiple specialists in a sequential fashion often results in care that is perceived as slow, fragmented and poorly coordinated.
A number of guidelines and initiatives have been published to establish standards for timely care for patients with known or suspected lung cancer. These guidelines are primarily based on clinical opinion and relatively little has been published on the effects of these guidelines on processes of care.
In 1998 the British Thoracic Society (BTS) published specific recommended maximum time intervals for diagnosis and treatment in patients with lung cancer.1 In 2000 the UK National Health Service Cancer Plan provided goals for providing timely care to patients with all types of cancer.2 In 2000 the RAND Corporation also published quality indicators for timely diagnosis and treatment, focusing on the time from the first abnormal radiograph to diagnosis and from diagnosis to treatment.3 In 2003 the American College of Chest Physicians provided recommendations for the practice organisation of lung cancer care in the USA, with an emphasis on integrated multidisciplinary care.4 While timely care may contribute substantially to patients’ quality of life and emotional well-being, it remains unclear whether timely care also improves patient outcomes.
In this systematic review we aimed to summarise all recently published studies that described the timeliness of care in patients with lung cancer, identified factors that were associated with more or less timely care, or examined the association between the timeliness of care and lung cancer outcomes, including stage distribution and survival. In addition, we aimed to identify studies that evaluated interventions to improve the timeliness of care for patients with lung cancer.
Methods
Systematic methods were used to identify studies, assess eligibility for inclusion, evaluate quality, abstract data and synthesise results.
Search strategy and selection criteria
We searched MEDLINE to identify studies published between 1 January 1995 and 1 June 2007. Studies published before 1995 were excluded because they were included in a previous review5 and may be less relevant to current healthcare practices. We developed three separate search strategies to capture relevant studies that (1) described the timeliness of care in patients with lung cancer, (2) examined the association between timeliness of care and lung cancer outcomes and (3) described an intervention aimed at improving timeliness of lung cancer care (see Appendix). In addition, we manually searched reference lists of included studies and review articles and reviewed practice guidelines and systematic reviews. We included human studies published in the English language and excluded studies published only as abstracts.
All studies that included patients with known or suspected lung cancer were considered, including studies reporting patterns of care for patients with symptoms that could be suggestive of lung cancer or patients with abnormal imaging test results.
Data abstraction and quality assessment
One investigator (JKO) reviewed all titles and abstracts and excluded articles that were obviously irrelevant or contained no primary data. Additional studies were excluded after review of the full article. Two investigators (JKO and EMS) assessed quality and abstracted the following data elements from included studies: study design, patient population, sample size, relevant time intervals and outcomes. Disagreements were resolved by discussion and by consultation with the senior investigator.
For studies of timeliness of care to be included we required that (1) the study reported one or more time intervals in the process of lung cancer diagnosis and treatment and (2) at least 75% of patients were diagnosed with lung cancer or results for patients with lung cancer were reported separately. For studies that examined the association between timeliness and lung cancer outcomes, we also required that the study reported overall and/or disease-free survival, stage distribution, tumour size or resectability in relation to timeliness of care, in addition to criteria (1) and (2) listed above.
Studies of interventions were included if they described any intervention aimed at improving the timeliness of care for patients with lung cancer, provided that they met the inclusion criteria that we used for studies of timeliness. We did not include studies that described a multidisciplinary team meeting, or tumour board, as this approach has already been widely adopted in cancer care. Studies of multidisciplinary clinics or dedicated lung mass clinics were included.
Data synthesis
When available from published studies, we report the median and range or interquartile range (IQR) for relevant time intervals in lung cancer care. Mean time intervals were reported only when no other data were available from published studies. Heterogeneity in study methods and reporting of results precluded quantitative synthesis.
Results
Our search yielded 10 266 potentially relevant studies. We excluded 10 194 studies during the initial review, leaving 72 studies for further detailed review (fig 1). Nineteen studies were excluded after a full review and therefore 53 studies were included in the final analysis (see table in online supplement).

