Article Text

Abstract
Introduction Lung function abnormalities are common in sickle cell anaemia (SCA) but data from sub-Saharan Africa are limited. We hypothesised that children with SCA from West Africa had worse lung function than their counterparts from Europe.
Methods This prospective cross-sectional study evaluated spirometry and anthropometry in black African individuals with SCA (haemoglobin phenotype SS) aged 6–18 years from Nigeria and the UK, when clinically stable. Age-matched controls were also included in Nigeria to validate the Global Lung Initiative spirometry reference values.
Results Nigerian SCA patients (n=154) had significant reductions in both FEV1 and FVC of ~1 z-score compared with local controls (n=364) and ~0.5 z-scores compared with the UK patients (n=101). Wasting (body mass index z-score<−2) had a prevalence of 27% in Nigerian patients and 7% in the UK ones (p<0.001). Among children with SCA, being resident in Nigeria (OR 2.4, 95% CI 1.1 to 4.9), wasting (OR 2.3, 95% CI 1.1 to 5.0) and each additional year of age (OR 1.2, 95% CI 1.1 to 1.4) were independently associated with increased risk of restrictive spirometry (FVC z-score<−1.64+FEV1/FVC≥−1.64).
Conclusions This study showed that chronic respiratory impairment is more severe in children with SCA from West Africa than Europe. Our findings suggest the utility of implementing respiratory assessment in African children with SCA to early identify those with chronic lung injury, eligible for closer follow-up and more aggressive therapies.
- paediatric lung disaese
- clinical epidemiology
- respiratory measurement
Statistics from Altmetric.com
Key messages
What is the key question?
Lung function abnormalities are common in sickle cell anaemia (SCA) but it has never been investigated whether there are differences in the degree of respiratory impairment between children with this condition living in West Africa and Europe.
What is the bottom line?
Children with SCA from West Africa have worse spirometry outcomes and higher prevalence of a restrictive spirometry pattern compared with their counterparts from Europe.
Why read on?
This is the first study comparing lung function in children with SCA living in West Africa and Europe, and it shows important differences in the degree of respiratory impairment between the two populations, implying the need of implementing lung function assessment in patients with SCA in West Africa.
Introduction
Respiratory complications and lung function abnormalities are common in patients with sickle cell anaemia (SCA).1 However, there are limited data from sub-Saharan Africa, where over 200 000 children with this condition are born each year.2 Chronic respiratory impairment in SCA has a multifactorial pathogenesis and involves both parenchymal, airways and vascular abnormalities.1 Patients generally experience a decline of lung function with age,3–6 and a restrictive pattern may appear in childhood,3 becoming common in adulthood.7 However, among paediatric patients with SCA living in high-income countries (HICs), obstructive lung function is more frequent than restrictive.8–10 Spirometry results have a prognostic meaning in adults with SCA, as a low FEV1 is associated with earlier mortality.7 Regarding risk factors for abnormal lung function in paediatric SCA patients, some studies pointed out an association with a history of acute chest syndrome (ACS)3 11 12 but other did not,8–10 whereas the rate of pain crises seems to be unrelated to respiratory abnormalities.8 10 Malnutrition is associated with increased risk of restrictive spirometry pattern in children with SCA from Central Africa,13 while the body mass index (BMI) percentile was found to be an independent predictor of increase in FEV1 in patients from HICs.14
Although limited evidence is available, it seems that lung function abnormalities are highly prevalent in paediatric patients with SCA from sub-Saharan Africa,12 13 15 16 with restrictive spirometry being the most frequent pathological pattern.13 The burden of respiratory disease in children with SCA living in low-middle income countries (LMICs) and HICs has not been previously compared. This evaluation could be useful because, if substantial differences were found, respiratory care of SCA patients in the two settings should be tailored to the local epidemiology.
In this cross-sectional study, we investigated lung function, through spirometry, in black African paediatric patients with SCA from Nigeria and the UK. Age-matched healthy controls were also included in Nigeria. We hypothesised that SCA-related chronic lung disease was more severe in paediatric patients from West Africa than in their counterparts from Europe, resulting in lower spirometry z-scores and higher prevalence of restrictive spirometry in the former.
Methods
Parental consent from each participant was obtained before assessments.
