Article Text

Abstract
Rationale: Birt–Hogg–Dubé (BHD) syndrome, a rare inherited autosomal genodermatosis first recognised in 1977, is characterised by fibrofolliculomas of the skin, an increased risk of renal tumours and multiple lung cysts with spontaneous pneumothorax. The BHD gene, a tumour suppressor gene located at chromosome 17p11.2, has recently been shown to be defective. Recent genetic studies revealed that clinical pictures of the disease may be variable and may not always present the full expression of the phenotypes.
Objectives: We hypothesised that mutations of the BHD gene are responsible for patients who have multiple lung cysts of which the underlying causes have not yet been elucidated.
Methods: We studied eight patients with lung cysts, without skin and renal disease; seven of these patients have a history of spontaneous pneumothorax and five have a family history of pneumothorax. The BHD gene was examined using PCR, denaturing high-performance liquid chromatography and direct sequencing.
Main results: We found that five of the eight patients had a BHD germline mutation. All mutations were unique and four of them were novel, including three different deletions or insertions detected in exons 6, 12 and 13, respectively and one splice acceptor site mutation in intron 5 resulting in an in-frame deletion of exon 6.
Conclusions: We found that germline mutations of the BHD gene are involved in some patients with multiple lung cysts and pneumothorax. Pulmonologists should be aware that BHD syndrome can occur as an isolated phenotype with pulmonary involvement.
- BHD, Birt–Hogg–Dubé
- DHPLC, denaturing high-performance liquid chromatography
- EBV-LCL, Epstein–Barr virus-transformed lymphoblastoid cell line
- FLCN, folliculin
- FNIP1, folliculin-interacting protein 1
- HRCT, high-resolution computed tomography
- LAM, lymphangioleiomyomatosis
- LCH, Langerhans cell histiocytosis
- tumor suppressor gene syndrome
- folliculin
- lymphangioleiomyomatosis
Statistics from Altmetric.com
- BHD, Birt–Hogg–Dubé
- DHPLC, denaturing high-performance liquid chromatography
- EBV-LCL, Epstein–Barr virus-transformed lymphoblastoid cell line
- FLCN, folliculin
- FNIP1, folliculin-interacting protein 1
- HRCT, high-resolution computed tomography
- LAM, lymphangioleiomyomatosis
- LCH, Langerhans cell histiocytosis
Birt–Hogg–Dubé (BHD) syndrome is a rare inherited autosomal genodermatosis first recognised in 1977 by three Canadian doctors.1 They studied a large family whose members were affected with multiple, small, white or skin-coloured papules on the face, neck and upper trunk that developed after the age of 25 years. These lesions, called fibrofolliculomas, are proliferating benign hamartomas of the hair follicle. Subsequent reports have described patients whose cutaneous lesions are associated with renal tumours,2–4 spontaneous pneumothorax or lung cysts,4,5 colon polyps and colon carcinomas.6,7,8,9,10,11
The genetic defect responsible for BHD syndrome was mapped to chromosome 17p11.22,12 and thereafter the BHD gene, consisting of 14 exons, was cloned.13 Disease-causing mutations were found over the entire region of the BHD gene, including insertions, deletions and nonsense mutations that were predicted to truncate the BHD protein.13 The BHD gene codes a protein called folliculin (FLCN)which is expressed widely in skin, kidney, lung and other organs.13,14 It is supposed to function as a tumour suppressor gene,15 and it has recently been reported that FLCN interacts with FLCN-interacting protein 1 (FNIP1) and may be involved in energy and/or nutrient sensing through the 5′ AMP-activated protein kinase and mammalian target of rapamycin signalling pathway.16
Once the BHD gene was identified, enabling genetic testing, the clinical features of BHD syndrome were gradually specified, giving a better understanding of the disease. Analysis of a large cohort of families with BHD syndrome revealed that the characteristic triad of the phenotype (involvement of skin, lung and kidney) may not always be apparent in people with BHD germline mutation and that BHD patients show diverse clinical heterogeneity.17 For example, it was reported that isolated familial spontaneous pneumothorax with no fibrofolliculomas and no renal tumour was caused by mutations of the BHD gene.18,19 Accordingly, we hypothesised that patients with multiple lung cysts with undetermined causes might be part of the clinical spectrum of BHD syndrome even if no skin and renal lesions exist.
