Article Text

Abstract
Objective: To identify potentially confounding variables for the interpretation of plasma N-terminal pro brain natriuretic peptide (NT-proBNP).
Design: Randomly selected subjects filled in a heart failure questionnaire and underwent pulse and blood pressure measurements, ECG, echocardiography, and blood sampling.
Setting: Subjects were recruited from four Copenhagen general practices located in the same urban area and were examined in a Copenhagen University Hospital.
Patients: 382 women and 290 men in four age groups: 50–59 years (n = 174); 60–69 years (n = 204); 70–79 years (n = 174); and > 80 years (n = 120).
Main outcome measures: Associations between the plasma concentration of NT-proBNP and a range of clinical variables.
Results: In the undivided study sample, female sex (p < 0.0001), greater age (p < 0.0001), increasing dyspnoea (p = 0.0001), diabetes mellitus (p = 0.01), valvar heart disease (p = 0.002), low heart rate (p < 0.0001), left ventricular ejection fraction ⩽ 45% (p < 0.0001), abnormal ECG (p < 0.0001), high log10[plasma creatinine] (p = 0.0009), low log10[plasma glycosylated haemoglobin A1c] (p = 0.0004), and high log10[urine albumin] (p < 0.0001) were independently associated with a high plasma log10[plasma NT-proBNP] by multiple linear regression analysis.
Conclusions: A single reference interval for the normal value of NT-proBNP is unlikely to suffice. There are several confounders for the interpretation of a given NT-proBNP concentration and at the very least adjustment should be made for the independent effects of age and sex.
- amino-terminal pro brain natriuretic peptide
- heart failure
- population study
Statistics from Altmetric.com
Natriuretic peptides are gaining increased recognition as diagnostic markers in heart failure, and brain natriuretic peptide (BNP)1,2 and its amino terminal portion, N-terminal pro brain natriuretic peptide (NT-proBNP)3—which may have advantages because of its greater stability4—have proved especially promising. Concentrations of BNP and NT-proBNP are related to left ventricular filling pressures5 and wall stress.6
All previous studies of the diagnostic value of BNP in heart failure, whether focusing purely on left ventricular systolic dysfunction7–10 or on a clinical diagnosis of heart failure,11,12 have consistently reported a very high negative predictive value of BNP (0.98 to 1.00), while the positive predictive value has been lower (0.16 to 0.42). The high negative predictive value makes BNP appear well suited for population screening; however, the low positive predictive value may pose a problem in any population screening or diagnostic setting because of the large number of false positive results that are likely to be found.
Our aim in this population based study was to try to identify potentially confounding variables for the interpretation of the plasma concentration of NT-proBNP, which might lead to better diagnostic performance of the marker.
METHODS
Patients
The study sample was recruited from four Copenhagen general practitioners located in the same urban area. The sole inclusion criterion was age between 50–90 years. Exclusion criteria were inability to cooperate (for example, because of dementia), residence in a nursing home, and lack of response to two written invitations.
Study design
In order to obtain a sufficient number of elderly subjects, the study sample was stratified to include at least 120 subjects in each decade. An invitation to participate in the study was sent to all persons between 50–90 years of age assigned to the first two general practitioners. From the third practice, all persons aged 60–90 years were invited, and from the last practice, all persons aged 80–90 years. Seventy per cent of those invited participated in the study. The attendance was higher among younger individuals (approximately 75%), while it was approximately 50% in the oldest decade. The study was designed to be representative of the background population in Copenhagen by compensating for the lower response rate in the older age groups through oversampling in those groups.
Subjects from general practitioners 1 and 2 entered the study in the autumn of 1997; they completed a questionnaire and had echocardiography and a blood pressure measurement. They were recalled by the autumn of 1998 (n = 424), when they had an ECG and a blood sample was taken. Subjects from general practitioners 3 (n = 207) and 4 (n = 41) had all the investigations in the autumn and winter of 1998-99. Thus all the subjects in the study had each investigation done once.
The local ethics committee approved the study and the patients gave their written informed consent.