Black African individuals with SCA (haemoglobin phenotype SS) aged 6–18 years were consecutively enrolled between March 2016 and September 2017 during a follow-up appointment in two SCA clinic either at the Evelina London Children’s Hospital, UK, or the Barau Dikko Teaching Hospital, Kaduna, Nigeria. Both the hospitals are considered tertiary care centres for SCA in their countries. The study groups included patients of different socioeconomic status (SES), mainly living in urban areas and grossly representative of children with SCA followed at tertiary care in their countries, who are the majority in the UK17 but a minority in Nigeria.18 In the UK, only black African patients who had lived steadily in the country for the last 5 years were included. A control group of age-matched children and adolescents was enrolled in four schools in Kaduna state, Nigeria (details in online supplementary data), to verify whether the Global Lung Initiative 2012 (GLI-2012) reference values for spirometry fitted that population. In the UK, healthy controls were not enrolled, since the GLI-2012 had been previously validated for children of black African origin.19
Supplemental material
Individuals who had respiratory symptoms or felt unwell on the test day and those who performed a low-quality spirometry20 21 were excluded. Patients who had experienced SCA-related acute events (eg, pain crises) in the last month were also excluded. Details on sample size calculation are provided in online supplementary data.
Questionnaires
Caregivers of patients with SCA were interviewed by one of the investigators regarding frequency of pain crises in the last 12 months (bone pain in the chest, extremities or other areas that required at least 24 hours of analgesic therapy). A history of asthma was identified according to parent’s report or evidence from medical record of physician-diagnosed asthma ever. Information on hydroxyurea therapy and previous ACS episodes (fever and/or respiratory symptoms, accompanied by a new pulmonary infiltrate on a chest X-ray22) was taken from medical records.
Environmental factors that could have an impact on respiratory health, such as SES, tobacco smoke exposure and the type of fuel most frequently used for cooking at home, were also investigated. SES was evaluated using a modified version of the Family Affluence Scale (FAS)23 (details in online supplementary data).
Assessments
Height and weight were measured according to a standardised protocol (details in online supplementary data). Z-scores for height (zHeight) and BMI (zBMI) were derived using published reference equation.24 25 Wasting was defined as zBMI<−2 (<2.5th percentile) and stunting as a zHeight<−2. An Easy on-PC ultrasonic flowmeter spirometer (ndd, Zurich, Switzerland) was used and 95% of spirometry tests were performed by the principal investigator. Quality control was performed according to European Respiratory Society standards adapted for children20 21 and over-reading was carried out by a blinded trained investigator. Spirometry z-scores for FEV1, FVC and FEV1/FVC were derived according to the GLI-2012 reference equations for African–Americans.26 A z-score indicates how many SDs a measurement differs from the predicted value. The lower limit of normal (LLN) for spirometry was established at −1.64 z-scores (5th percentile) of the reference population.27 Spirometry patterns were classified as normal (FVC and FEV1/FVC≥LLN), obstructive (FVC≥LLN and FEV1/FVC<LLN), restrictive (FVC<LLN and FEV1/FVC≥LLN) or mixed (FEV1/FVC and FVC<LLN).
Statistical analysis
Normality of distribution was assessed by the Shapiro-Wilk test. Group comparisons were performed using unpaired t-test, Wilcoxon rank-sum test, χ2 test or Fisher’s exact test as appropriate. Regression analyses were restricted to SCA patients. The association between being resident in Nigeria (vs the UK) and a restrictive spirometry pattern (vs ‘normal’) was evaluated through a multivariable logistic regression model including several potential confounders (ie, sex, age, zBMI<−2, absence of hydroxyurea therapy, previous ACS and at least three pain crises in the last year). The same covariates (except for zBMI that was here considered as a continuous variable) were also tested in multivariable linear regression models for FEV1 and FVC z-scores. Covariates selection was carried out through a stepwise backward approach, by retaining in the final model variables with a p value<0.2 (saturated models are presented in online supplementary data). Validity of regression assumptions and the models’ fit were assessed through the analysis of residuals, the Cameron and Trivedi’s decomposition of information matrix test and the Hosmer-Lemeshow goodness-of-fit test. A p value<0.05 was considered as statistically significant. All analyses were conducted using Stata V.14 software.