In this study, we performed BHD mutation analysis in eight patients with multiple lung cysts identified by a chest CT scan that was prompted by the occurrence or history of pneumothorax or other predisposing reasons. Although all patients had neither skin nor renal lesions, five of the eight patients were found to carry BHD germline mutations.
MATERIALS AND METHODS
Study population
This study was approved by the ethics committees of Juntendo University. Written informed consent was obtained from all subjects as required. We enrolled a total of eight patients (two male, six female), who have been receiving medical care at our hospital since 1998 and had multiple lung cysts on high-resolution CT (HRCT) of the chest (table 1). High-resolution 2 mm sections were obtained through the chest at 10 mm intervals. We counted the number of cysts identified in all sections of the chest HRCT but regarded a cyst to be the same one when it was located in the same area in consecutive HRCT sections. All patients but one (patient B5) had a medical history of pneumothorax, and most of the patients had repeated episodes of pneumothorax in both lungs except for patients B4 and B8. Patient B4 had a pneumothorax but could not remember which side was affected, and patient B8 had experienced episodes of right-sided pneumothorax. Mean (SD) age at time of pneumothorax (except for patient B5) was 30.4 (10.9) years and age at time of enrolment was 41.8 (17.1) years. All patients but one (patient B4) had undergone video-assisted thoracic surgery for resection of the bullous part of the lungs, but this did not yield any pathological results that could identify causes for cystic formation in the lungs. Patient B8 underwent transbronchial lung biopsy, but did not result in definite diagnosis. There was thus no positive evidence, either clinical or pathological, to support the diagnosis of any cystic lung disease including lymphangioleiomyomatosis, pulmonary Langerhans cell histiocytosis (LCH), Sjögren syndrome, lymphoproliferative disorders, amyloidosis, alpha-1-antitrypsin deficiency, Ehlers–Danlos syndrome or Marfan syndrome. All patients were evaluated with abdominal CT scan and consulted dermatologists.
Clinical data of the eight subjects
Mutation analysis of the BHD gene
Genomic DNA was isolated from peripheral blood leukocytes. Exons with flanking intronic sequences of the BHD gene were amplified by PCR using genomic DNA. Each PCR was performed in a 25 μl reaction mixture containing 100 ng of genomic DNA, 1 μmol/l of each primer, PCR buffer II (Applied Biosystems, Foster City, California, USA), 1.0∼2.0 mmol/l MgCl2, 0.2 mmol/l dNTPs and 0.625 U of AmpliTaq Gold (Applied Biosystems). PCR primers were prepared according to the method of Nickerson et al.13 PCR conditions were 94°C for 4 min; 35 cycles of 94°C for 30 sec, 55°C for 30 sec, 72°C for 1 min; and 72°C for 5 min. Each PCR product was first screened for mutations by denaturing high-performance liquid chromatography (DHPLC) (WAVE; Transgenomic, Omaha, Nebraska, USA) and followed by sequence analysis if heteroduplex formation was detected. Although genomic sequencing may be more sensitive to detect mutations, we used DHPLC because it is sufficiently sensitive to screen for genetic alterations and commonly used for mutation analysis of hereditary diseases.20,21
Sequencing was performed using commercial reagents and an automated sequencer (ABI Prism BigDye Terminator v1.1 Cycle Sequencing Kit and ABI 3130 Genetic Analyzer; both Applied Biosystems). Both strands were sequenced to confirm nucleotide alterations. If direct sequencing revealed a superimposed nucleotide chromatogram suggesting nucleotide alteration of either insertion or deletion, the PCR products were cloned (TA Cloning Kit; Invitrogen, Carlsbad, California, USA) and then sequenced.
