Article Text

Abstract
Background: Evidence for improved exercise tolerance or relief of breathlessness by short term use of oxygen before or after exercise in patients with chronic obstructive pulmonary disease (COPD) is scant, and guidelines for this treatment are lacking despite widespread provision in the UK.
Methods: The effect of oxygenation either before or after exercise on perception of breathlessness and walk distance was studied in a group of patients with moderate to severe COPD (mean forced expiratory volume in 1 second (FEV1) 34% of predicted, mean 6 minute walk distance on air 283 m), all of whom desaturated by at least 4% on submaximal exercise. Oxygen (28%) or air was delivered double blind and in random order, either for 5 minutes before a standard 6 minute walk test (n=34) or for 5 minutes following the end of the test (n=18). Exercise tolerance was measured as the distance achieved and breathlessness was assessed using visual analogue scales (VAS) which were scored before and after exercise and during recovery.
Results: No increase in mean walk distance after oxygen (288 v 283 m) and no improvement in mean breathlessness scores (58 v 54 mm) or recovery times occurred with oxygen taken either before (177 v 184 seconds) or after exercise (182 v 151 seconds).
Conclusions: This group of patients with COPD derived no physiological or symptomatic benefit from oxygen breathed for short periods before or after submaximal exercise. Domiciliary oxygen should only be prescribed for such patients if they have shown objective evidence of benefit on exercise testing.
- domiciliary oxygen
- breathlessness
- chronic obstructive pulmonary disease
Statistics from Altmetric.com
The provision of domiciliary oxygen by cylinder for the relief of breathlessness is widespread in the UK. The number of prescriptions issued for cylinders and associated equipment (633 000) has risen by over 70% in the last decade, the annual cost exceeding £11 million in 2001–2002.1 Many of these prescriptions are for the relief of breathlessness in patients with chronic obstructive pulmonary disease (COPD), and the cost is not far short of that for the provision of long term oxygen by concentrator.
There is good evidence of modest benefit from oxygen at rest2 and during exercise3–7 in many patients with COPD. However, there is little evidence as to whether patients with COPD can benefit from short periods of oxygen before or immediately after exertion despite widespread provision for use in this way, and patients are frequently given little or no advice about how to use their oxygen. Most use it while breathless after exertion while a smaller number pre-dose; flow rates and duration of use vary.8 There is a need for further studies to inform practice—and particularly guidelines9—in this area because previous studies of oxygen breathing immediately before exertion in patients with COPD have used a spectrum of oxygen flow rates, modes of exercise, and outcome measures and have shown conflicting results in terms of improvements in performance and in severity of dyspnoea during the ensuing exertion.4,10–12 Studies of oxygen breathing during recovery from exertion12,13 have also used disparate methodologies and have shown only very modest benefit after short burst or intensive exertion.
We have therefore re-examined this topic, using oxygen flow rates typical of cylinder based systems of supply, exercise protocols, and indices of dyspnoea which have been shown to be valid and reproducible in COPD patients with impaired exercise tolerance14 and a cohort of patients with severe COPD and exercise desaturation who might be expected to benefit from oxygen.
METHODS
Subjects
Patients were recruited from two hospital outpatient clinics in the Greater London area on the basis of spirometric evidence of fixed airflow obstruction and a clinical history of COPD which had been stable for a minimum of 4 weeks. Forty two patients volunteered to take part. The inclusion criteria were forced expiratory volume in 1 second (FEV1) less than 60% of predicted, with less than 15% reversibility to inhaled salbutamol, a smoking history of more than 20 pack years, and exertional desaturation of at least 4% on pulse oximetry during submaximal exertion (corridor walking). Patients with any other complicating medical condition were excluded.
All patients made a visit before entry into the study at which they completed two 6 minute walks. This was to confirm that desaturation occurred on exercise, to familiarise the patients with the procedure, and to eliminate learning effects which have been observed to improve performance on the initial two walks.15 Patients were also familiarised with the use of a visual analogue scale (VAS) for measurement of breathlessness severity. Six patients failed one or more entry criteria and two dropped out during the study because of chest infections. Thirty four patients completed the study of oxygen pre-breathing and 18 completed the study of oxygen during recovery (performed at only one of the two participating centres).
