Article Text

Abstract
Background: The frequency of clinical isolation of non-tuberculous mycobacteria (NTM) in the Netherlands is increasing, but its clinical relevance is often uncertain.
Objective: To assess the frequency and clinical relevance of isolation of NTM in four associated hospitals in a single region in the Netherlands.
Methods: Medical files of all patients from whom NTM were isolated between January 1999 and January 2005 were reviewed retrospectively. Diagnostic criteria for non-tuberculous mycobacterial disease published by the American Thoracic Society (ATS) were used to determine clinical relevance.
Results: 232 patients were found, from whom NTM were isolated from the respiratory tract in 91% of cases. Patients were mostly white men, with an average age of 60 years and pre-existing pulmonary disease. Fifty-three of 212 patients (25%) with pulmonary isolates met the ATS diagnostic criteria for pulmonary NTM disease; this percentage differed by species. Most patients were treated with rifampicin, ethambutol and clarithromycin. Treatment outcome for pulmonary NTM disease was suboptimal but differed by species: overall, improvement was seen in 67% of treated patients, but in only 50% of those with pulmonary M avium disease. Lymphadenitis was the most common extrapulmonary disease type.
Conclusions: Twenty-five per cent of all patients with pulmonary NTM isolates met the ATS criteria. Clinical relevance differs by species. NTM isolation increases over time. Species distribution differs from that of neighbouring countries and the M avium complex isolates have traits different from those reported in the USA. Adherence to diagnostic and treatment guidelines can be improved.
Statistics from Altmetric.com
The clinical isolation of non-tuberculous mycobacteria (NTM) increases in many countries where the incidence of tuberculosis is decreasing, with marked geographical differences in the species encountered.1–3 The NTM are often opportunistic pathogens, capable of causing disease in patients with impaired immunity, either local due to pre-existing pulmonary disease or systemic—for example, haematological malignancy, immunosuppressive drug treatment or HIV/AIDS.1 The clinical relevance of isolated NTM is often unclear. The NTM are common in the environment and can survive in flowing water systems.4 Moreover, NTM resist common disinfectants.5 Thus, pseudo-infection due to occasional presence of NTM in clinical samples as a consequence of contamination of medical tools should always be considered.1 6 7
To differentiate true infection from pseudo-infection, and establish the clinical relevance of an NTM isolate, is of paramount importance since treatment of NTM disease is time consuming and often complicated. To assist in this differentiation, the American Thoracic Society (ATS) established general criteria for the diagnosis of pulmonary non-tuberculous mycobacterial infection (box 1).1
Box 1: Summary of the American Thoracic Society diagnostic criteria for pulmonary non-tuberculous mycobacterial infection1
Clinical
Pulmonary symptoms, nodular or cavitary opacities on chest radiograph, or a high-resolution CT scan that shows multifocal bronchiectasis with multiple small nodules.
and
Appropriate exclusion of other diagnoses.
Microbiological
Positive culture results from at least two separate expectorated sputum samples. (If the results from the initial sputum samples are non-diagnostic, consider repeat sputum acid-fast bacillus (AFB) smears and cultures.)
or
Positive culture results from at least one bronchial wash or lavage.
or
Transbronchial or other lung biopsy with mycobacterial histopathological features (granulomatous inflammation or AFB) and positive culture for non-tuberculous mycobacteria (NTM) or biopsy showing mycobacterial histopathological features (granulomatous inflammation or AFB) and one or more sputum or bronchial washings that are culture positive for NTM.
Expert consultation should be obtained when NTM are recovered that are either infrequently encountered or that usually represent environmental contamination.
Patients who are suspected of having NTM lung disease but who do not meet the diagnostic criteria should be followed up until the diagnosis is firmly established or excluded.
Making a diagnosis of NTM lung disease does not, of itself, necessitate the institution of treatment, which is a decision based on potential risks and benefits of treatment for individual patients.
We performed a retrospective case study to assess the prevalence and clinical relevance of NTM isolated in the four associated training hospitals of the Nijmegen-Arnhem region, the Netherlands, using the ATS diagnostic criteria to differentiate NTM disease from pseudo-infection or contamination.