Reverse transcription PCR of BHD mRNA
An Epstein–Barr virus-transformed lymphoblastoid cell line (EBV-LCL) was established from peripheral blood mononuclear cells using standard methods and maintained in RPMI 1640 medium supplemented with 10% fetal calf serum. Total RNA was isolated from EBV-LCL (RNeasy Plus Mini Kit; Invitrogen) and cDNA synthesised by reverse transcriptase (RT) PCR (ThermoScript RT-PCR system; Invitrogen), under the same conditions as described above.
RESULTS
Germline mutation of the BHD gene
BHD mutations were identified in five patients (table 2). All mutations detected were unique and four of them were novel. All were insertions or deletions; no missense or nonsense mutations were found. Four different insertions or deletions (patients B1, B2, B3 and B7) cause frameshifts leading to premature truncation of the protein. The mutation identified in patient B2 was a cytosine insertion in the mononucleotide tract (hot spot) of eight cytosines (nucleotides 1733–1740, C8) in exon 11.13 Figure 1 shows a representative mutation analysis result and family pedigree of patient B1. The fifth mutation was a deletion including a splice acceptor site of intron 5 (patient B6; figure 2). As the mutation is expected to cause problems in BHD mRNA splicing, we examined the effect of the mutation on the mRNA transcript using EBV-LCL established from patient B6. RT-PCR demonstrated two different PCR products on agarose gel (figure 2C), one was the size expected from normally spliced transcript (453 bp) and the other expected from an exon 6-skipped transcript (231 bp): direct sequencing of the each PCR product confirmed that this assumption was correct (data not shown). However, a tiny amount of exon 6-skipped transcript appears to be generated in controls too, suggesting that the intron 5 splice acceptor site may be “leaky”, at least in EBV-LCL.
Results of mutation analysis of the BHD gene

Result of mutation analysis of the BHD gene in the family B1. (A) Family pedigree of patient B1. The proband’s brother had a history of pneumothorax. The proband’s maternal relatives have a family history of pneumothorax. Mutation analysis identified a GATG deletion in exon 13 (B) in the proband, her mother, brother and nephew, but not in her father and sister. We could not obtain consent for mutation analysis from the remaining family members. The paternal relatives had a family history of cancer, but it is unlikely to be related to BHD syndrome. (B) Sequencing of genomic DNA revealed superimposed nucleotide chromatograms near the end of exon 13 (upper panel). Cloning of the PCR products demonstrated clones carrying the wild-type sequence (middle panel) and those carrying a deletion of four nucleotides (GATG) (lower panel). The location of deletion is indicated by a rectangle in the wild-type sequence.