Search strategy results and study exclusions. Search strategies yielded a total of 10 266 unique studies, of which 53 are included in this review. Included studies were grouped into three overlapping categories based on reported results.
A total of 49 studies described at least one time interval in lung cancer care. Eighteen studies examined the association between timeliness and one or more outcomes, including 15 studies that examined survival,6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 4 studies that examined stage distribution11 16 21 22 and 1 that examined tumour growth.23 Eight studies that described an intervention to improve timeliness of care were identified.24 25 26 27 28 29 30 31
The majority of studies were performed in European Union member countries, including 24 studies performed in Great Britain and Ireland. Only five studies were performed in the USA, including one large study from Hawaii,32 one small study from Massachusetts33 and three studies conducted in US Veterans Affairs (VA) facilities.13 26 31 Four Canadian studies21 34 35 36 and four Japanese studies12 15 16 37 were identified, including several studies that examined delays in care after mass population-based screening. We also included two studies from Turkey,17 38 one study from Australia24 and one study from Malaysia.9
Overall, study quality was uneven (fig 2). A total of 11 population-based reports were identified,6 18 19 34 36 38 39 40 41 42 43 while most studies described care provided at tertiary care referral centres. Only nine studies enrolled patients prospectively.17 23 24 30 39 44 45 46 47 While many studies were limited by small sample sizes, eight studies included more than 1000 patients with lung cancer.11 14 29 32 34 35 36 43 In several studies basic demographic information was not reported, nor was information about histology or stage distribution. Information about the statistical analysis was often incomplete (fig 2).