The study was approved by the local ethics committees and all subjects gave written informed consent.
Gas delivery and walk tests
Two studies were undertaken, each using a double blind and randomised protocol. For each study patients performed duplicate 6 minute walk tests on a pre-measured course. The tests were performed at least 30 minutes apart to allow full recovery between exercise bouts.13 During the walks standard phrases of encouragement were delivered at 1 minute intervals.15 Those patients who took part in both studies did so on separate days.
Study 1: Oxygen pre-breathing
Patients breathed either air or oxygen for 10 minutes immediately before each walking test. Gas delivery was randomised and neither the patient nor the test supervisor was aware of the gas mixture being used, or of oxygen saturation levels which were recorded by another observer. The gas was supplied via constant performance masks (Intersurgical 010, Wokingham, UK, or Ventimask Mark IV) which supply 28% oxygen at the mouth over a wide range of flow rates and breathing patterns.16 A flow rate of 4 l/min was used.
Study 2: Oxygen during recovery
Patients breathed either air or oxygen for 5 minutes immediately after the walk. The double blind mode of gas delivery, randomisation, and recording were as for the first study.
Measurements
In addition to the distance walked, oxygen saturation and heart rate were measured continuously during each test by a portable pulse oximeter (Ohmeda 3775 or Minolta Pulsox-7) carried by the test operator. Subjective breathlessness was measured on a 100 mm visual analogue scale (VAS) with end points of “not breathless at all” and “the most breathless I have ever been”. The VAS score was recorded at rest before exercise, at the end of the walking test, and at the point of objective recovery (pre-breathing study) or at the end of 5 minutes of air or oxygen breathing (recovery study). Time to subjective recovery from breathlessness was recorded by asking patients to inform the test operator when they felt back to the level of breathlessness they had noted at baseline, before exercise and gas administration. Objective recovery time was measured as the time at which oxygen saturation had returned to within 2%, and heart rate to within 5 beats/min of the pre-exercise baseline values.
Statistics
The study was originally devised to provide 90% power to detect a 20% change in walk distance or VAS score, requiring that 26 patients complete the protocol.
Relationships between variables were assessed by correlation analysis and possible differences by two tailed paired or unpaired t tests and by examination of 95% confidence intervals. Statistical significance was taken at the 95% level. Data were analysed using SPSS.
RESULTS
The characteristics of the 34 patients (18 men) who completed the pre-breathing study and the subset of the 18 (10 men) who completed the recovery study are given in table 1. The majority had severe COPD; in all but four the FEV1 was less than 50% of the predicted value, and 74% were desaturated (Sao2 <96%) at rest. The subset of patients who completed the recovery study did not differ significantly in any respect except FEV1 as a percentage of the predicted value was marginally lower.
Clinical details of patients in study 1 (pre-breathing oxygen) and study 2 (oxygen during recovery)
Oxygen pre-breathing
The effect of pre-breathing 28% oxygen on arterial oxygen saturation is shown in fig 1. There was a mean rise of 3.0% at the end of the oxygenation period, before exercise, compared with air breathing (95.3% after oxygen, 92.3% after air, p<0.01). This difference had disappeared by the end of the 6 minute walk (84.3% after oxygen, 82.9% after air, p=NS).

Mean arterial oxygen saturation at rest on room air (baseline), following gas breathing (pre-exercise), and at the end of the 6 minute walk (post-exercise). *p<0.01 for air v oxygen breathing.