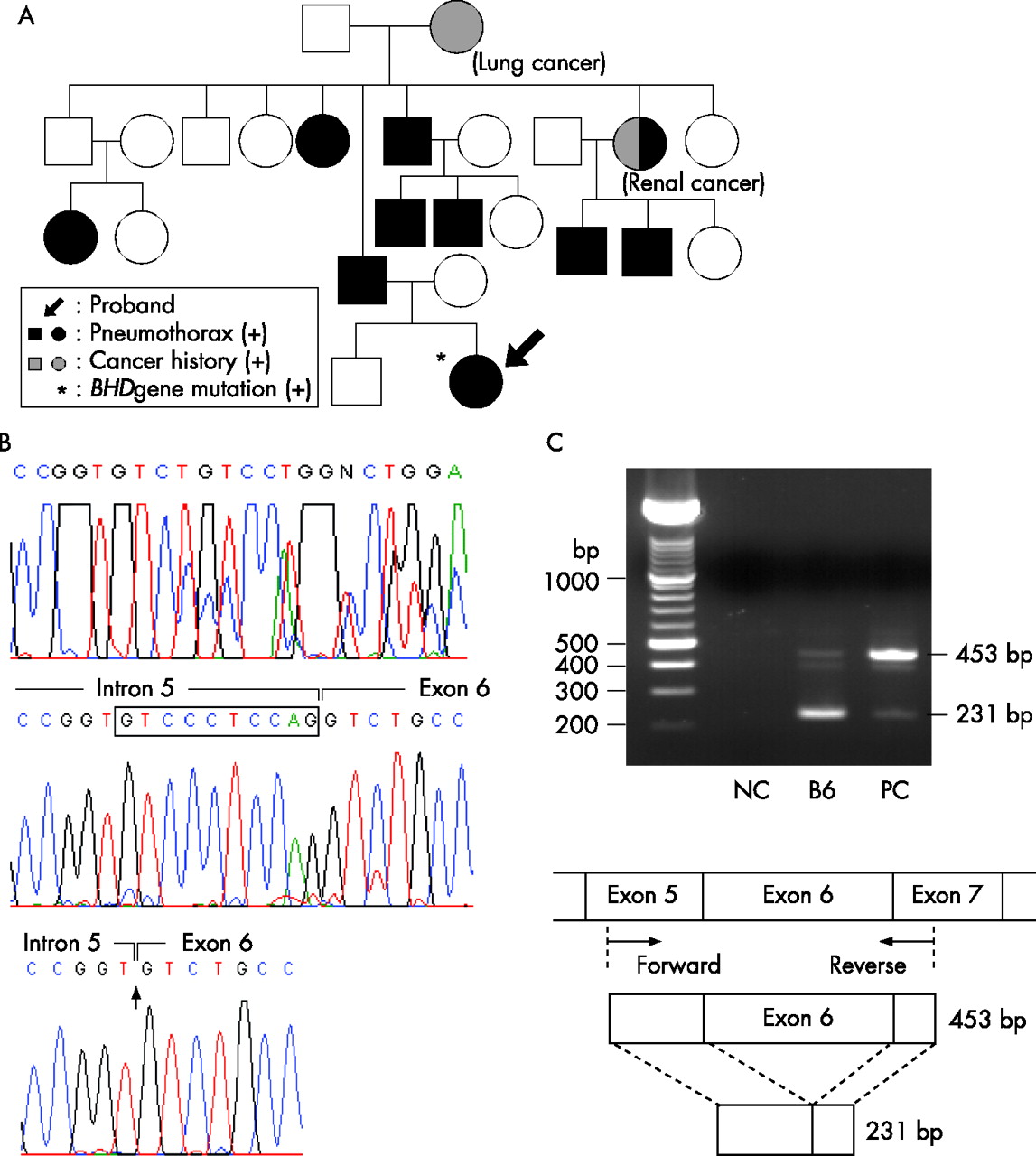
Result of mutation analysis of the BHD gene in the family B6. (A) The family pedigree of patient B6 shows a familial spontaneous pneumothorax in the proband’s paternal relatives. Note that the proband’s paternal aunt had a spontaneous pneumothorax and renal cancer, two of three characteristic features of BHD syndrome. Although the paternal relatives appear to be affected with BHD mutation, we could not obtain consent for gene analysis from the family. (B) Sequencing of genomic DNA revealed superimposed nucleotide chromatograms near the beginning of exon 6 (upper panel). Cloning of the PCR products demonstrated clones carrying the wild-type sequence (middle panel) and those carrying the deletion of 10 nucleotides (gtccctccag) including splice acceptor signal, “ag”, in intron 5 (lower panel). The location of the deletion is indicated by a rectangle in the wild-type sequence. (C) Effect of the mutation on the splicing of BHD transcript was examined by reverse transcriptase PCR using total RNA isolated from an Epstein–Barr virus-transformed lymphoblastoid cell line (EBV-LCL). RT-PCR products were size-fractionated on 2% agarose gel (upper panel) and location of forward (5′-CGGACATGTGCGAGGGCTGC-3′ in exon 5) and reverse (5′-GGAATGGCGTGAAGGCTGTG-3′ in exon 7) primers used in RT-PCR is schematically presented. DNA size markers are shown on the left. NC, negative control (no cDNA in reaction mixture); PC, positive control (EBV-LCL established from a healthy Japanese volunteer), respectively. The control subject had a major band with an expected size of 453 bp, whereas the proband had another band with an expected size of 231 bp, corresponding to the DNA fragment from the exon 6-skipped mRNA transcript. The band detected under the 453 bp major band is a heteroduplex consisting of both the 453 and 231 bp bands formed during PCR. Note that a tiny amount of exon 6-skipped mRNA transcript may be generated in EBV-LCL from control subjects. Assessment of the size of each DNA fragment was confirmed by direct sequencing and cloning of PCR products.