METHODS
To determine clinical relevance, we examined medical records of all inpatients and outpatients in four collaborating hospitals in the Nijmegen-Arnhem region of the Netherlands from whom NTM were isolated between January 1999 and January 2005. We recorded demographic, clinical and microbiological data and status according to the diagnostic criteria for pulmonary NTM disease by the ATS.1 We considered pulmonary isolates clinically relevant if the patient met the ATS diagnostic criteria in the absence of evidence of other pulmonary infections.
For patients treated for NTM disease, we defined cure as symptomatic improvement and reversion to negative cultures sustained throughout our follow-up period. We focused on pulmonary isolates.
The Dutch National Institute for Public Health and the Environment (RIVM) subjected isolates of all patients to laboratory diagnosis. The RIVM is the national reference laboratory that provides identification, drug susceptibility testing and genotyping of mycobacterial isolates for all hospitals in the Netherlands. To identify NTM, the INNO-LiPA MYCOBACTERIA v2 (Innogenetics, Gent, Belgium) reverse line blot assay was used, after ruling out membership of the M tuberculosis complex using a Hain GenoType MTBC line probe assay (Hain Lifescience, Nehren, Germany). If no species-specific result was obtained, 16S rDNA gene sequencing (151 bp hypervariable region A) was performed. Before 2004, 16S rDNA gene sequencing was performed, after ruling out membership of the M tuberculosis complex or M avium complex using the AccuProbe MTB and M avium complex DNA probe kits (GenProbe, San Diego, USA). Sequencing results were compared with the GenBank (National Center for Biotechnology Information, http://www.ncbi.nlm.nih.gov (accessed 27 March 2009) database. A Pearson χ2 test was used for statistical correlations. The regional ethics committee approved the study.
RESULTS
We found 232 patients with NTM isolates, mostly from the respiratory tract (n = 212, 91%). Primary isolates were cultured from sputum (n = 158; 75%), bronchoalveolar lavage samples (n = 47; 22%) and lung biopsy specimens (n = 7; 3%). The annual number of patients from whom NTM were isolated rose during our research period, mainly owing to an increase in pulmonary isolates, especially M avium complex (MAC) isolates (fig 1). The annual percentage of patients meeting the ATS criteria did not change.

Total number of patients with non-tuberculous mycobacteria isolates, per year and isolation site. MAC, M avium complex.
Table 1 presents the baseline characteristics of the 212 patients with pulmonary NTM isolates.
Fifty-three patients (25%) met the ATS diagnostic criteria and were thus likely to have pulmonary NTM disease. Of the 159 patients who did not meet the ATS criteria, 146 (92%) failed to meet microbiological criteria and 149 (94%) failed to meet radiological criteria. For these patients, follow-up for a mean duration of 47 months (range 29–98 months) did not yield additional evidence of NTM disease.