Heart failure questionnaire
All subjects filled in a heart failure questionnaire on their medical history, symptoms, drug history, and alcohol and tobacco consumption. Symptoms of heart failure were recorded from questions on ankle swelling and breathlessness (self reported). The degree of breathlessness was recorded from the questionnaire using the World Health Organization classification (grade 1, no dyspnoea; grade 2, dyspnoea when vacuum cleaning or climbing stairs to the next floor; grade 3, dyspnoea when walking on an even road; grade 4, dyspnoea on minimum exertion; grade 5, orthopnoea; grade 6, dyspnoea at rest). Self reported medical history was recorded from questions on hospital admissions (with special emphasis on admissions for heart failure, pulmonary oedema, and myocardial infarction), history of ischaemic heart disease (previous myocardial infarction and/or angina), history of hypertension, and history of diabetes mellitus (insulin treated or non-insulin-dependent). Each questionnaire was evaluated immediately after it was completed and where there were any omissions or inconsistencies the subjects were contacted by telephone to ensure the highest possible data quality.
Measurements
Heart rate and blood pressure were measured and a 12 lead standard ECG was recorded and evaluated according to the Minnesota code. Using predefined criteria (absence of arrhythmias, ST deviation, Q waves, hypertrophy, or abnormal left ventricular axis), each ECG was classified as either normal or abnormal.
The subjects were also submitted to apical four and two chamber and apical long axis echocardiograms. Left ventricular systolic function was evaluated by 16 segment wall motion score indexing, from which the left ventricular ejection fraction was calculated by multiplying by 30.13 Heart valves (aortic, mitral, and tricuspid) were evaluated by the colour Doppler technique in apical four and two chamber or long axis echocardiograms. Any sign of stenosis or incompetence led to further assessment with continuous wave Doppler and M mode atrial measurements. Valve defects were characterised on a four grade scale as normal, mild, moderate, or severe. Only subjects with valve defects described as moderate or severe were diagnosed as having valve disease in this study. Two independent and experienced observers evaluated all echocardiograms.
Blood and urine samples were collected for biochemical markers (plasma NT-proBNP, plasma creatinine, plasma glycosylated haemoglobin A1c (HbA1c), and urinary albumin/creatinine ratio). All blood samples were collected with the participant in a sitting position and after at least 15 minutes of rest. Blood samples for analyses of the biochemical markers were immediately centrifuged at 4°C and plasma samples were stored in disposable tubes containing aprotinin (kallikrein inhibitor) in a −80°C freezer.
Plasma concentrations of NT-proBNP were measured by a novel, highly sensitive and specific immunoassay based on a sandwich format using unextracted EDTA plasma. The sensitivity of the assay was < 3.0 pmol/l and the intra-assay and interassay coefficients of variation were 1.3% and 4.8%, respectively.14
“Normal” subjects
Subjects were classified as having a very low probability of heart disease and subgrouped as normal if the following criteria were fulfilled: no congestive heart failure, no ischaemic heart disease, no history of hypertension, no diabetes mellitus, no lung disease, receiving no cardiovascular drugs, and having a left ventricular ejection fraction of ⩾ 60%, a blood pressure of < 140/90 mm Hg, and a normal ECG.
Statistics
Verification of the normal distribution of continuous data was accomplished using histograms and normal plots. Measures of plasma NT-proBNP, plasma creatinine, urine albumin, and plasma glycosylated haemoglobin showed a log normal distribution and were consequently logarithmically (log10) transformed. Two sample t tests were done between mean or geometric mean values of variables in the normal patients and all patients except the normal patients, and between mean or geometric mean values of variables in men and women in case of normal or log normal distribution of data; alternatively Mann–Whitney tests were done. Dichotomous data were analysed by continuity adjusted χ2 tests. Plasma concentrations of NT-proBNP in the different age groups for each sex were compared using one way analyses of variance. Variables potentially associated with the plasma concentration of NT-proBNP in all subjects, in all subjects except those diagnosed with diabetes mellitus, and in the normal subjects were analysed by multiple linear regression analyses with backward elimination.
All tests were two sided and a significance level of 5% was used. All tests were done using the Statistical Analysis System (SAS Institute, Cary, North Carolina, USA).
RESULTS
Basic characteristics and measurements
The criteria for normality, as outlined in the methods section, were met by 130 of the 672 subjects; these were consequently classified as “normal”. Clinical characteristics, including fundamental measurements for all subjects and for subjects classified as normal, are given in table 1.
Clinical characteristics of the subjects in the study
Variables independently associated with plasma NT-proBNP
In all subjects, female sex, greater age, increasing dyspnoea, diabetes mellitus, valvar heart disease, lower heart rate, left ventricular ejection fraction ⩽ 45%, abnormal ECG, high log10[plasma creatinine], low log10[plasma HbA1c], and high log10[urine albumin] were all independently associated with a high plasma concentration of log10[NT-proBNP] by multiple linear regression analysis (table 2).