In this study, we identified four nucleotide alterations that are considered to be polymorphisms in the BHD gene (table 3). One is located in the non-coding region of exon 1, two exist in an intronic sequence and there is one silent mutation in exon 13. As we did not perform genomic sequencing in three cases (patients B4, B5 and B8), in which screening with DHPLC revealed no heteroduplex formation, we cannot exclude false negative results regarding germline BHD mutation in these cases. However, a false negative result can occur even in direct genomic sequencing if of a large genomic deletion including the BHD gene exists.
Polymorphisms in the BHD gene
Clinical features of the patients with a BHD germline mutation
None of the patients (B1, B2, B3, B6 and B7) had fibrofolliculomas nor renal tumour, regarded as two of three clinical important phenotypes of the BHD syndrome. As renal tumours usually have a 2.5-fold higher rate of development in men than in women and are usually diagnosed at the median age of 48 years (range 31–71 years),17 our group of patients with BHD germline mutation may comprise too many women and be too young to have developed the renal features of BHD syndrome. All patients had lung cysts, as shown demonstrated by HRCT of the chest, repeated episodes of pneumothorax in bilateral lungs and a family history of spontaneous pneumothorax. We could not obtain consent to analyse the BHD gene from relatives of the patients enrolled in the study, with the exception of the family of patient B1: father (61 years old at the time of the study), mother (56 years), brother (34 years) and nephew (6 years) were examined. Genetic study showed that mother carried the BHD germline mutation and it was transmitted to the proband, her brother and her nephew. The brother had experienced repeated episodes of pneumothorax but without renal tumour and fibrofolliculomas. The mother had neither renal tumour nor fibrofolliculomas and had never experienced any episode of spontaneous pneumothorax, but she was found to have multiple pulmonary cysts using HRCT of the chest (figure 3B). We did not perform chest CT scan for the nephew, as he was only 6 years old and had no overt signs of pneumothorax. Patient B6 had no skin lesions (fibrofolliculomas) and no renal tumour, but she had experienced spontaneous pneumothorax in both sides of the lung at the age of 35 years and multiple lung cysts were found on the HRCT scan of the chest. It was later discovered that she was a member of a large family with spontaneous pneumothorax (figure 2A).

{kind=link}
{kind=link}
{kind=link}
Representative chest HRCT images of the study participants. Lower lung images of (A) patient B1, (B) her mother, (C) patient B5, and (D) upper lung field from patient B8. No BHD mutation was detected in patients B5 and B8. Compared with patient B1 (A) and her mother (B), in whom a diagnosis of BHD syndrome was made in this study, patient 5 (C) has more cysts detectable in both lung fields and patient B8 (D) has cysts showing subpleural distribution.
Figure 3 shows typical HRCT findings of the chest of BHD patients. There are characteristic findings: most lung cysts were ranged on both lung fields and located predominantly in the basal and mediastinal regions of the lungs. Blood vessels were identified in or next to some of the lung cysts. The cysts were variously sized, and rimmed by smooth thin walls. The surrounding parenchyma was generally unremarkable. The number of cysts seems to be small when all CT images of the lungs were evaluated (table 1): <100 except for patient B2. In addition, the distribution of lung cysts in patients with no BHD mutation appears to be different: they were located in both upper lobes and at the periphery of the lung (patient B8; figure 3D).