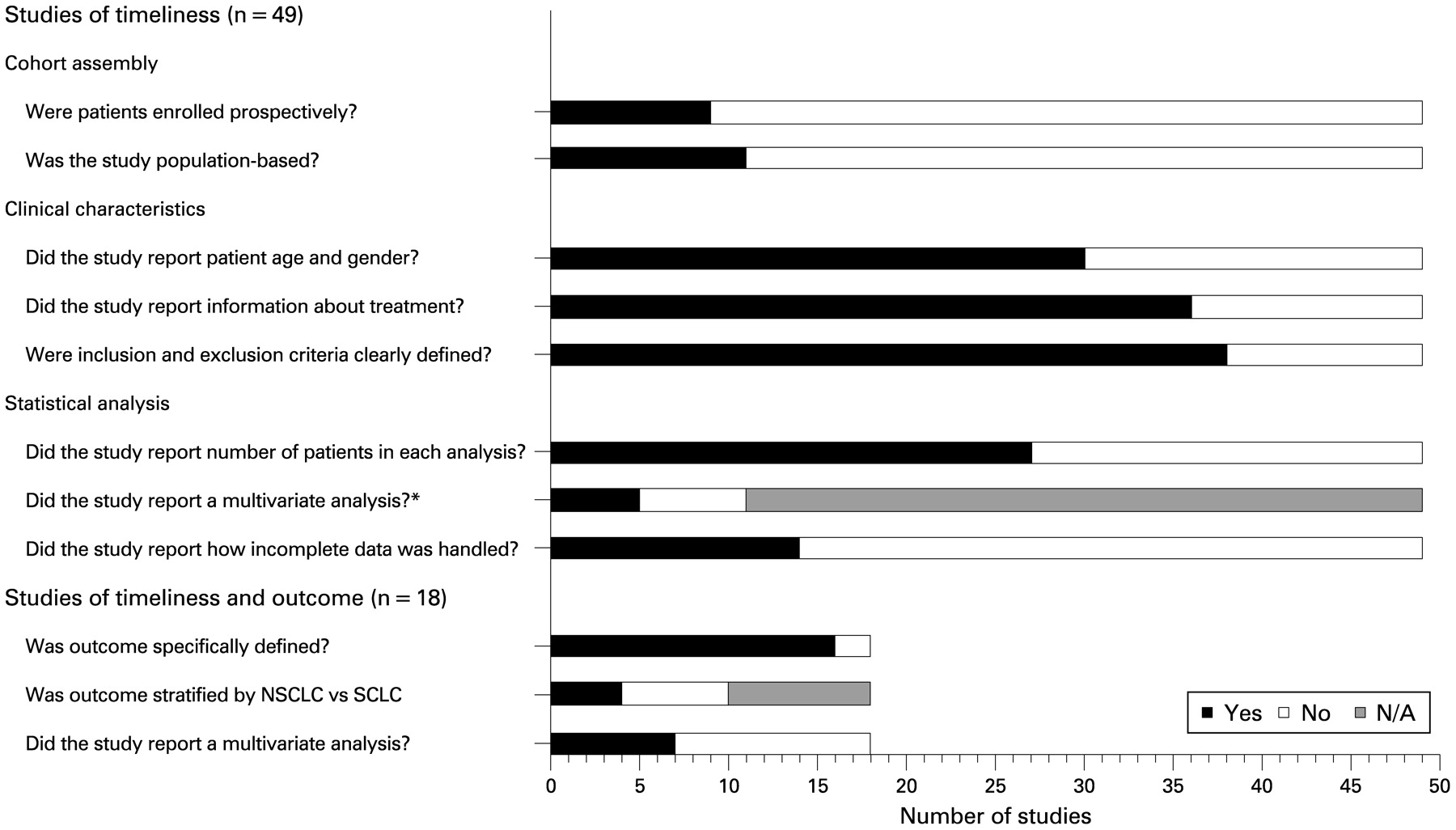
Study quality. Top: Number of studies that met each quality indicator for studies that described timeliness of care. Bottom: Studies that reported an analysis of clinical outcomes as a function of timeliness of care were assessed using additional quality criteria. *If the study examined predictors of timely care, did the authors report a multivariate analysis to control for differences between groups? NSCLC, non-small cell lung cancer; SCLC, small cell lung cancer.
Timeliness of lung cancer care
Forty-nine studies described at least one interval in the continuum from symptom onset to initial treatment. Reported median times from the primary care visit to referral for specialist evaluation were 13 days (range 0–21 days),48 16 days,6 33 days (IQR 12–68 days)49 and 33 days (range 0–477 days).39 Two studies demonstrated that patients often made multiple visits to their primary care physician before additional investigation were initiated.50 51 This was particularly evident in patients with superior sulcus tumours, who were often treated for presumed musculoskeletal shoulder pain before further evaluation took place.37 42
Adherence with existing guidelines for timeliness of lung cancer care was modest (table 1). In the eight studies reporting time from referral to first respiratory specialist visit, median times were all within the 14 days recommended by the NHS Cancer Care Plan, but seven studies reported a median time that exceeded the BTS recommendation for a maximum time of 7 days.6 10 19 20 29 41 55 Both guidelines have set target intervals for the maximum wait for all patients rather than median wait times. Three studies reported median times from specialist consultation to surgery that exceeded the 56-day maximum recommended by the BTS.21 26 54 The most commonly cited reasons for delay were the need for multiple diagnostic tests and consultations.