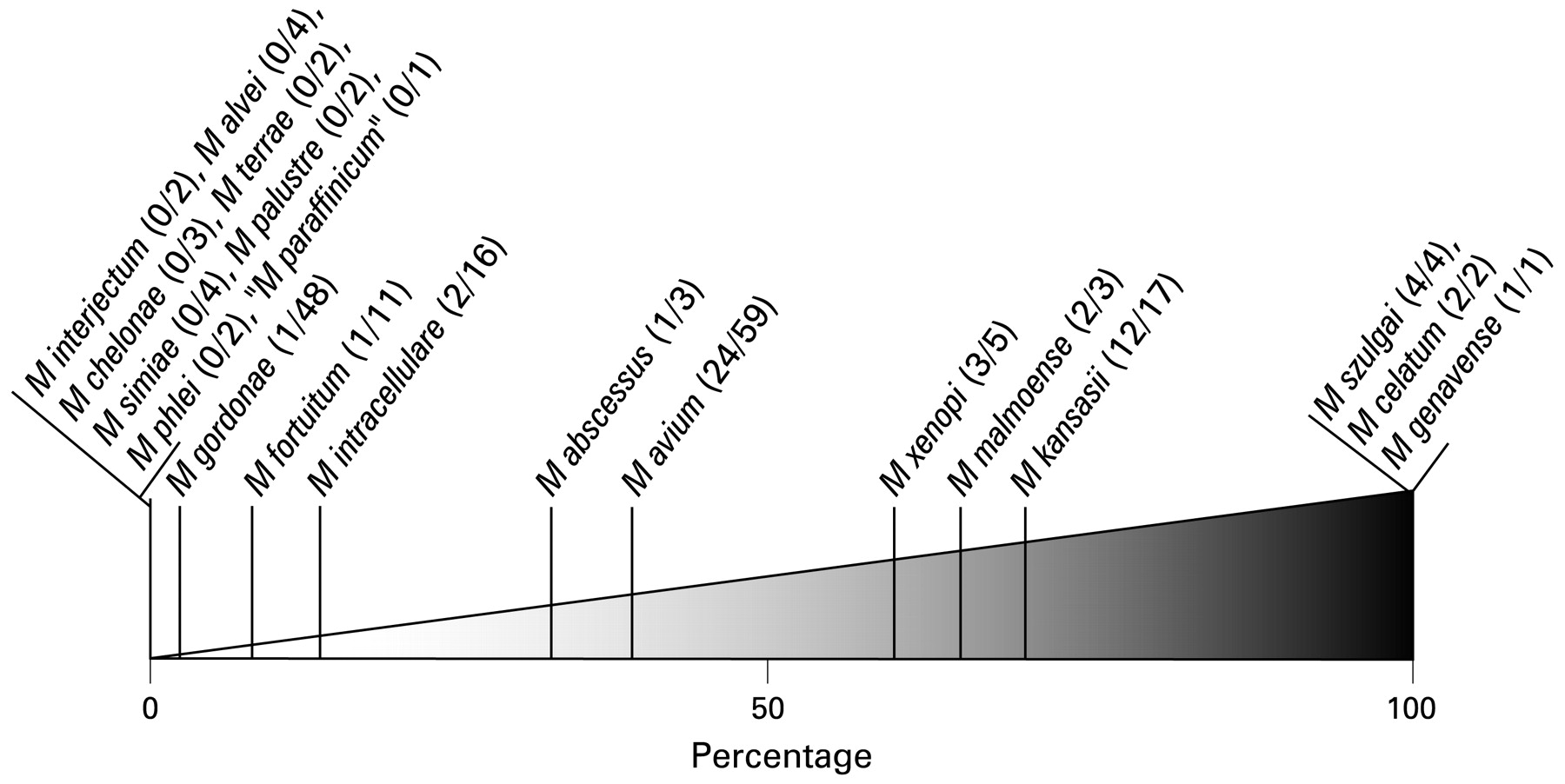
Figure 2 visualises the clinical relevance of the various NTM species, defined by the percentage of patients who met the ATS diagnostic criteria. Four cases of pulmonary NTM disease were actually relapses of disease episodes before our study period (two M avium, one M xenopi, one M kansasii).
{kind=link}
{kind=link}
Clinical relevance of pulmonary non-tuberculous mycobacteria isolates in this study, per species. (x/y), number of patients who met the American Thoracic Society diagnostic criteria/total number of patients per species.
Eighty-five patients (40%) had MAC isolates (59 M avium, 16 M intracellulare, 10 other MAC) of whom 26 (24 M avium, 2 M intracellulare; 31%) met the ATS diagnostic criteria. M avium isolation was clinically more relevant than M intracellulare (24/59 = 41% vs 2/16 = 13% of patients met the ATS diagnostic criteria). A radiographic presentation with fibrosis and cavities was more prevalent than nodular bronchiectatic disease (12 vs 3 cases for M avium and one case each for M intracellulare).
Whereas MAC was most frequently seen, the degree of clinical relevance was higher for isolation of M malmoense (2/3), M kansasii (12/17, 71%), M xenopi (3/5), M szulgai (4/4), M celatum (2/2) and M genavense (1/1; fig 2).