DISCUSSION
In this study, we identified BHD germline mutations in five of eight patients with multiple lung cysts and recurrent pneumothorax. None of the affected patients had the skin lesions or renal tumours that are considered to be the clinical hallmarks of BHD syndrome.10 Other studies have reported that pneumothorax can be the only clinical sign of BHD syndrome as an underlying disease.18,19 The development of the clinical features of BHD syndrome seems to be age-dependent. Fibrofolliculomas are reported to occur in patients with BHD after the age of 25–35 years10,17,22 and may be easily missed if they appear as subtle papules with normal skin colour or are hidden by makeup. In contrast, renal neoplasms predominantly develop after the age of 40 years.10,17 We carefully investigated for the presence of both skin and renal lesions in our study population, but could not identify either. However, we cannot exclude the possibility that they may develop in the future, as the mean age of the patients diagnosed with BHD syndrome at the time of genetic testing was 36.6 years old (range 30–40). In other words, pulmonary feature may precede the development of the other two phenotypes,10as one (patient B2) experienced her first pneumothorax at the age of 16 years and one case report exists describing a boy who had a spontaneous pneumothorax at the age of 7 years.23
There is increasing evidence that BHD syndrome shows not only genetic but also considerable clinical heterogeneity. The skewed clinical expression in our study population could be a variable genotype–phenotype correlation or the result of involvement of a combination of three major organs rather than the chronological development of each phenotype. All mutations we detected in this study were insertions or deletions, including one splice donor site mutation, and four of the five are novel. All mutations are predicted to cause a frameshift leading to protein truncation, which is in agreement with the results of studies reported by other groups.13,17 To date, one example of the genotype–phenotype relationship in BHD syndrome has been reported. The frequency of renal tumours was significantly lower in patients with BHD with a C deletion mutation in the C8 tract of exon 11 than those with a C insertion mutation in the same mutational hotspot.17 Two studies18,19 have already reported that germline BHD mutation is a genetic defect associated with hereditary spontaneous pneumothorax, and none of our family members had skin or renal features of BHD syndrome. Painter et al18,19 identified a 4 bp deletion in exon 4 in a large Finnish family with spontaneous pneumothorax, and Graham et al18,19 found nonsense mutations of exon 9 and 12, respectively, in 2 of 12 families with familial spontaneous pneumothorax.
Our study examined patients with multiple lung cysts of undetermined cause, who had episodes of pneumothorax. Germline BHD mutations were found in five index cases whose family members had pneumothorax, but not in the remaining three index cases whose family members had no pneumothorax. Accordingly, eight BHD mutations, which predisposed only to the pulmonary features of BHD syndrome, were collected but there does not at present appear to be any specific genotype–phenotype correlation with these pulmonary features. Further study is needed, however, to resolve the question of whether BHD mutations that preferentially predispose to pulmonary features of BHD syndrome exist. Although a high detection rate of BHD mutations was noted in our study population compared with that of Graham et al,18,19 this may be due to differences in study populations.
It is recognised that the clinical presentation in tumour-suppressor gene syndromes can be variable. Phenotypic features may vary due to the combination of the involvement of skin, lung and kidney, three target organs affected by BHD mutations. Schmidt et al17 reported that of their 53 families with BHD syndrome whose members had either a germline BHD mutation or the affected BHD haplotype, 41.5% (22/53) of the families had skin, lung and renal features, 41.5% (22/53) had members with skin and lung phenotypic features, 2% (1/53) had renal and lung phenotypic features, 13% (7/53) had only skin papules and 2% (1/53) had renal tumours and skin papules. The lungs appear to be frequently involved in BHD syndrome, as in their study, 85% (45/53) of the families had members who developed lung cysts or spontaneous pneumothorax, and 85% (110/129) of patients with BHD who were examined by chest CT scan were found to have one or more lung cysts. In our study, only the relatives of patient B1 were willing to participate in genetic testing and the proband’s mother (56 years old) was found to have BHD, although she had neither skin lesion nor a history of pneumothorax. She did, however, have lung cysts but not renal tumours on CT scan. Although the number of study subjects and family members we examined was very small, the study indicates that pulmonary features can be an isolated phenotypic expression of BHD syndrome.