Recommended maximum time intervals and reported median delays in specialist consultation and treatment (in days)
The NHS National Cancer Plan targets a maximum interval of 1 month from diagnosis to treatment.2 In 5 of 11 studies the median time from diagnosis to treatment exceeded this recommendation and in several studies the median time approached or exceeded the 6-week maximum recommended by the RAND Corporation (table 1).3
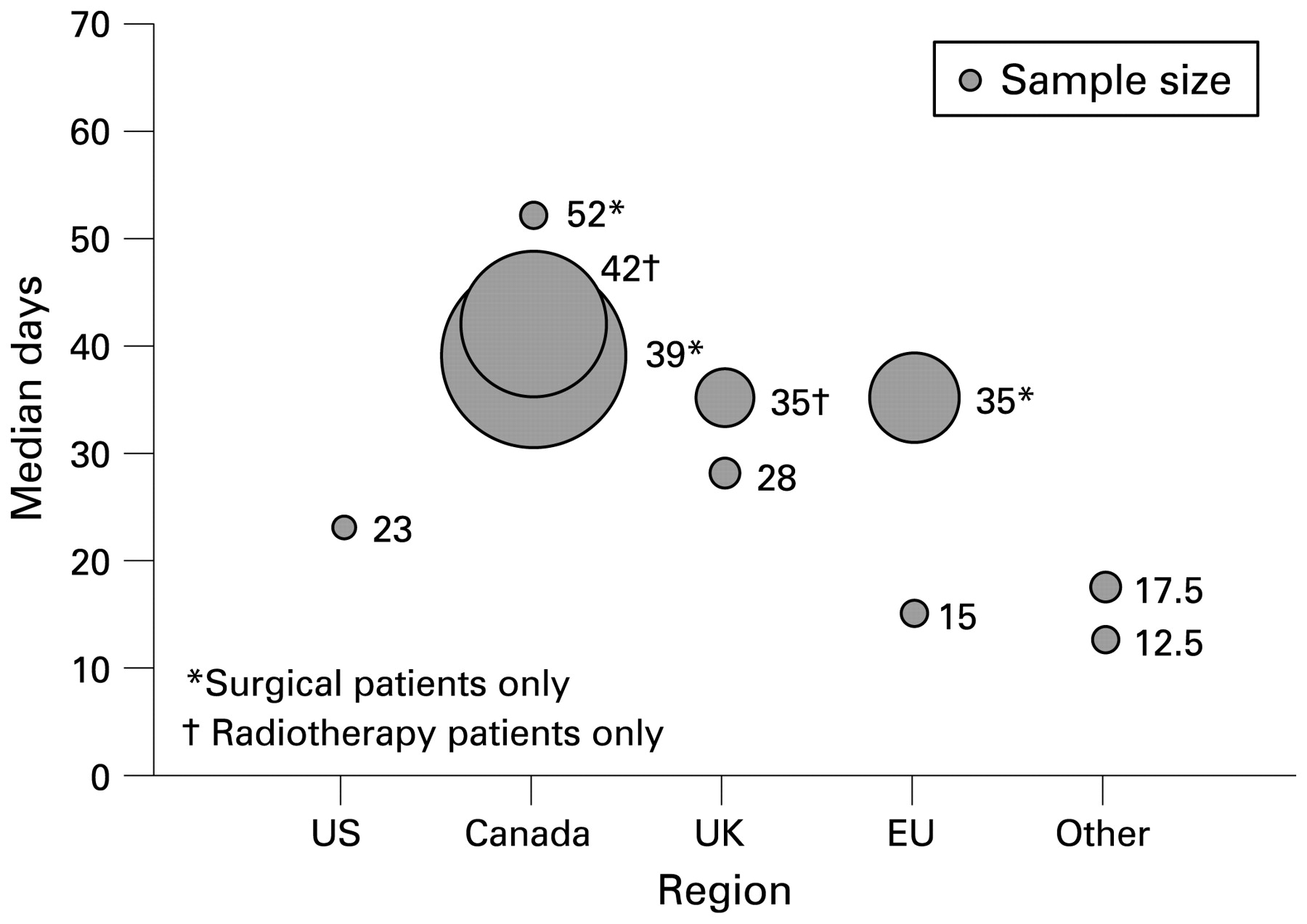
Median times from diagnosis to treatment were similar across geographical regions (fig 3). In general, longer median times from diagnosis to treatment were reported in studies that limited analysis to patients treated with surgery or radiotherapy, which also tended to have larger sample sizes.
{kind=link}
{kind=link}
{kind=link}
Distribution of median times from diagnosis to treatment. Sample size, patient cohort and reported median time from diagnosis to treatment varied widely among studies that reported this interval. Labels indicate reported median values for time from diagnosis to treatment. Bubbles indicate relative sample size, which ranged from 89 to 4366 patients. EU, European Union (excluding UK and Ireland); UK, United Kingdom and Ireland; US, United States.