Results
General characteristics of the study population
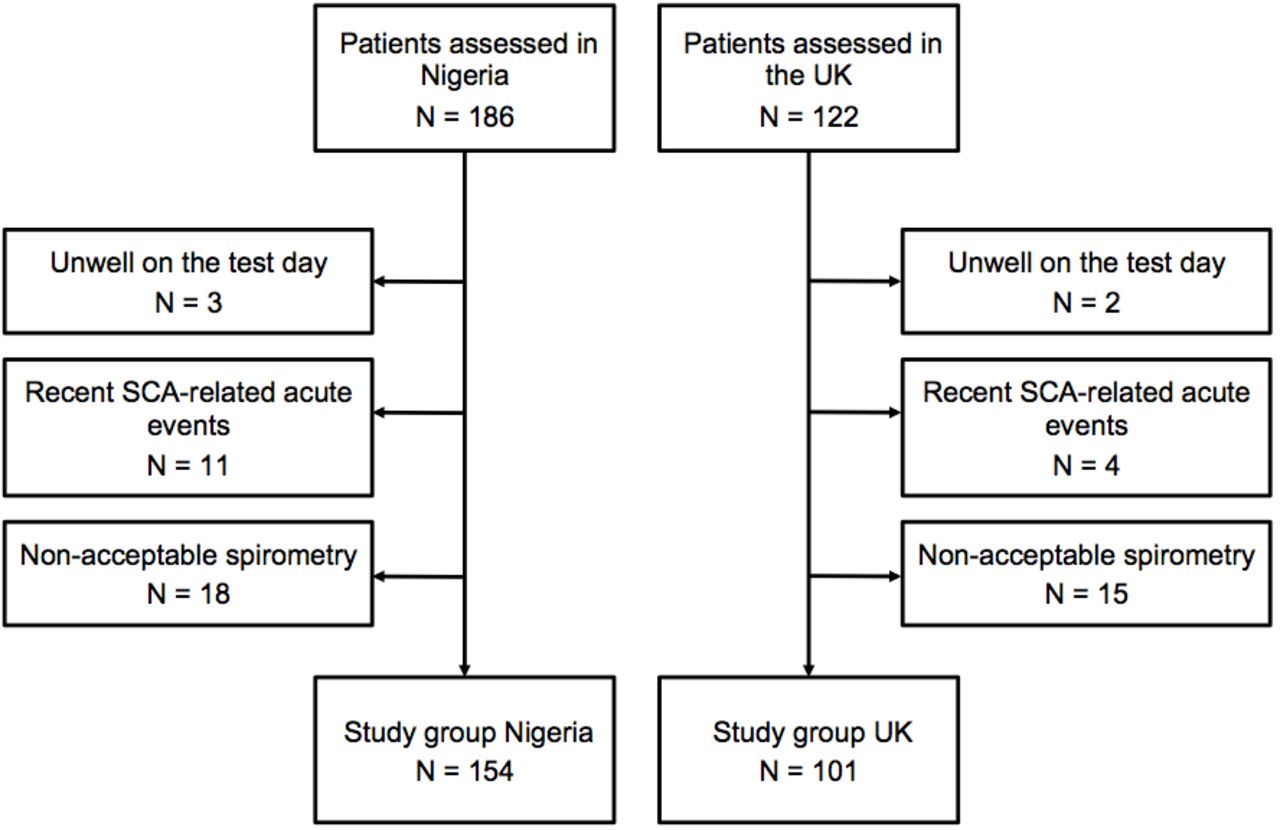
A total of 186 individuals with SCA in Nigeria and 122 in the UK were recruited. After exclusions (figure 1), data from 154 patients in Nigeria and 101 in the UK were analysed. Among patients enrolled in the UK, 82% (83/101) had West African origins (born in the UK or overseas), while the others were originally from different countries of Central and East Africa. Clinical characteristics of SCA patients are resumed in table 1.
Frequency of clinical variables in paediatrics patients (aged 6–18 years) with sickle cell anaemia (SCA) from the UK (n=101) and Nigeria (NIG) (n=154)

Study groups. Patients with sickle cell anaemia (SCA) aged 6–18 years from two tertiary care centres in Nigeria and the UK.
Distribution by age and sex was similar in the two groups of SCA patients (see online supplementary table E1). Among controls, 15/434 (3%) were excluded for the presence of respiratory symptoms and 55/434 (13%) for low-quality spirometry, with 364 individuals left in the final analysis (table 2).