Given that multiple lung cysts with or without the occurrence of pneumothorax can be an isolated phenotypic expression of BHD syndrome, and has a high incidence, BHD syndrome should be considered in the differential diagnosis for spontaneous pneumothorax, especially in patients with a family history18,19 and those with cystic lung diseases, such as lymphangioleiomyomatosis (LAM) and LCH, which frequently complicate pneumothorax. It has been reported that chest HRCT of BHD patients shows thin-walled cysts of varying sizes with normal intervening lung parenchyma,24 and the predominant distribution of cysts is in the basilar and mediastinal regions of the lungs.25 We confirmed these findings in our five patients with BHD (figure 3). Furthermore, we found that the number of cysts in the lung fields is usually <100 (table 1). LAM and LCH, particularly in the early stages, need to be carefully distinguished from BHD syndrome. LAM, especially in association with tuberous sclerosis complex, may have several clinical feature in common with BHD syndrome: facial skin lesions (angiofibromas, but not fibrofolliculomas), renal tumours (usually angiomyolipomas, but may be renal cell carcinomas) and recurrent episodes of pneumothorax, even in the early stage of the disease when the number of lung cysts is still limited.26 In one case report,27 a biopsy of a facial rash in a pre-menopausal woman (42 years old) with recurrent pneumothorax and radiological findings of multiple cysts was initially interpreted as a sebaceous adenoma. The patient was eventually diagnosed with BHD syndrome from the results of a lung biopsy, a detailed family history and re-evaluation of the skin pathology. BHD syndrome appears to have no gender predilection10,17 whereas LAM occurs exclusively in female.28 All patients identified with a BHD germline mutation in this study were women, but this may have been subject to bias, as our hospital is the main institution in Japan to which patients with suspected or diagnosed LAM are most often referred.
In conclusion, our study confirms that pulmonologists should be aware of and be able to recognise this rare inherited disorder. Descriptions of BHD syndrome are mainly published in the dermatological literature and are rather scanty in the respiratory literature. However, pulmonologists have the opportunity of early diagnosis and management for possible future cancer development in patients with this syndrome. Molecular analysis of the BHD gene should be systematically conducted in patients with multiple lung cysts even in the absence of characteristic fibrofolliculomas on the face and renal tumours.
Key points
-
It is increasingly recognised that BHD syndrome shows not only genetic but also considerable clinical heterogeneity. Phenotypic features can be variable due to involvement of the combination of the skin, lung and kidney, three target organs affected by BHD mutations.
-
We found that five of eight patients with multiple lung cysts and recurrent pneumothorax, but no skin lesions or renal tumours, had BHD germline mutations. All mutations we detected were insertions or deletions, including one splice donor site mutation, and four of them are novel.
-
Pulmonologists should be aware that BHD syndrome can occur as an isolated phenotype with pulmonary involvement.
Acknowledgments
We would like to thank Dr Sakae Honma, MD, PhD, Department of Respiratory Medicine, Toho University School of Medicine and Dr Hitoshi Tokuda, MD, PhD, Department of Respiratory Medicine, Social Insurance Central General Hospital, who kindly referred the patients.
REFERENCES
Footnotes
-
This study was supported by Grant-in-Aid for Scientific Research No. 18659242 (Seyama K) and in part by the High Technology Research Center Grant from the Ministry of Education, Culture, Sports, Science and Technology, Japan.
-
Competing interests: None declared.
-
Published Online First 11 May 2007