Predictors of timely care
Fourteen studies reported an analysis that identified predictors of timely care or provided descriptive information about reasons for delays in care (table 2).6 7 17 18 34 35 36 42 45 46 49 52 54 57 Many studies examined the effect of age on timeliness of care, but the results were mixed.6 17 18 34 35 36 Patients with early-stage cancer often waited longer for a diagnosis, probably due to the need for multiple diagnostic tests to achieve a diagnosis.56 One Canadian study reported a tendency towards admitting patients with limited financial resources to the hospital, thereby expediting their care.34 Factors associated with less timely care included atypical symptoms, co-morbid conditions, teaching hospital setting, receipt of curative (versus palliative) radiotherapy, initial referral to a non-respiratory physician, requirement for multiple diagnostic tests and care received at more than one healthcare facility. Household income,34 35 36 52 gender,35 36 hospital volume,35 rural residence35 and distance travelled to obtain care36 52 were not associated with timeliness.
Variables associated with less timely care in lung cancer
Timeliness of lung cancer care and outcomes
A total of 18 studies examined the association between timely care and patient outcomes. Fifteen studies looked at the effect of timeliness on survival and reported mixed results, including eight studies that showed no association between timeliness and outcome.6 7 8 9 10 11 12 13
Three studies demonstrated worse survival in patients with delayed diagnosis and treatment, including two studies that included patients identified through population-based mass screening.14 15 16 Kashiwabara et al reported both an analysis of patients with tumours that were initially missed on screening but identified 1 year later on repeat screening, and an analysis of patients with correctly identified abnormalities who did not attend follow-up with a physician.12 16 Median survival was worse in those who did not follow up promptly and correlated with increases in tumour size. The hazard of death increased by 5.5% for each additional 1 mm in tumour size at the time of diagnosis.16 In another study of patients with lung cancer identified on a screening chest radiograph, Kanashiki et al found that survival was worse in patients who received a diagnosis more than 4 months after the initial abnormal chest radiograph.15 Buccheri et al also observed worse survival among patients with longer time from symptom onset to specialist referral.14
Paradoxically, four studies showed better median survival for patients who received less timely care.17 18 19 20 Annakkaya et al reported a statistically significant difference in survival when comparing patients with a symptom-to-diagnosis interval above and below 60 days, but not 45 or 90 days.17 Comber et al reported better lung cancer-specific survival in patients with longer times to treatment compared with those who waited less than 1 month.19 In the study by Myrdal et al, patients with more advanced disease experienced significantly shorter times to diagnosis and treatment.18 The authors reported a significant interaction between tumour stage and timeliness, suggesting that the increased mortality in patients with shorter time intervals was due to more advanced disease at the time of presentation. Similarly, Neal et al reported that survival was worse in patients with lung cancer who had urgent versus non-urgent referrals, and that patients with urgent referrals had more advanced stage disease at diagnosis.20
Four studies examined the effect of timeliness on stage. Three studies showed no effect,11 21 22 while one study demonstrated an association between longer delays and more advanced stage.16 Liberman et al limited their analysis to surgically treated patients in Canada and found no effect of preoperative delay on pathological stage.21
One study examined the relationship between tumour growth and delays in initiation of radiotherapy in 29 patients with non-small cell lung cancer in the UK.23 Comparing tumours seen on diagnostic and planning CT scans separated by a median interval of 54 days, the median increase in tumour cross-sectional area was 19% but tumour size increased by as much as 373% in one patient. Six patients became ineligible for curative treatment, all of whom were diagnosed with squamous cell carcinomas. This study supports the notion that tumour cell biology may be a determinant of the impact of delay on patient outcome, as all of the patients with adenocarcinomas were able to proceed with treatment as planned.