Variables independently associated with the plasma concentration of N-terminal pro brain natriuretic peptide
When leaving out subjects diagnosed with diabetes mellitus, the same independent variables were identified: sex (0 = female, 1 = male), regression coefficient (rc) (SE) = −0.193 (0.031), p < 0.0001; age (years), rc = 0.019 (0.002), p < 0.0001; increasing dyspnoea, rc = 0.044 (0.012), p = 0.0002; valvar disease, rc = 0.364 (0.117), p = 0.002; heart rate (beats/min), rc = −0.005 (0.001), p < 0.0001; left ventricular ejection fraction ⩽ 45%, rc = 0.198 (0.052), p = 0.0002; abnormal ECG, rc = 0.182 (0.034), p < 0.0001; log10[plasma creatinine (μmol/l)], rc = 0.279 (0.081), p = 0.0006; log10[plasma HbA1c (%)], rc = −0.600 (0.149), p < 0.0001; and log10[urine albumin (%)], rc = 0.078 (0.015), p < 0.0001, intercept (0.163 (0.419), NS).
In the normal subjects, female sex, greater age, and low diastolic blood pressure were independently associated with a high plasma concentration of log10[NT-proBNP] (table 2).
Greater age was by far the most important independent variable in explaining the plasma concentration of log10[NT-proBNP], as in all models it was much more strongly associated with log10[NT-proBNP] than any of the other independent variables.
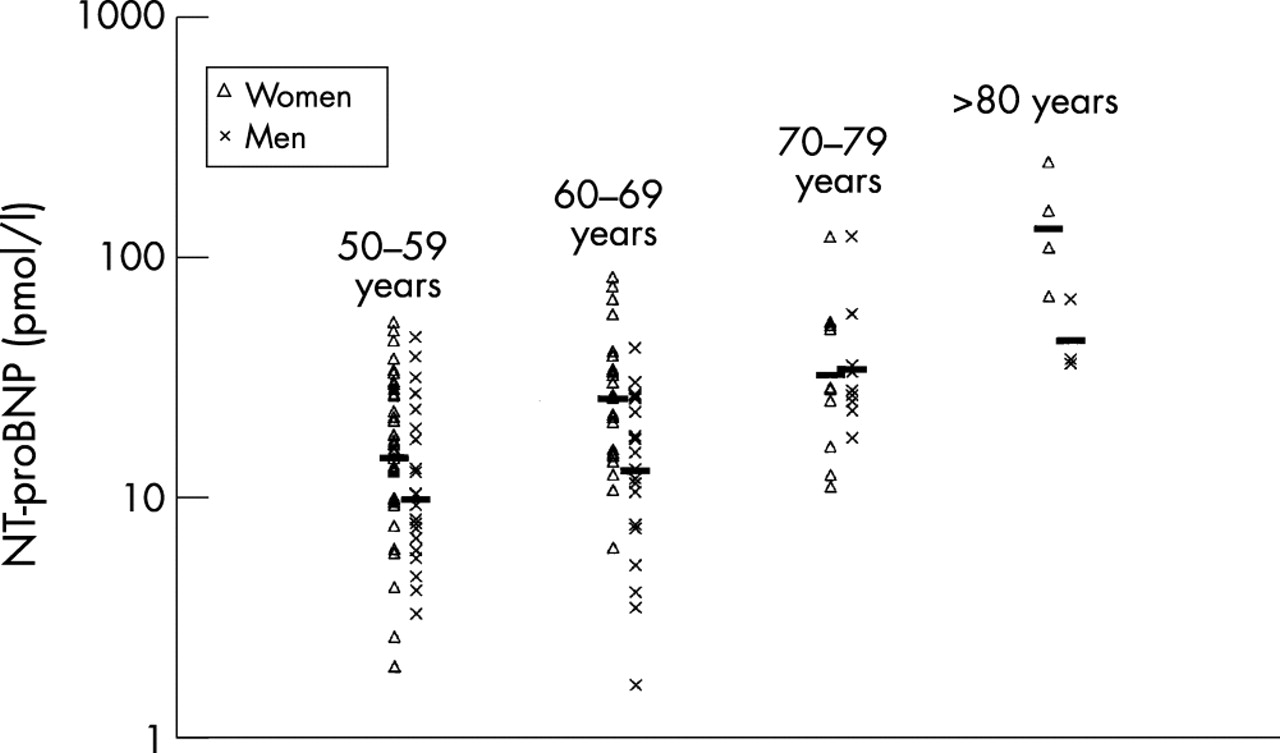
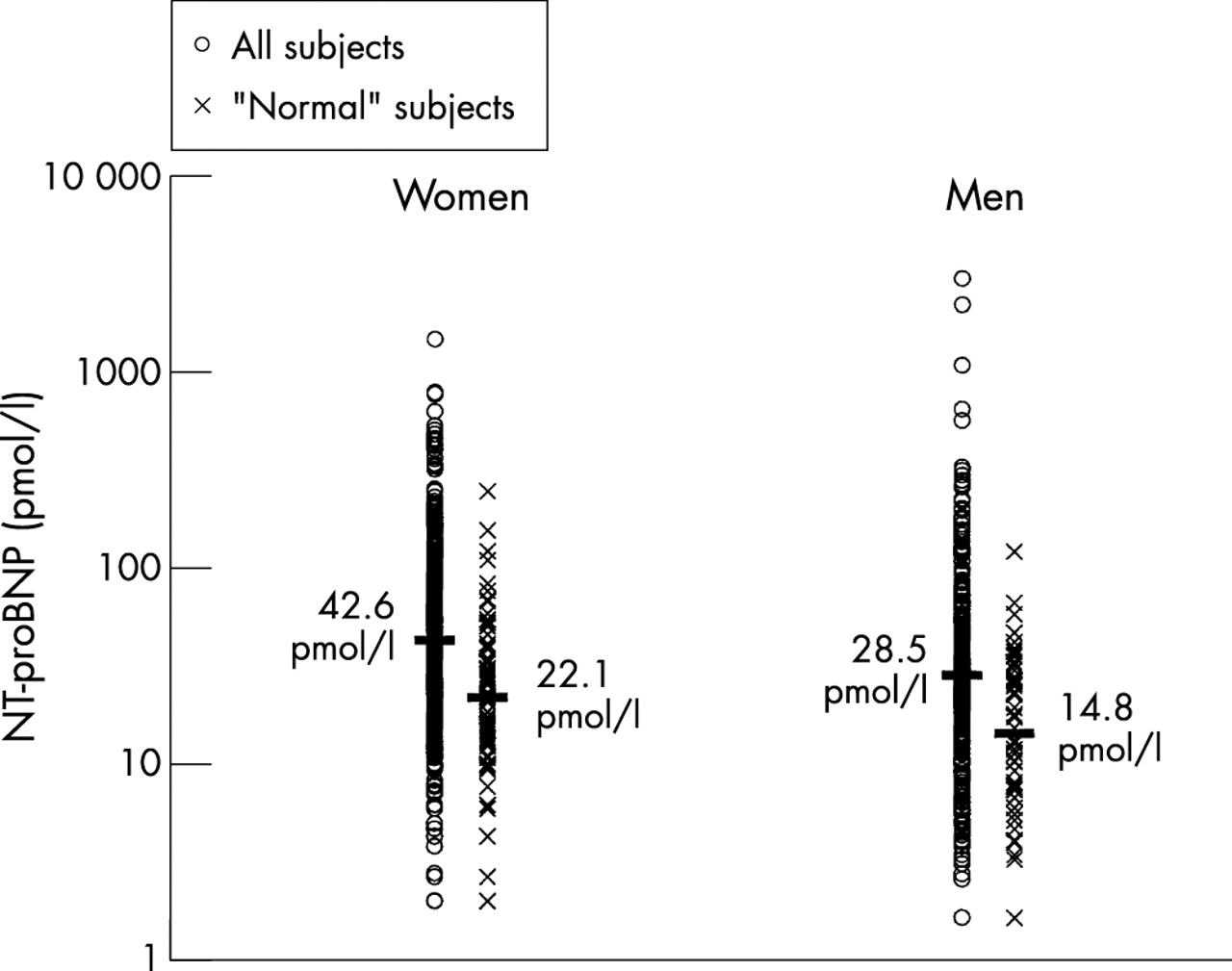
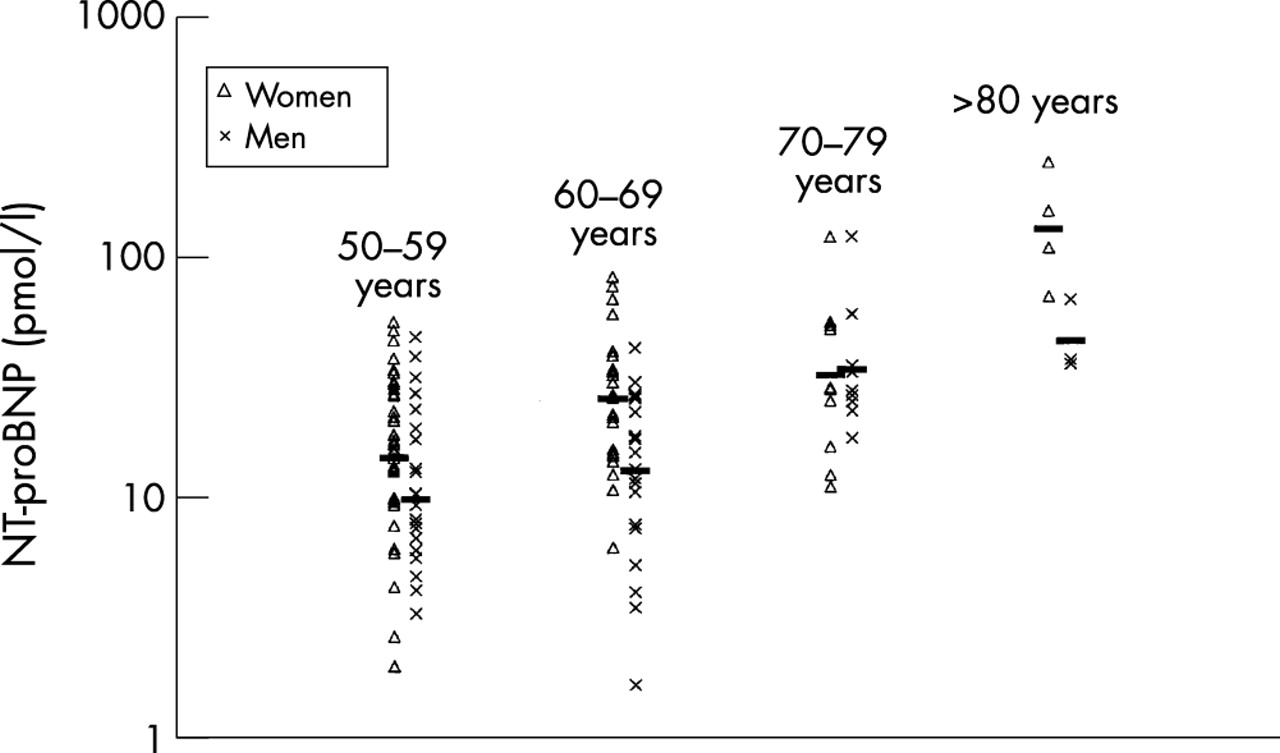
As sex was also identified as a significant independent variable, plasma concentrations of NT-proBNP in various age and sex groups in all subjects (table 3 and figs 1 and 2) and in the normal subjects (table 4 and figs 1 and 3) were calculated. In all subjects and in the normal subjects, plasma concentrations of NT-proBNP were significantly higher in women than in men, and the mean concentration of plasma NT-proBNP almost doubled per age decade regardless of sex or “normality” status.
Geometric mean concentrations of N-terminal pro brain natriuretic peptide in different age and sex groups in the undivided study sample
Geometric mean concentrations of N-terminal pro brain natriuretic peptide in different age and sex groups in subjects defined as normal in the study sample¶

Plasma concentrations of N-terminal pro brain natriuretic peptide in men and women in the study sample. Horizontal bars indicate geometric mean concentrations. Definition of “normal” subject: no congestive heart failure, no ischaemic heart disease, no history of hypertension, no diabetes, no lung disease, no cardiovascular drugs treatment, left ventricular ejection fraction of ⩾ 60%, blood pressure < 140/90 mm Hg, and a normal ECG. NT-proBNP, N-terminal pro brain natriuretic peptide.

Plasma concentrations of N-terminal pro brain natriuretic peptide in different age and sex groups in the undivided study sample. Horizontal bars indicate geometric mean concentrations.
{kind=link}
{kind=link}
{kind=link}
Plasma concentrations of N-terminal pro brain natriuretic peptide in different age and sex groups in the subjects defined as “normal” in the study sample. Horizontal bars indicate geometric mean concentrations. Definition of normal subject: no congestive heart failure, no ischaemic heart disease, no history of hypertension, no diabetes, no lung disease, no cardiovascular drug treatment, left ventricular ejection fraction of ⩾ 60%, blood pressure < 140/90 mm Hg, and a normal ECG.