Anthropometric and spirometry z-scores in patients aged 6–18 years with sickle cell anaemia (SCA) from the UK and Nigeria (NIG)
Frequency of low SES (FAS score 0–1 out of 6) in Nigeria was 52% in SCA patients, 52% in controls, and 17% among patients with SCA in the UK (p<0.001 compared with Nigerian SCA group) (see online supplementary table E2). Passive smoking was recorded in 9% of SCA patients in Nigeria and 12% in the UK (p=0.4). Almost half (49%) of Nigerian patients used solid fuels for cooking (37% wood, 10% coal and 1% animal dung), whereas the other patients in Nigeria and in the UK used non-solid fuels (see online supplementary table E2).
Lung function and nutritional status in SCA patients and controls
Children and adolescents with SCA in Nigeria had lower spirometry and markedly lower anthropometry z-scores than those from the UK (table 2). The proportion of patients with FEV1<5th percentile of predicted was 38% in Nigeria and 27% in the UK (p=0.05).
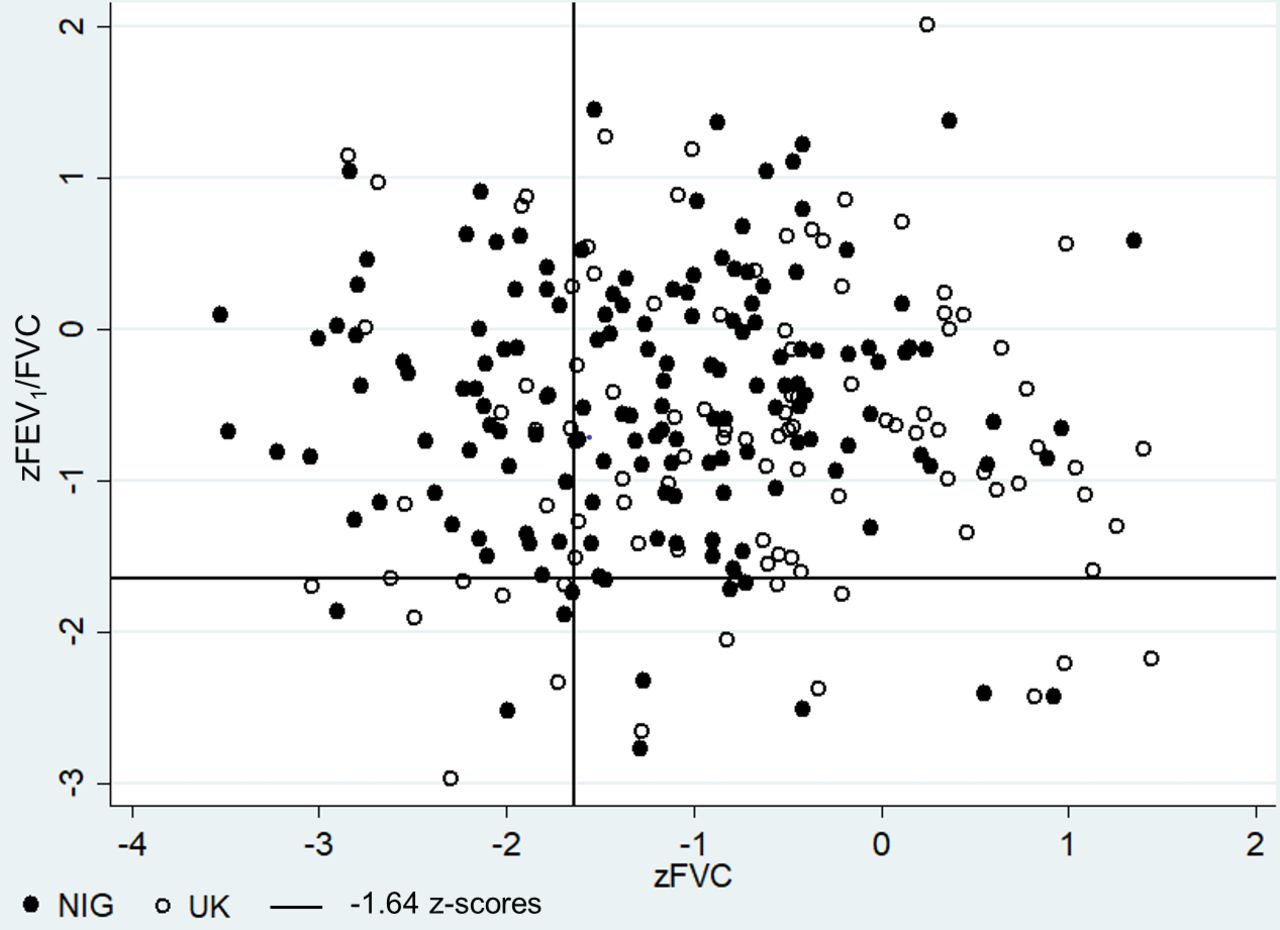
Most children and adolescents with SCA in both countries had normal spirometry (62% in Nigeria and 70% in the UK, p=0.19) (figure 2). Prevalence of a restrictive spirometry pattern was more than double in the Nigerian SCA group than in the UK one (30% vs 14%, p=0.008), whereas there were no significant differences in the frequency of an obstructive pattern (5% vs 9%, p=0.4) and a mixed obstructive/restrictive pattern (3% vs 7%, p=0.11).