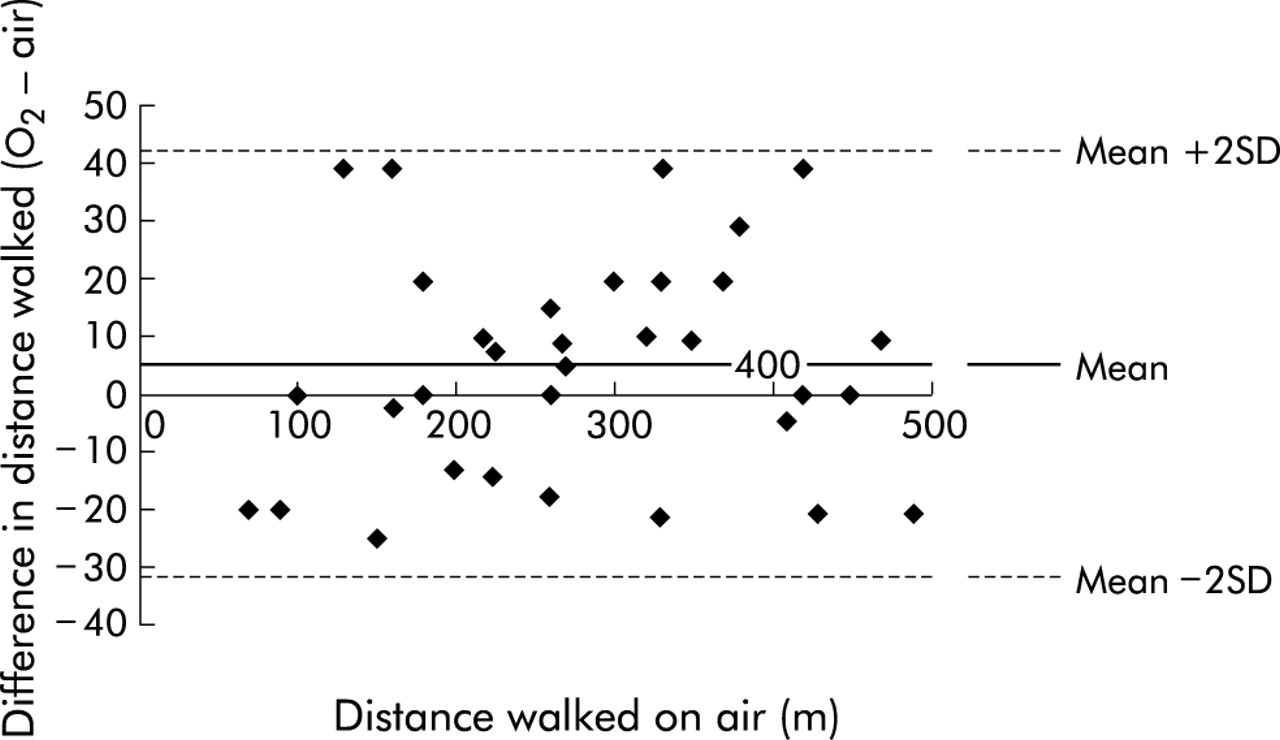
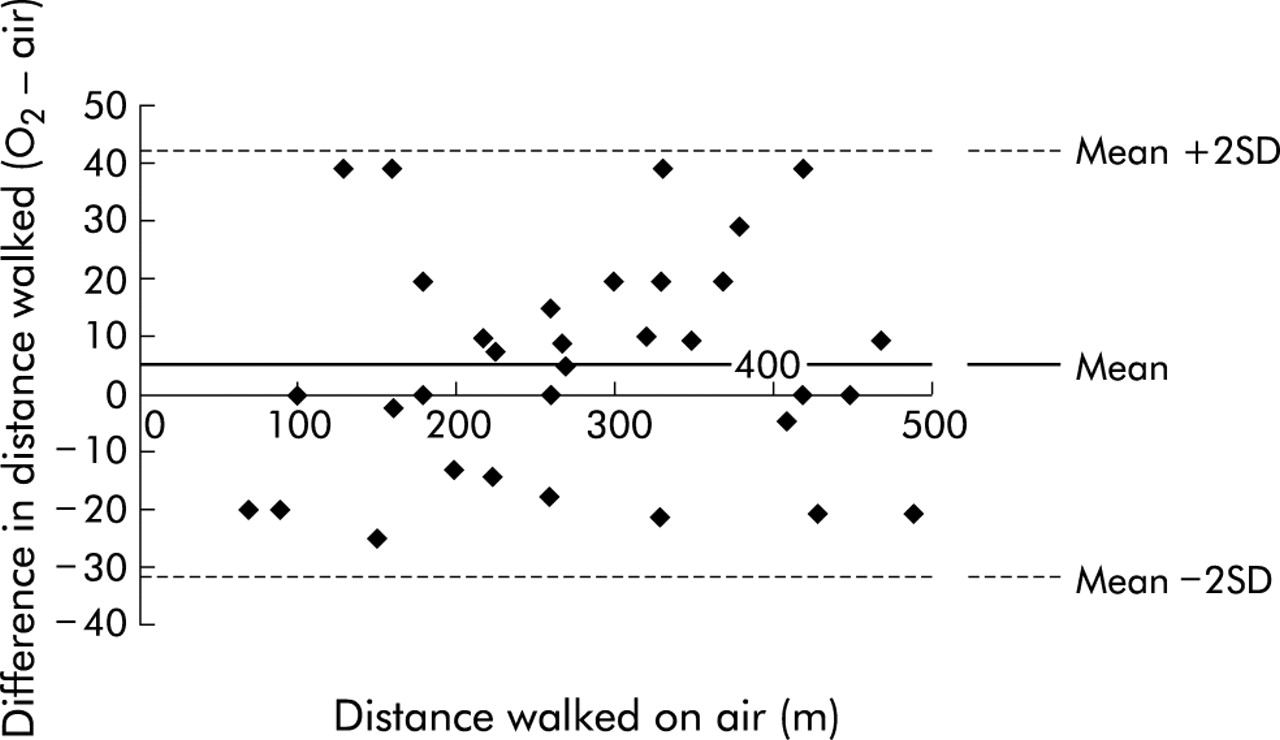
The effect on exercise measurements is shown in table 2. There was a small, statistically non-significant mean increase in 6 minute walk distance. There was no change in subjective breathlessness or in recovery times. Figure 2 presents a comparison of the 6 minute walk distance on air and oxygen for individual patients.
Effects of pre-breathing oxygen and air on 6 minute walk distance, oxygen saturation, breathlessness, and recovery time in 34 patients with COPD
{kind=link}
{kind=link}
Individual data on walk distance after pre-breathing air and oxygen (Bland-Altman plot format). The small increase in mean distance after oxygen was not significant.
Correlation analysis of the data for air breathing confirmed the existence of expected weak relationships between oxygen desaturation, breathlessness, and exercise intolerance. Thus, the more breathless subjects walked less distance (r=–0.47, p<0.01), as did those who desaturated further (r=–0.36, p<0.05). There was also a positive correlation between fall in arterial saturation and severity of breathlessness (r=0.40, p<0.05).
Oxygen during recovery
The two walks performed by each subject in this study were comparable; there was no significant difference between the mean distances walked (246 v 247 m), degree of breathlessness (VAS 70 v 74 mm), or arterial oxygen saturation at the end of the walks (81.7% v 80.4%). Relevant