Symptoms recorded at presentation varied widely; only fever (p = 0.014, OR = 2.422, 95% CI 1.179 to 4.978) and fatigue (p<0.001, OR = 3.477, 95% CI 1.721 to 7.024) at presentation were associated with meeting the ATS diagnostic criteria (table 1). Chest radiographs were performed for 206 of the 212 patients and abnormalities were noted in 161 patients (78%; table 1). Abnormalities did not differ significantly by NTM species. Three patients with pulmonary NTM disease presented with a pulmonary mass, mimicking malignancy. Computed tomography (CT) scans were performed in 107 patients (50%); among patients meeting the ATS diagnostic criteria, five cases of fibrocavitary disease and six cases of nodular-bronchiectatic disease were noted in patients with inconclusive chest radiographs. On chest radiographs, these cases of fibrocavitary disease presented with dense air-space opacities; the nodular-bronchiectatic disease appeared as coarse linear scarring.
Drug treatment for mycobacterial infection was started in 44 patients; 31 started treatment for tuberculosis (TB) and switched to an NTM treatment regimen, 13 patients received standard TB treatment only. Of these 44 patients, 30 met the 1997 ATS diagnostic criteria available during the study period.8 Among those 30, 20 (67%) were cured, defined by symptomatic improvement and reversion to negative cultures, five died during treatment (three with M avium, one with M intracellulare, one with M xenopi disease; 17%) and five had a relapse after treatment (four with M avium, one with M celatum disease; 17%) The mean interval between the end of treatment and culture-proven relapse was 31 months (range 23–44). Of 14 patients treated for pulmonary M avium disease, only seven improved. The regimens used mostly consisted of rifampicin and ethambutol, despite frequent in vitro resistance (15/25 primary isolates were resistant to rifampicin, 18/25 to ethambutol; five were not tested); isoniazid was added in 11 patients (despite in vitro resistance in all cases), clarithromycin in 19, ciprofloxacin in four. Clarithromycin and ciprofloxacin were used only in patients with susceptible isolates. Three patients received 6 months of standardised TB treatment only. The mean treatment duration was 13 months (range 1–37). Three patients received additional surgical treatment that consisted of resection of a solitary pulmonary mass in two and lobectomy for persisting fibrocavitary disease in one; all three were cured. The mean duration of follow-up after treatment was 34 months (range 17–91).
Treatment was not given in 168 patients, though eight of them met the 1997 ATS diagnostic criteria.8 Four patients were considered to have too few symptoms or radiographic deterioration, one refused treatment and one patient spontaneously reversed to negative cultures. Slow radiographic deterioration of pulmonary disease was apparent in all seven persistently symptomatic and culture-positive, untreated patients.
During the study period, NTM were isolated from extrapulmonary samples only of 20 patients. Lymphadenitis was the most common extrapulmonary NTM disease type; six children and one elderly woman had cervical lymphadenitis (three M avium, two M malmoense, one M intracellulare, one M haemophilum) and one patient with AIDS (CD4 count 1) had axillar and mediastinal lymphadenitis with extensive abscess formation, caused by M gordonae. We recorded three cases of skin infection: two caused by M marinum in fish tank owners and one by M malmoense in a patient with haematological malignancy. We also noted single cases of M kansasii tenosynovitis in a gardener, M abscessus otomastoiditis after tympanostomy tube placement in a child and disseminated M avium disease in an AIDS patient (CD4 count 40). The remaining six patients had MAC isolated from the digestive tract, in the absence of further evidence of NTM disease.