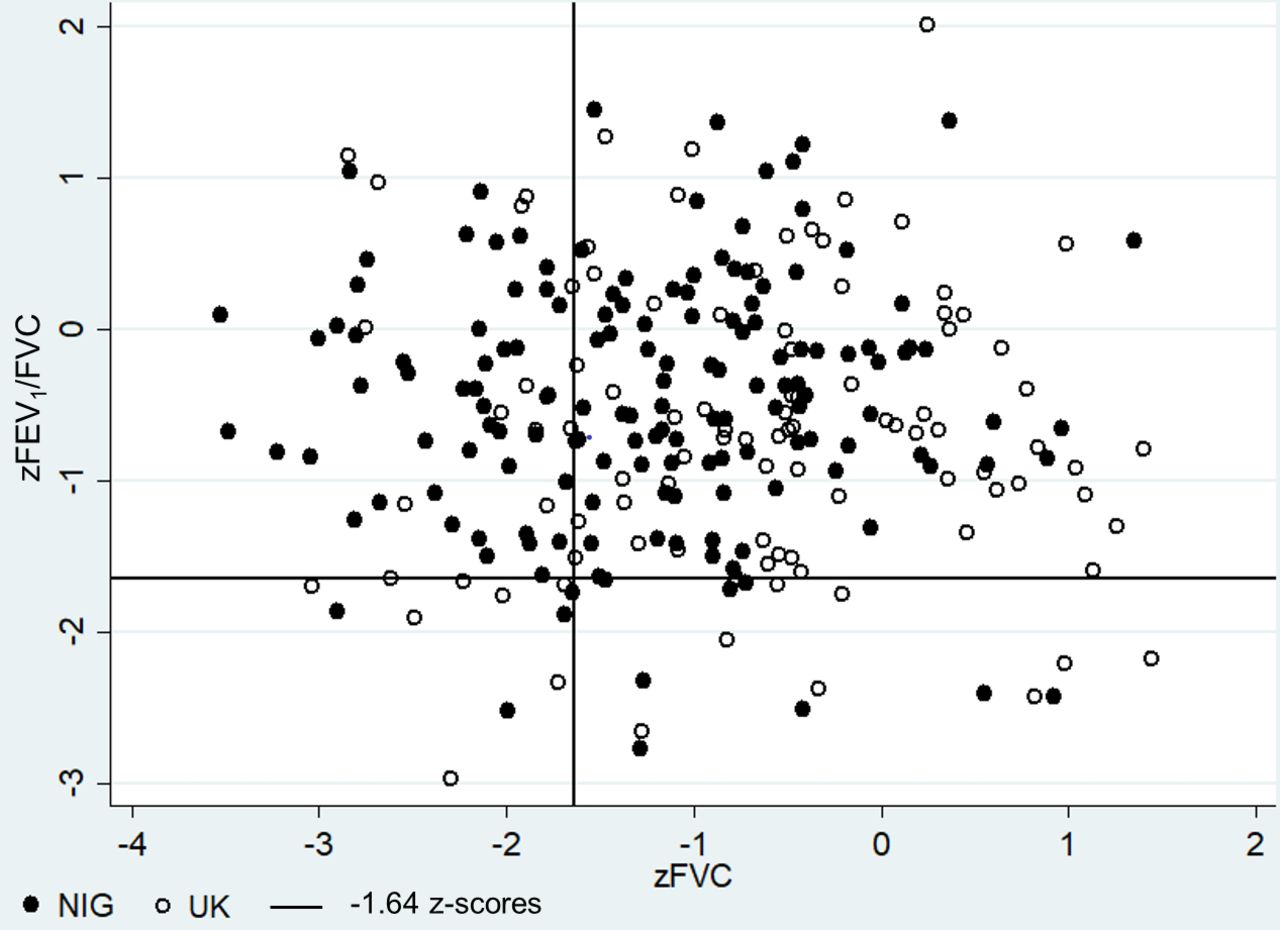
Scatter plot of FEV1/FVC versus FVC z-scores in children aged 6–18 years with sickle cell anaemia from Nigeria (NIG) (black dots, n=154) and the UK (white dots, n=101). The continuous lines represent −1.64 z-scores. Z-scores were derived from the Global Lung Function Initiative 2012 equations for African–Americans.26
Mean FEV1 and FVC values in Nigerian controls were within −0.3 z-scores from predicted with SD close to 1, while mean (SD) FEV1/FVC z-score was −0.08 (0.88) (table 2). Prevalence of pathological spirometry patterns in controls was 8% restrictive, 4% obstructive and 0.5% mixed.