Improving timeliness of lung cancer care
We identified eight studies that described an intervention to improve timeliness of care and/or surgical resection rates.24 25 26 27 28 29 30 31 The studies evaluated different approaches to improving timeliness of care, including multidisciplinary clinics, nurse-led care coordination, telemedicine and a novel “two-stop” outpatient diagnostic process.
Three studies that evaluated patient care coordination through a dedicated lung mass clinic or a multidisciplinary clinic did not show a reduction in delays with either approach.24 26 31 In contrast, Davison et al reported a successful effort to improve communication between specialists and participation by thoracic surgeons in the UK by using telemedicine multidisciplinary meetings in the care of patients with suspected lung cancer.25 Leary and Corrigan reported a significant improvement in timeliness with a nurse-led intervention that included a detailed analysis of the local care process, restructuring of referral patterns and hospital-wide educational initiatives.28 Lewis et al performed a retrospective study of 1044 patients with suspected lung cancer referred to a single facility during the 12 months before and 24 months after introduction of the UK Department of Health urgent referral guidelines.29 The authors found that the median time from referral to first visit with a respiratory specialist increased from 7 to 9 days. The authors concluded that the “2-week wait” initiative did not achieve the primary objective of reducing waiting times for lung cancer care.
Two studies reported reductions in time to treatment using a “two-stop” diagnostic process for expediting investigation of patients with suspected lung cancer. Laroche et al described 275 patients treated at a single tertiary care facility in the UK.27 Patients received CT, biopsy and/or other diagnostic tests at the initial visit and a treatment plan was developed during a multidisciplinary meeting within 3 days. The median time from first specialist visit to surgery was reduced by 50%, and the overall successful surgical resection rate was 25%. Murray et al subsequently randomised 88 patients with suspected lung cancer to undergo investigation and treatment via a centralised “two-stop” diagnostic process or conventional diagnosis at the local hospital.30 Time from first presentation to treatment was 3 weeks in the centralised arm compared with 7 weeks in the conventional arm.
Discussion
Despite the increasing emphasis on efficient and timely delivery of health care, we found that reported times to diagnosis and treatment for patients with lung cancer in a variety of different healthcare settings are often longer than recommended by published guidelines.
In a previous review, Jensen and colleagues identified 16 studies published before 2001 that reported delays in lung cancer management.5 Like our study, they found considerable heterogeneity in study design, patient population and interval definitions, limiting comparisons across studies. They found very few published data on health system delays and little evidence that delays were associated with survival or stage.5
In this systematic review, limited conclusions can be drawn from the studies of timeliness of care and outcomes which revealed mixed and even paradoxical results. Studies were limited by referral centre bias and by inadequate methods for dealing with confounding variables such as age, stage, tumour histology, co-morbidities and the presence of symptoms at presentation. Most large studies were performed by using administrative databases with only surgical patients and included limited clinical information about tumour size, co-morbidities and adjuvant therapy. It is possible that some of the non-surgically treated patients excluded from these studies would have been eligible for surgical treatment had a diagnosis been made sooner. Smaller studies often included all patients with lung cancer and included more detailed clinical information, but typically were underpowered and often did not adjust for variables that might confound the relationship between timeliness and survival. Such confounding may explain the paradoxical results reported in several studies in which patients with the most timely care had the worst survival rates. In these studies, patients with advanced disease at the time of presentation are more likely to have symptoms and signs of malignancy and may be more likely to receive prompt diagnosis and palliative treatment due to earlier specialist referral and fewer diagnostic tests needed to achieve a diagnosis. These patients may also be more likely to receive supportive care only, and to die earlier than patients with early-stage disease. Additionally, some studies were potentially limited by lead time bias, especially studies that measured survival from the start of treatment.
Several studies examined ways to improve timeliness of care for patients with lung cancer. While the multidisciplinary clinic approach to care has been encouraged as a way to improve both timeliness and quality of care, there is little evidence that this approach actually improves timeliness of lung cancer care. Studies do show that multidisciplinary clinics are associated with increased rates of active treatment, including surgical resection and chemotherapy, and may therefore provide better quality medical care. The “two-stop” diagnostic process described by Laroche et al and Murray et al appears effective in significantly reducing diagnostic delay. The main limitation to this approach is that it requires a high level of care coordination by multiple specialty services. Lewis et al concluded that the UK “two-week wait” initiative failed to reduce wait times because the increase in urgent referrals burdened specialist services, leading to longer waits for patients referred non-urgently.
