Article Text

Abstract
Background: A study was undertaken to investigate the differential diagnostic role of chest radiographic findings, total white blood cell count (WBC), erythrocyte sedimentation rate (ESR), and serum C reactive protein (CRP) in children with community acquired pneumonia of varying aetiology.
Methods: The study population consisted of 254 consecutive children admitted to hospital with community acquired pneumonia diagnosed between 1993 and 1995. WBC, ESR, and CRP levels were determined on admission. Seventeen infective agents (10 viruses and seven bacteria) were searched for. Chest radiographs were retrospectively and separately reviewed by three paediatric radiologists.
Results: A potential causative agent was found in 215 (85%) of the 254 cases. Bacterial infection was found in 71% of 137 children with alveolar infiltrates on the chest radiograph, while 72% of the 134 cases with a bacterial pneumonia had alveolar infiltrates. Half of the 77 children with solely interstitial infiltrates on the chest radiograph had evidence of bacterial infection. The proportion of patients with increased WBC or ESR did not differ between bacterial and viral pneumonias, but differences in the CRP levels of >40 mg/l, >80 mg/l, and >120 mg/l were significant although the sensitivity for detecting bacterial pneumonia was too low for use in clinical practice.
Conclusions: Most children with alveolar pneumonia, especially those with lobar infiltrates, have laboratory evidence of a bacterial infection. Interstitial infiltrates are seen in both viral and bacterial pneumonias.
- bacterial pneumonia
- viral pneumonia
- community acquired pneumonia
- children
Statistics from Altmetric.com
Childhood community acquired pneumonia is a common illness. Several bacteria and viruses and their combinations can cause the infection, but there is a lack of rapid and commercially available laboratory tests for most pathogens which may explain why the aetiology is rarely established in clinical practice and why antibiotic treatment is empirical in most cases. Up to 60% of the cases are associated with respiratory virus infections, so unnecessary and ineffective antibiotic treatment may often be used.1
Many published studies have addressed the differentiation of bacterial from viral pneumonia using clinical,2–5 radiological,2–9 and routine haematological tests,2–5,9–11 but these methods have not been found to be sufficiently reliable in differential diagnosis. These studies have been hampered by incomplete aetiological approaches. Some studies have looked only for a limited number of microbes,2–5,7,12 some have used insensitive techniques,2,4,13 and some have used only serological tests14 or bacterial antigen tests.13 It is therefore not well established whether bacterial and viral pneumonia can be differentiated by routine radiological and laboratory tests.
This 3 year study was undertaken to investigate the chest radiographic changes in childhood community acquired pneumonia of many different aetiologies. In addition, the differential diagnostic roles of the total white blood cell count (WBC), erythrocyte sedimentation rate (ESR), and serum C reactive protein (CRP) levels were studied. To obtain the maximum yield of microbiological diagnoses we collaborated with several research laboratories and searched for 17 infective agents using many different laboratory methods.
METHODS
Between 1 January 1993 and 31 December 1995, 296 consecutive children admitted to hospital with community acquired pneumonia were enrolled in the study. The diagnosis was based on a simultaneous finding of an infiltrate on the chest radiograph and fever (>37.5°C) and/or respiratory symptoms. The radiological diagnosis was made either by a paediatric radiologist (during office hours) or a resident on call. All patients were treated in the Department of Pediatrics of Turku University Hospital. Forty two children were excluded, either because a convalescent serum sample was not obtained (n=33) or because the chest radiographs were not available for review or because no infectious infiltrate was found on the radiograph on review (n=9). The remaining 254 patients were entered in the study (37 aged <1 year, 71 aged 1–2 years, 84 aged 2–5 years, and 62 ≥5 years of age).
Posteroanterior and lateral chest radiographs were obtained on admission and were reviewed retrospectively and separately by three paediatric radiologists. The findings were classified as: alveolar and/or interstitial pneumonic changes, hyperaeration, hilar enlargement, atelectasis, pleural fluid, location in one lung or both lungs. Individual findings were accepted if at least two of the three radiologists agreed. The chest radiographs with alveolar infiltrates were re-reviewed by one of the radiologists (RV) to determine whether the infiltrate was lobar or multilobar. WBC (× 109/l), ESR (mm/h), and CRP (mg/l) were determined on admission using routine laboratory methods.