Stunting had a prevalence of 41% in patients with SCA in Nigeria, 23% in local controls (p<0.001) and 5% in the UK SCA group (figure 3). Wasting was found in 27% of patients in Nigeria, 10% of controls (p<0.001) and 7% of the UK SCA group (figure 3).

{kind=link}
{kind=link}
{kind=link}
Prevalence of wasting (BMI z-score<−2), stunting (height z-score<−2) and the combination of both in patients with sickle cell anaemia (SCA) from the UK (n=101), Nigeria (n=154) and healthy controls in Nigeria (n=364), aged 6–18 years. Anthropometry z-scores are based on WHO growth charts. BMI, body mass index.25
Factors associated with lung function impairment in patients with SCA
At multivariable logistic regression in children with SCA, being resident in Nigeria (OR 2.4, 95% CI 1.1 to 4.9), each additional year of age (OR 1.2, 95% CI 1.1 to 1.4) and wasting (OR 2.3, 95% CI 1.1 to 5.0) were independently associated with increased risk of restrictive spirometry (adjusted R2=0.12) (table 3). Only these variables, along with a history of ACS, were retained in the final model, whereas the covariates ‘male sex’, ‘no hydroxyurea therapy’ and ‘at least three pain crises in the last 12 months’ were excluded according to a stepwise backward approach based on a p value<0.2.
Multivariable logistic regression for restrictive spirometry pattern (vs normal) in 223 paediatric patients with sickle cell anaemia from Nigeria and the UK
At multivariable linear regression analyses, increasing age, BMI z-score and a history of ACS also had a significant impact on both FEV1 z-score (adjusted R2=0.25) and FVC z-score(adjusted R2=0.27) of patients with SCA (table 4).
Multivariable linear regression models for FEV1 and FVC z-scores in 255 patients with sickle cell anaemia aged 6–18 years from Nigeria (n=154) and the UK (n=101)
There were no significant interactions among variables included in the logistic and linear regression models (data not shown).
There were no statistically significant differences in the prevalence of pathological spirometry patterns in Nigerian and the UK SCA patients according to SES, tobacco smoke exposure and, in Nigeria, the use of solid fuels versus non-solid fuels for cooking at home (data not shown).
Discussion
This study showed that black African paediatric patients with SCA living in a LMICs setting had significant reductions of approximately 0.5 z-scores in both FEV1 and FVC and a more frequent restrictive spirometry pattern compared with their counterparts resident in a HICs setting (30% vs 14%, p=0.008).
An obstructive pattern was more common among patients from the UK than Nigeria (9% vs 5%), though the difference was not significant (p=0.4). In studies performed in HICs, airflow limitation is a common finding at spirometry in children with SCA.8–10 Airway inflammation and remodelling related to vaso-occlusion and haemolysis in the pulmonary microcirculation,1 together with pulmonary vessel engorgement causing compression of the distal airways,28 could be the basis of this finding. Studies on adolescents and adults with SCA, however, show that a restrictive physiology becomes prominent with increasing age,7 29 30 probably as a consequence of cumulative lung injury. The predominance of a restrictive spirometry pattern over an obstructive one in children with SCA from Nigeria recalls the findings of older SCA patients in HICs7 and probably reflects a more advanced stage of chronic lung disease than in children with SCA from the UK.