results during recovery are shown in table 3; oxygen breathing did not improve breathlessness or shorten recovery time. As expected, oxygen breathing raised arterial saturation but no other difference was detectable.
Effects of 5 minutes of oxygen or air breathing immediately after 6 minute walk
DISCUSSION
The outcomes of both parts of this study are clear. At rates available from domiciliary systems in the UK, neither pre-breathing oxygen before exercise nor breathing oxygen during recovery was effective in relieving dyspnoea or usefully increasing submaximal exercise tolerance in COPD patients with exercise limitation and desaturation on air.
Oxygen pre-breathing for a period of 10 minutes before exercise at 4 l/min (approximately 28% inspired oxygen concentration) has been shown in previous studies to raise arterial oxygen saturation to a plateau level 2–8% higher than baseline.2,4,10,11 Our patients showed similar increases.
There are few comparable previous studies. Woodcock and colleagues4 found a 10% improvement in 6 minute walk distance (which increased by 28 m) but no improvement in dyspnoea in 10 “pink puffers” after oxygen pre-breathing. Rhind et al10 reported on a group of 12 hypoxic patients in whom they found no improvement in walk distance, and two other studies (treadmill exercise in 20 patients11 and stair climbing in 18 patients12) also reported no improvement in exercise tolerance or breathlessness scores after oxygen.