Several bacteriological and virological methods were used to determine the potential cause of the pneumonia, details of which have been published earlier.15 Virus culture in nasopharyngeal aspirates was performed using the Ohio strain of HeLa cells and human foreskin fibroblasts according to routine procedures. Viral antigens (influenza A and B viruses, respiratory syncytial virus, parainfluenza virus types 1, 2, and 3, and adenovirus) in nasopharyngeal aspirates were detected by time resolved fluoroimmunoassay using monoclonal antibodies.16 Virus specific serum antibody titres from acute and convalescent serum samples were determined by enzyme immunoassay (EIA) using antigen coated solid phase and horseradish peroxidase conjugated rabbit antihuman IgG (Dako A/S, Glostrup, Denmark).16 Human herpesvirus 6 (HHV-6) IgG responses were detected by microimmunofluorescence.17 The diagnosis of Epstein-Barr virus and varicella zoster virus infections was based on routine determination of IgM antibodies. Two reverse transcription PCR assays were used for detection of rhinoviruses.18,19
Bacterial antibody assays were performed on acute and convalescent serum samples. IgG antibodies to pneumococcal pneumolysin and C-polysaccharide (CPS) were measured by EIA.16 Circulating immune complexes containing pneumococcal CPS and pneumolysin were also measured from paired serum samples.20 Antibodies to non-typeable Haemophilus influenzae and Moraxella catarrhalis were detected by EIA using whole bacterial cell antigen.16 IgM antibodies to Mycoplasma pneumoniae were measured using a commercial EIA kit with minor modifications (Platelia; Sanofi Diagnostics Pasteur SA, Marnes la Coquette, France).21 IgG and IgM antibodies to chlamydial species were studied by a microimmunofluorescence method using elementary antibodies of Chlamydia pneumoniae Kajaani 7 and C trachomatis 1.2 as antigens.16 Anti-streptococcal antibodies (antistreptolysin 0 and antideoxyribonuclease B) were measured using routine commercial laboratory tests.
Statistical analyses
The standard χ2 test was used to compare the proportions between the groups.
RESULTS
Aetiology
A potential causative agent was found in 85% of the cases and this has been reported separately.15 A respiratory virus was found in 62% (RSV 29%, rhinovirus 24%, parainfluenza viruses 10%, adenovirus 7%, influenza viruses 4%, other viruses 8%) and a bacterial agent in 53% (Streptococcus pneumoniae 37%, Haemophilus influenzae 9%, Mycoplasma pneumoniae 7%, Moraxella catarrhalis 4%, Chlamydia pneumoniae 3%, other bacteria 2%). In 30% of cases there was evidence of a mixed viral/bacterial infection, viral infection alone was detected in 32% and bacterial infection alone in 22% of patients. The comparisons between bacterial infections (n=134, sole bacterial infections + mixed bacterial/viral infections) and sole viral infections (n=81) are shown in tables 1 and 2. There were no significant differences between bacterial infections alone and mixed bacterial/viral infections (statistical results not shown). Children aged ≥2 years had a bacterial pneumonia more often than children <2 years of age (72% v 51%, p=0.001).
Chest radiographic findings in 215 children with community acquired pneumonia
Laboratory findings and combinations of chest radiographic and laboratory findings in 215 children with community acquired pneumonia
Radiographic findings
Evidence of a bacterial infection was found in 71% of 137 children with alveolar infiltrates on the chest radiograph (64% of the 215 patients in the study), while 72% of the 134 cases with a bacterial pneumonia had alveolar infiltrates. In children with solely viral pneumonia 49% had alveolar changes (p=0.001 compared with bacterial pneumonias, table 1). The alveolar infiltrate was lobar in 36% of cases with bacterial pneumonia and in 15% of the those with viral pneumonia (p=0.001).