DISCUSSION
Twenty-five per cent of all patients in this study had pulmonary NTM disease according to the ATS diagnostic criteria, and the clinical relevance differed significantly by species (fig 2). Isolation of M malmoense, M xenopi, M szulgai, M kansasii, M celatum and M genavense warrants special attention, as this usually reflects true NTM disease; an observation confirmed in previous studies.1 Although in the current study the number of isolates of many species is too low to permit firm conclusions, similar rates of clinical relevance have already emerged for M xenopi (21/45 patients; 47%), M chelonae (7/35; 20%), M abscessus (13/39; 33%), M simiae (3/28; 11%) and M szulgai (11/15; 73%) in nationwide studies of pulmonary isolates in the Netherlands.9–12 These data and the additional data in our current study strengthen a presentation such as that shown in fig 2. The 25% of patients who met the ATS criteria is similar to the 33% recently found in a Canadian referral centre study, 25% recorded among patients in Korea and the results of earlier studies reviewed by Marras and Daley.2 13 14
A difference in clinical relevance by species has also been noted in the recently published Korean study with results similar to ours, except for a very limited relevance of M szulgai (2/32 patients; 6%) and M celatum (1/11; 9%).13 These differences in clinical relevance between NTM species emphasise the major role of the bacteriological laboratory in the management of these emerging infections; correct identification of NTM isolates is a prerequisite for correct patient handling. These apparent regional differences in clinical relevance of NTM species require further study.
The ATS diagnostic criteria are based on experience with M avium, M kansasii and M abscessus1; their applicability to less studied species may be limited.1 9 The clinical applicability of the ATS criteria is supported by those patients who did not meet the ATS criteria and who had no clinical event or new radiological events during follow-up. Very few follow-up cultures were performed (table 1), although this was advocated in the ATS statement available during the study period.8
Although for some species the small number of isolates decreases the weight of the conclusions of the analysis, the difference in clinical relevance of the various NTM species may mean that for the species to the left of fig 2 the ATS criteria should be very strictly applied or even be made more stringent, whereas among the upper half (50–“100”% clinical relevance) a diagnosis of NTM disease may be justified after the first positive culture.
The increase in the annual number of patients from whom NTM were isolated (fig 1) is a cause for concern and has also been noted in previous studies.1 2 13 15 This increase was often thought be related to improvements in laboratory techniques; in the Netherlands, the use of (automated) liquid culture systems increased during the study period.1 16 A recent study, however, demonstrated that skin sensitisation to M intracellulare has also increased significantly over recent decades in the USA, consistent with observed increases in the rate of pulmonary NTM infections.17 Several aspects may influence this increase in NTM isolation. First, the Dutch population, as in many developed countries, is ageing and an increasing prevalence of chronic obstructive pulmonary disease is observed.18–20 The baseline characteristics of our study group, predominantly men with an average age of 60 years, similar to previous NTM studies in societies with low HIV prevalence,1 13 15 reflect these changes. Second, for chronic inflammatory diseases, immunosuppressive drugs, including tumour necrosis factor α neutralising agents, are increasingly used. Both these aspects may have an impact on the future prevalence of NTM disease. In addition, the exposure to aerosols of tap water may have increased over time, as frequency of showering has risen dramatically over recent decades. The minor role of HIV infection probably reflects the low prevalence of HIV infection in the Netherlands, compared with chronic pulmonary disease, and the advent of highly active antiretroviral treatment. This limits the number of cases of severe HIV immunosuppression and its co-infections,21 which may be reflected in the decreasing NTM isolation from extrapulmonary samples (fig 1). Besides, the hospitals participating in the study are situated in the eastern part of the Netherlands, where HIV incidence is lower than in the more urbanised western part.22
The limited associations between symptoms, chest radiography results and NTM disease according to the ATS diagnostic criteria underline the fact that diagnosis of NTM remains difficult. Hence, the NTM merit special attention by doctors and microbiologists.
Despite inherent limitations, the species found in this study and their frequencies probably reflect the current epidemiological situation for NTM in the Netherlands. This situation is remarkably different from nearby southeast England, where M xenopi is most common and Scotland and Scandinavia, where M malmoense is especially prevalent.1 14 23 The species distribution and clinical relevance among MAC isolates seen in this study differs from recent reports from the USA where M intracellulare is the more common respiratory pathogen,1 clinically more relevant than M avium in non-HIV patients,24 and nodular-bronchiectatic pulmonary MAC disease, associated with postmenopausal immunocompetent women, is as prevalent as cavitary disease.24 Possibly, the predominance of M avium and cavitary disease in our study group are inter-related; different MAC subtypes are known to cause different disease types in humans.25 Cases of nodular-bronchiectatic disease may have also been missed owing to the infrequent use of CT scanning and small number of follow-up cultures performed; diagnosing this paucibacillary disease type generally demands prolonged, intense follow-up.1 Alternatively, since we used hospital inpatient and outpatient file review, cases of nodular-bronchiectatic disease may have been missed as they are less often referred to hospitals for diagnosis, owing to a more indolent clinical course1 compared with cavitary MAC disease.