Our patients did not walk significantly further after oxygen or notice any relief of breathlessness. Only four patients walked more than 30 m further after oxygen. In addition to the fact that the mean difference between the air and oxygen walk distances did not differ significantly from zero, there are a number of reasons why the result in these patients is likely to be due to limited reproducibility of the method rather than a real difference. Firstly, one of these patients walked further without oxygen pre-breathing in two subsequent walks undertaken for the recovery study. Secondly, another “responder” who repeated the test at a later date walked marginally further after air than after oxygen pre-breathing on that occasion. Finally, a third “responder” had walked further on his screening walk, without pre-breathing oxygen, than he did during the formal test walks.
None of the clinical or physiological characteristics of the patients separated the apparent responders to oxygen from the rest. This included an examination of the “store” of extra oxygen provided by pre-breathing oxygen. The extra oxygen stored in the blood can be calculated from the measured saturations, assuming a blood volume of 5 litres. The approximate extra volume of oxygen in the lung can be calculated by first deriving alveolar oxygen concentrations from the values of arterial saturation (with the assumption of a normal oxyhaemoglobin dissociation curve). The volumes of oxygen in the lung after breathing the two gases can then be derived by multiplying these concentrations by total lung capacity (with the further assumption of complete mixing in the lung, which is tenable given the pre-breathing period used17). In the 23 patients in whom total lung capacity measured by helium dilution was available (3.6–7.3 litres), the total extra oxygen store after pre-breathing oxygen was 40–370 ml. This was not correlated with improvement in walk distance following oxygen pre-breathing.
The disappointing outcome of these studies is that pre-breathing oxygen does not reduce breathlessness in COPD and, in hypoxic patients at least (who might be expected to derive most benefit), does not improve performance either. Factors other than oxygen saturation are clearly more important determinants of walk distance. These might include, for example, respiratory work, peripheral muscle fatigue, or cardiovascular deconditioning. Desaturation would then represent a marker of severity of disease rather than a primary factor limiting exercise tolerance. The wide scatter in walk distances between patients (table 1 and fig 2) would be consistent with this concept.
The 6 minute walk test has been widely used in previous studies of dyspnoea and exercise tolerance in COPD, and has shown that oxygen supplementation during exercise can cause improvement.3–7 The test has the advantages that it is comparable to real life exertion and has been validated for the detection of therapeutic improvements in dyspnoea in COPD.18 It is also safe, inexpensive, and simple to set up. Given that oxygen saturations had returned to baseline by the end of the 6 minute walk in our patients, it is possible that a shorter exercise period would have yielded a more positive outcome. However, no such effect on breathlessness was seen by McKeon et al11 who examined VAS scores at 1 minute intervals during exercise after oxygen pre-breathing and found no detectable early benefit. Walk tests shorter than 6 minutes, and other forms of exercise such as stair climbing, are less reproducible than the 6 minute walk test and, in any case, an intervention which helps the patient for much less than 6 minutes would be of little value.
Oxygen breathing during recovery from exertion is the commonest way in which patients use domiciliary oxygen supplied by cylinder8 and has been examined previously in two studies. Evans et al13 used step testing and showed a very modest reduction in subjective recovery time in 11 of 19 patients; however, they were using higher inspired oxygen concentrations (67%) than can be achieved with domiciliary systems. In part of a larger study Killen and Corris12 used oxygen at low flow rates (2 l/min) after brief stair climbs and reported a non-significant reduction in peak dyspnoea assessed by VAS. In the present study we found no evidence that recovery time from exercise is shortened, or dyspnoea alleviated, by oxygen from cylinder based systems of the kind used for domiciliary treatment in the UK.
In summary, our studies do not support a useful therapeutic role for domiciliary oxygen by cylinder in patients with COPD who desaturate on exercise, whether it is used before or after exercise. We suggest that current prescribing practice for this treatment in the UK (short burst use for the alleviation of dyspnoea in COPD patients) should be revised. If the evidence from this and previous studies is to be followed, only patients with a demonstrable objective benefit should be considered suitable for such treatment. They are likely to be a small minority. We should add the caveat that this study did not allow us to examine the possibility of a benefit from a flow of cold gas on the face,19 although we are able to assert that this need not be oxygen.
REFERENCES
Footnotes
-
↵* Dr MacRae died during the final preparation of the manuscript.