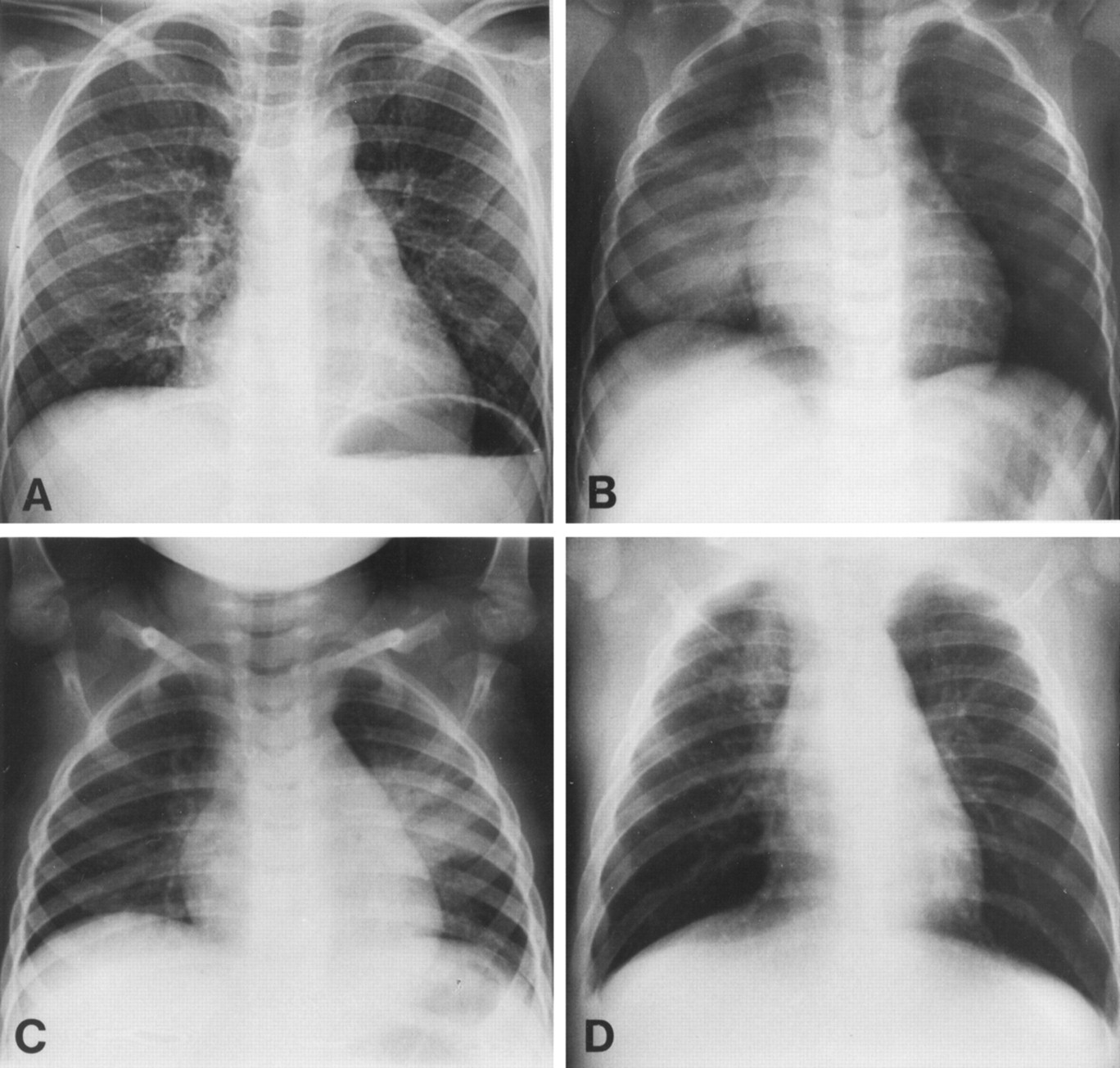
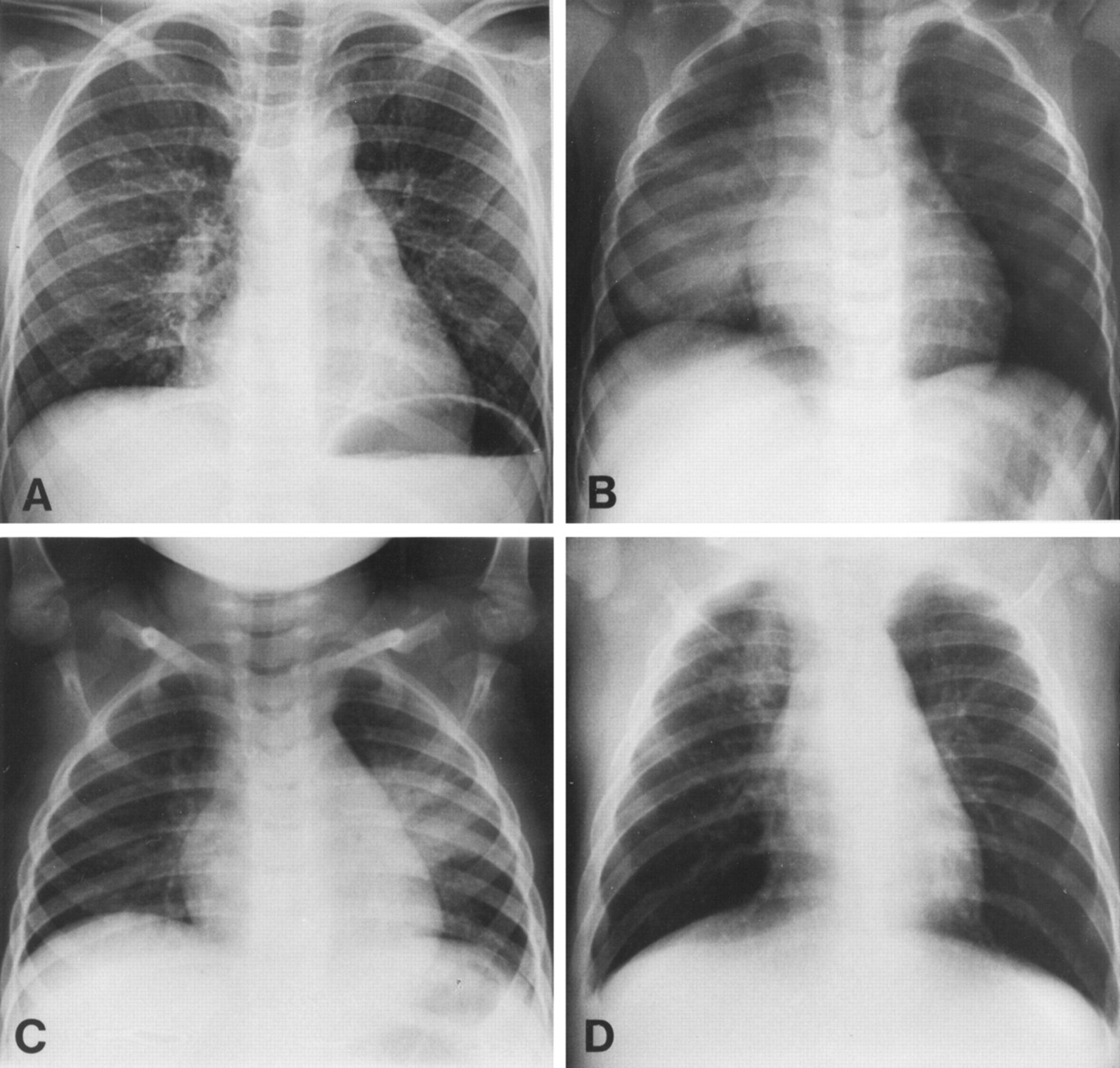
Half of the 77 children with sole interstitial infiltrates on the chest radiograph had evidence of viral infection and half had evidence of bacterial infection. The 215 patients were divided into two subgroups according to age (<2 years and ≥2 years). In children aged ≥2 years, 78% (n=65) of those with bacterial infection had alveolar infiltrates compared with 56% (n=18) of those with viral infection (p=0.02, table 1). Representative chest radiographs of four patients are shown in fig 1.
{kind=link}
Chest radiographs of (A) a 6.5 year old girl with widespread interstitial changes in both lungs caused by S pneumoniae (significant increase in pneumolysin IgG antibodies), WBC 29.8 × 109/l, ESR 35 mm/h, CRP 9 mg/l; (B) a 1.9 year old boy with alveolar changes in the right lower lobe caused by S pneumoniae (significant increase in pneumolysin IgG antibodies), WBC 13.8 × 109/l, ESR 125 mm/h, CRP 332 mg/l; (C) a 2.8 year old girl with alveolar changes in the left lower lobe associated with rhinovirus, WBC 17.7 × 109/l, ESR 64 mm/h, CRP 128 mg/l; (D) a 0.3 year old girl with alveolar changes in the right upper lobe associated with parainfluenza 2 and human herpes virus 6, WBC 17.0 × 109/l, ESR 8 mm/h, CRP 22 mg/l.
Laboratory findings
The proportion of patients with an increased WBC (>15.0 × 109/l) or increased ESR (>30 mm/h) was similar in bacterial and viral pneumonia (48% v 47% and 66% v 60%, respectively). The differences in the CRP levels between the two groups were significant at the selected levels of >40 mg/l (p=0.004), >80 mg/l (p=0.001), >120 mg/l (p=0.001), and >160 mg/l (p=0.01). We chose a CRP concentration of >80 mg/l as a screening limit for bacterial pneumonia (sensitivity 0.52, specificity 0.72) because there were too many false positives at the level of >40 mg/l (specificity 0.53) and too many false negatives at the level of >120 mg/l (sensitivity 0.36). When the patients were subdivided into the two age groups (<2 years and ≥2 years), a CRP concentration of >80 mg/l significantly predicted bacterial pneumonia only in the younger age group (p=0.003, table 2).