Comparison of our findings with those of previous studies on children with SCA is hampered by the fact that many different spirometry reference values and criteria for defining lung function abnormalities have been used.4 9 10 15 16 Two recent studies adopting the GLI-2012 reference values reported frequencies of restrictive and obstructive spirometry patterns in children with SCA from HICs and LMICs settings, respectively, similar to those of the present study.8 13
Asthma was more frequent in the UK SCA group than in the Nigerian one. Asthma is reported in 15%–28% of people with SCA living in HICs,31 whereas we found that less than 10% of SCA patients in the Democratic Republic of Congo (Central Africa)13 and Nigeria (West Africa) had a physician’s diagnosis of asthma. Some of these children could have been underdiagnosed, due to poor healthcare access in sub-Saharan Africa.32 On the other side, though overdiagnosis of paediatric asthma is common in the primary care setting in HICs,33 that should not be the case for SCA patients enrolled in the UK, most of whom had been reviewed by a respiratory paediatrician and had an asthma diagnosis based on the integration of clinical history information and objective investigations. Overall, from our findings, it seems that asthma is less common in children with SCA from sub-Saharan Africa than in those from HICs. These differences could be related to a lower asthma prevalence in the general African population, which is estimated at 5.9% in the urban setting, although with high variability between countries.34
The GLI-2012 reference values fitted Nigerian children and adolescents adequately, as the mean spirometry z-scores in controls were within −0.3 z-scores from predicted with an SD of nearly 1.26 Paediatric SCA patients in Nigeria had marked reductions of 1.03 z-scores (13% of predicted) in FEV1 and 0.90 z-scores (11% of predicted) in FVC compared with local controls (table 2). Despite the use of different reference values precluding accurate comparison with other studies, low spirometry results have been consistently reported in African children with SCA from the eastern,15 central13 and western12 16 part of the continent. Conversely, most recent data from HICs, including our findings in the UK SCA group, show that patients living in this setting have higher dynamic lung volumes3 35 and narrower differences with controls3 36 compared with Nigerian patients. Overall, these findings suggest that chronic lung injury in children with SCA in HICs is milder than in sub-Saharan Africa. It is plausible that the disparities in healthcare provisions between the two settings play a role in these differences. In our study, for example, only one patient among those followed at a tertiary care centre in Nigeria had access to hydroxyurea therapy, which was shown to slow down lung function decline in paediatric SCA patients.37
Risk factors for pathological spirometry in patients with SCA
Being resident in Nigeria (vs the UK) was associated with a 2.4-fold increased risk of restrictive spirometry among SCA patients (95% CI 1.1 to 4.9). However, as most of UK patients had Nigerian origin, it is likely that the covariate ‘being resident in Nigeria’ was a proxy for other unmeasured risk factors, unrelated to genetic background. The above-mentioned differences in healthcare provisions between the UK and Nigeria might be among these risk factors, which should be further investigated in prospective studies.
Malnutrition, as indicated by the presence of wasting, affected almost one out of three Nigerian SCA patients (27%) and was much more frequent than in local controls (10%) and the UK patients (7%). There is evidence indicating that malnutrition is common in children with SCA in sub-Saharan Africa13 15 and is associated with worse clinical outcomes.38 From our findings, nutritional status seems to have an impact on lung function in SCA patients, as the unitary increase of zBMI was associated with approximately 0.3 z-scores increases in FEV1 and FVC, while wasting was associated with a more than doubled risk of restrictive spirometry (OR 2.3, 95% CI 1.1 to 5.0, p=0.03). The results are in line with those of previous studies reporting a positive association between BMI percentile and FEV1,14 as well as an increased risk of restrictive spirometry pattern in SCA patients with wasting.13 There are several factors potentially implicated in the relationship between nutritional status and lung function in SCA patients. First of all, wasting could reflect increased metabolic demands due to a more severe course of disease,38 including worse respiratory manifestations. Moreover, wasting could affect chest size39 and expiratory muscle strength, which was shown to be impaired in children with SCA.40
Increasing age was associated with a decline in spirometry z-scores and increased risk of restrictive spirometry. Although the cross-sectional nature of this study does not allow to draw conclusions regarding lung function changes over time, these findings are consistent with those of longitudinal studies showing a decline of lung function with age in paediatric SCA patients,3–5 associated with a progressively increasing risk of restrictive lung abnormalities.3 4
We found that a previous ACS episode had a negative impact on spirometry z-scores in children with SCA (table 4). However, since there is conflicting evidence from longitudinal studies,3 35 the relationship between ACS and respiratory impairment in SCA patients should be further investigated, especially in sub-Saharan Africa where it has not been evaluated so far.