Our study has several limitations. We limited our literature search to a single computerised database and included only studies published in the English language. However, our MEDLINE search was comprehensive, and we also identified studies by scanning reference lists from included studies and recent reviews. Most of the studies were performed in European Union member countries, limiting conclusions that one can make about lung cancer care in non-European Union healthcare settings. In particular, only five studies were performed in the USA, including three carried out in VA hospitals. Direct comparison of timeliness in different countries and healthcare systems may be misleading as patterns of care vary within different regions. However, we believe that such comparisons are still valuable, particularly given the paucity of recommendations that address timeliness of lung cancer care.
While heterogeneity in study methods precluded us from performing a quantitative synthesis, the observation that time intervals were often longer than recommended in numerous and varied healthcare settings strongly supports the generalisability of our findings. However, we believe that future studies would benefit by using more standardised methods. In particular, we recommend that a standard definition for each relevant time interval be accepted.
We need more studies that describe lung cancer care in private hospitals, teaching facilities, county hospitals and Health Maintenance Organizations in the USA as most of the US population receives care in such facilities. Prospective studies with consecutively enrolled patients would reduce confounding due to selection bias, recall bias, missing data and variations in treatment practices. Studies should also examine the effect of patient factors, including race and ethnicity, on the timeliness of care.
While it remains unclear whether more timely care improves outcomes in lung cancer, improving timeliness is important independent of its ultimate effect on survival. Our patients expect, deserve and appreciate care that is timely, safe and effective.
Appendix: Medline search strategies
Studies of timeliness of lung cancer care
lung neoplasms/diagnosis[MESH] OR lung neoplasms/drug therapy[MESH] OR lung neoplasms/radiotherapy[MESH] OR lung neoplasms/surgery[MESH] OR lung neoplasms/therapy[MESH]
AND
time factors[MeSH] OR waiting lists[MeSH] OR delay[text word] OR Timeliness[text word] OR Time[text word] OR prognosis[MESH]
AND 1995/01/01[PDat]: 2007/06/01[PDat] AND Humans[Mesh] AND English[lang]
Studies of timeliness and outcome in lung cancer care
lung neoplasms[MESH] OR lung cancer*[text word]
AND
time factors[MeSH] OR waiting lists[MeSH] OR delay[text word] OR timeliness[text word]) AND
mortality[MeSH Terms] OR survival rate[MESH] OR survival analysis[MESH] OR survival[MeSH Terms]
AND 1995/01/01[PDat]: 2007/06/01[PDat] AND Humans[Mesh] AND English[lang]
Studies aimed at improving timeliness of lung cancer care
lung neoplasms[MeSH] OR lung cancer*[text word]
AND
delivery of health care[MESH] OR program development[MESH] OR management information systems[MESH] OR outcome and process assessment (health care)[MESH] OR referral and consultation[MESH] OR practice management[MESH]
AND
time factors[MeSH] OR waiting lists[MeSH] OR delay[text word] OR timeliness[text word] OR time[text word]
AND 1995/01/01[PDat]: 2007/06/01[PDat] AND Humans[Mesh] AND English[lang]
REFERENCES
Supplementary materials
Web only appendix 64/9/749
Files in this Data Supplement:
Footnotes
▸ A table of the studies included in the analysis is published online only at http://thorax.bmj.com/content/vol64/issue9
Funding This study was supported by the VA Office of Quality and Performance.
Competing interests None.
The views expressed in this paper are those of the authors and do not necessarily represent the views of the Department of Veterans Affairs.
Provenance and Peer review Not commissioned; externally peer reviewed.
Linked Articles
- Airwaves