Combined radiographic and laboratory findings
All of the combinations which had significant differences between bacterial and viral pneumonias included a CRP concentration of >80 mg/l. WBC >15.0 × 109/l or ESR >30 mm/h had no additional power. An additional 40 combinations were investigated but showed no significant results (data not shown).
DISCUSSION
Our observations show that most children with an alveolar pneumonia, especially those with lobar infiltrates, have laboratory evidence of a bacterial infection. This finding confirms the common belief that has not previously been based on rigorous data. The observation is clinically important because two thirds of the 254 hospitalised patients in our study had alveolar infiltrates on the chest radiograph. Half of the children with interstitial infiltrates as the sole radiographic finding had bacterial infection. This supports the view that interstitial infiltrates are not a reliable indication of solely viral pneumonia, although there were significantly more pneumonias with interstitial infiltrates in this group. WBC, ESR, and CRP—all of which may be available to a clinician when deciding on treatment—added very little to the differential diagnosis. A serum CRP concentration of >80 mg/l was found to be the most practical laboratory test for bacterial pneumonia with a good specificity (0.72) but a low sensitivity (0.52).
The strength of this study is that several laboratory methods were used to identify all major viruses and bacteria associated with community acquired pneumonia in children and the potential causative agent was detected in 85% of cases. This is a much higher percentage than has been obtained in earlier studies of the role of chest radiography in the differential diagnosis of childhood pneumonias.2–7,9,12 Furthermore, our prospective study lasted 3 years and covered outbreaks of many different respiratory viruses which cause childhood pneumonia including S pneumoniae, RSV, and rhinovirus. Three experienced paediatric radiologists who were unaware of the possible aetiology read the chest radiographs independently without clinical information.
Several studies have suggested that bacterial pneumonia cannot be differentiated from non-bacterial pneumonia on the basis of the chest radiograph. In the study by McCarthy and co-workers on 128 ambulatory children with pneumonia, three observers interpreted a lobular or segmental consolidation in only three of the five children with bacterial pneumonia, and diffuse nodular densities or a disseminated reticular pattern in three of the 16 children with viral pneumonia.7 Turner et al studied the chest radiographs of 37 paediatric outpatients with pneumonia and documented viral or bacterial infection. Alveolar infiltrates were found in 38% of the cases with bacterial pneumonia and in 67% of those with viral pneumonia.2 Isaacs4 found viral pneumonia in 20 of 57 hospitalised children and bacterial pneumonia in four; lobar consolidation was seen in seven and two children, respectively. Courtoy and colleagues found alveolar infiltrates in 67% of 24 viral pneumonias and 42% of 12 bacterial pneumonias, the rest having interstitial infiltrates.5 Korppi and co-workers studied radiological findings in 61 children with microbiologically verified pneumonia. Alveolar pneumonia was associated with bacterial infection in 74% and with sole viral infection in 26% of the cases.9 Interestingly, Toikka and colleagues recently reported interstitial infiltrates (with no other radiological findings) in 9% of 85 children with blood culture positive pneumococcal pneumonia.22 The limited number of microbiological techniques used and the limited number of patients included undermine all of these findings. Furthermore, a reliable comparison of these studies is difficult because the descriptive terms of the radiological findings vary widely and no generalised conclusions can be drawn.
Our findings must be viewed with some reservations. We analysed chest radiographs and laboratory findings only once, on admission. Two or more observations during the illness might have given different results. Although we used several microbiological techniques, it is possible that more infectious agents, especially bacteria, could have been detected if polymerase chain reaction methods had been used more widely.23
In conclusion, our study provides evidence that bacterial infection is highly probable in cases of childhood community acquired pneumonia with alveolar infiltrates on the chest radiograph. Interstitial infiltrates are seen in both viral and bacterial pneumonias. With the exception of serum CRP levels, routine haematological tests have very little practical value in addition to a chest radiograph. It is evident that all children with radiologically confirmed pneumonia should be treated with antibiotics because, in clinical practice, it is virtually impossible to distinguish exclusively between viral pneumonia and bacterial pneumonia.
Acknowledgments
The authors thank Peter B Dean for reviewing the manuscript.
REFERENCES
Footnotes
-
Supported by the Academy of Finland, the Pediatric Research Foundation, and the Finnish Radiological Society.