The use of hydroxyurea was not associated with better lung function outcomes. However, this could be expected on a cross-sectional evaluation, considering that patients initiated on hydroxyurea generally are those with higher rates of complications and a more severe course of disease. There is already published evidence that hydroxyurea improves long-term lung function outcomes in SCA patients living in HICs,37 while evidence is pending in the African setting.
Tobacco smoke exposure and use of biomass fuel for cooking at home did not affect lung function in SCA patients. These factors have a detrimental effect on spirometry indices in the general paediatric population41 42 that might have been covered by SCA-related respiratory impairment in our study. It is even possible that methodological limitations (eg, environmental information based on parent’s report only; the impact of outdoor air pollution not evaluated; and the study not powered for this outcome) prevented to detect a possible impact of such environmental factors on lung function in children with SCA.
Strenghts and limitations
A strength of this study is that data collection was performed in two continents by the same principal investigator, using the same equipment and methodology. The validation of the GLI-2012 reference values for Nigerian children allowed a more accurate evaluation of spirometry results in patients with SCA from that country. The investigation of SES and sources of indoor pollution also allowed to evaluate the impact of important environmental factors on spirometry findings.
A limitation of this study is that the diagnosis of pathological respiratory patterns was only presumptive, in the absence of static lung volumes measurement. As known, cross-sectional studies usually cannot prove causality; therefore, especially for time-varying covariates, the associations found at regression analysis should be confirmed in longitudinal studies. The cross-sectional design also prevents from evaluating whether the lower spirometry results in patients with SCA from Nigeria are tracked over time and their prognostic meaning. Finally, since patients from Nigeria were followed at a tertiary care centre, they are not representative of the entire paediatric SCA population of that country, where most patients do not have access to tertiary care.18
Future directions
Future studies should focus on a longitudinal evaluation of lung function in SCA patients from sub-Saharan Africa, ideally including static lung volumes measured and accurate information about every aspect of clinical history that may influence respiratory outcomes. Another important area of research is the impact of comprehensive care programmes and therapeutic interventions, such as hydroxyurea, on long-term respiratory outcomes of SCA patients in low-resource settings.
Conclusions
Paediatric patients with SCA living in West Africa and followed at a tertiary care centre had more impaired lung function than their counterparts in the UK, showing significantly lower FEV1 and FVC z-scores and higher prevalence of a restrictive spirometry pattern. Wasting affected almost a third of Nigerian patients and was associated with lower dynamic lung volumes and increased risk of restrictive spirometry. In light of the high burden of respiratory impairment in children with SCA in West Africa, lung function assessment should be implemented in this setting to identify early patients with lung end-organ damage, who could benefit from closer follow-up and more aggressive therapies.
Acknowledgments
We thank Dr RC Audu, Dr Z Sani and Dr H Dadan-Garba from the Barau Dikko Teaching Hospital, Kaduna, Nigeria, for their help with data collection in Nigeria. We thank ‘SCORE International’ and ‘A.L.P.I. associazione allergie pneumopatie infantile’ for their financial support to the study.
References
Footnotes
Twitter @fizzy_emma, @ashelusher
Contributors MA conceived the study, performed data collection, interpreted data and wrote the manuscript; BI and PC conceived the study and contributed to the manuscript; MA, RZ, LGD, CZ, KV, EP, ADS and SN performed data collection and contributed to the manuscript; LC performed statistical analysis, interpreted data and contributed to the manuscript; ER, AG and MCC interpreted data and contributed to the manuscript. All the authors approved the final draft of the manuscript.
Funding ‘Sickle Cell Cohort Research Foundation’ (www.scorecharity.com) and ‘A.L.P.I. associazione allergie pneumopatie infantile’ (https://alpiassociazione.it/) offered financial support to refund travel expenses to Nigeria for two investigators (MA and CZ) and to buy a mobile spirometer that was used for data collection and was donated to the local hospital in Nigeria at the end of the study.
Competing interests None declared.
Patient consent for publication Obtained.
Ethics approval This cross-sectional multicentre study was conducted under approval by the local ethics committees in Nigeria (HREC 16-0017) and in the UK (REC 12/SW/0319).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on reasonable request.
Linked Articles
- Airwaves