Previous studies have recorded high degrees of clinical relevance of M kansasii, comparable to the 71% in this study.14 Whereas the latest ATS statement states that for M kansasii the treatment decision may be based on a single positive culture in select cases,1 we recorded single positive sputum cultures in five patients with non-suspect radiographic changes and repeatedly negative follow-up cultures. This would have meant an unnecessary treatment for these patients when applying the new ATS criteria.
We observed possible instances of both undertreatment (not treating those who meet the diagnostic criteria) and overtreatment (treatment of those who do not meet diagnostic criteria), as well as the use of treatment regimens that have never proved to be effective. This may harm patients. This, as well as the fact that few (high-resolution) CT scans and follow-up cultures, both strongly advocated in the ATS criteria,1 8 were performed in patients with NTM isolates in non-cavitary pulmonary disease, could reflect a lack of knowledge of and experience with the diagnosis and management of NTM disease in doctors, or clinical circumstances not captured in our file review. All these aspects emphasise the need for centralisation of knowledge, experience and care for patients with (suspected) NTM disease or increased expert consultation.
Treatment duration recorded in our study was not in accordance with the British Thoracic Society (BTS) and ATS guidelines.1 26 A favourable outcome for 67% of patients with pulmonary NTM disease is higher than the 36% observed in the recently published BTS clinical trial comparing regimens with clarithromycin or ciprofloxacin as adjuncts to rifampicin and ethambutol.27 In that trial, patients with MAC and M xenopi had worse outcomes than those with M malmoense.27 The differences in treatment outcome between our study and the BTS trial may result, first, from our more lenient definition of “cure”, second, our limited follow-up period and finally, the NTM species causing pulmonary disease in our patients. Whereas the first trials of macrolide-based regimens in pulmonary MAC disease in HIV-negative patients in the USA reported cure rates of 59–92%, with comparable definitions of cure,1 the outcome of treatment for pulmonary MAC disease seen in our study and the BTS trial was disappointingly poorer. The treatment results, over-representation of men and cavitary disease, MAC species distribution and clinical relevance all suggest differences in MAC organisms encountered in the USA and Europe.
Although, generally, outcome of NTM treatment is suboptimal,1 various factors may have influenced our results. First, the conditions predisposing to NTM disease influence the outcome of the patient. Second, the 1997 ATS diagnostic criteria8 available to doctors in the study period might not have selected the group of patients who would have benefited from treatment. More patients meet the recently published criteria,12 though herein it is stated that meeting the criteria does not of itself necessitate treatment.1 Still, this may lead to improved selection of patients to receive treatment and thus improve outcome rates. In this perspective, the term under-treatment will become invalid. Third, previous trials for pulmonary MAC disease have recorded better treatment outcome using similar definitions, but in a different MAC population. In our group more patients had cavitary disease, which in general is associated with a worse treatment outcome.1 Finally, one of the centres incorporated in this study is a referral centre for NTM disease treatment, which may create a selection bias.
Extrapulmonary disease was rare, though its overall frequency (9%) and distribution of disease types are in line with previous studies, summarised in the recent ATS statement.1
In conclusion, clinical isolation of NTM was relevant in 25% of the 212 patients with pulmonary isolates. Clinical relevance differs markedly by species and there are important regional differences in species distribution and relevance. This, as well as the rising isolation rates of NTM, warrants special attention by doctors and microbiologists. Treatment outcome of pulmonary NTM disease was disappointing. Both overtreatment and insufficient treatment were noted. Extrapulmonary NTM disease is rare. Actions to increase awareness of the ATS diagnostic criteria and management guidelines and centralisation of NTM disease management are strongly recommended.
REFERENCES
Footnotes
Competing interests: None.
Ethics approval: Regional ethics committee approval obtained.