DISCUSSION
This is the first population based study to confirm that the plasma concentration of NT-proBNP increases with age and that it is consistently higher in women than in men. In addition, we have identified several different factors of independent significance for the plasma concentration of the marker.
It has been shown repeatedly that the natriuretic peptides have significant potential as markers for left ventricular systolic impairment and increased left ventricular dimensions, as well as for the clinical syndrome of heart failure. In population based studies, these biochemical markers have proved their legitimacy to such a degree that the European Society of Cardiology has recently included a raised concentration of any one of these peptides in the diagnosis of heart failure.15
Focus has concentrated on BNP and its amino terminal portion NT-proBNP, and as these markers are likely to be incorporated into clinical practice within the foreseeable future, an increased understanding of the physiology and pathophysiology of the markers in a general population setting is needed, particularly to establish normal reference intervals.
It is generally accepted that BNP and thus NT-proBNP are mainly released locally from the left ventricle in response to increased wall tension or stretch,16 accounting for their value as diagnostic markers in heart failure—a condition often characterised by high left ventricular wall stress owing to increased left ventricular dimensions and wall thinning.
The identification of dyspnoea,17 valvar heart disease,18–21 a low left ventricular ejection fraction,7 and an abnormal ECG22 as variables of independent significance for the value of plasma NT-proBNP in the present study are all readily explicable by this well known association with left ventricular wall stress, and may thus account for the diagnostic value of the marker.
The finding that plasma concentrations of NT-proBNP were higher in women than in men, regardless of age or normality status, has previously been reported in one population based study,23 and seems to be an important factor that needs to be taken into account when defining future reference intervals for the marker. The association is, however, not easily explained, though a lower volume of distribution in women than in men could partly account for the difference.
The plasma concentration of NT-proBNP almost doubled per age decade in the present study, regardless of sex or normality status. This association has previously been reported in normal subjects and probably reflects increased myocardial mass,24 chamber specific alterations in gene expression,25 and a possible reduction in the renal clearance of natriuretic peptides with aging, not reflected completely by the plasma creatinine concentration.26
The finding that a high plasma creatinine was independently associated with a high plasma NT-proBNP in our study came as no surprise, as high natriuretic peptide concentrations have been reported in patients with renal failure27–30 and in heart failure patients with increased plasma creatinine.23,31 As well as a reduced clearance of the natriuretic peptides, increased cardiac afterload caused by fluid retention, leading to increased left ventricular wall stress, is a possible explanation for the effect of impaired renal function on the plasma concentration of NT-proBNP.20,32,33 This may also be part of the reason why a diagnosis of diabetes mellitus was independently related to a high plasma NT-proBNP, as previous studies have shown raised BNP concentrations in diabetic patients with and without microalbuminuria, probably explained by the presence of an early stage of diabetic nephropathy not yet affecting the plasma creatinine level.34 It was striking that when diabetic subjects were excluded from analysis in our study, a high urine albumin concentration remained independently associated with a high plasma NT-proBNP concentration, probably reflecting the onset of nephropathy.
We have no explanation for the surprising finding of a low glycosylated haemoglobin concentration as a predictor of a high plasma NT-proBNP concentration, nor for the finding that a low heart rate was independently predictive of a high plasma NT-proBNP concentration. The latter association was unaffected by exclusion of subjects on treatment with β blocking agents.
Conclusions
Our population based results indicate that a single reference interval for normal plasma NT-proBNP will probably not suffice, as adjustments for the independent effects of age and sex appear necessary. In addition, we have identified various other confounders involved in the interpretation of a given plasma NT-proBNP concentration, among which impaired renal function seems to be the most important.
Acknowledgments
This study was funded by F Hoffmann-La Roche Ltd, Basel, Switzerland; Merck Sharp & Dohme, Glostrup, Denmark; the Research Fund of the Copenhagen Hospital Corporation, Copenhagen, Denmark; Sophus Jacobsen and Wife Astrid Jacobsen’s Fund, Copenhagen, Denmark; Arvid Nilsson’s Fund, Copenhagen, Denmark; Leo Pharmaceutical’s Research Fund, Copenhagen, Denmark; Svend Hansen and Wife Ina Hansen’s Fund, Copenhagen, Denmark; Lykkefeldt’s Fund, Copenhagen, Denmark; Ove Villiam Buhl Olesen and Wife Edith Buhl’s Memorial Fund, Copenhagen, Denmark; Elisabeth M Schlinsog’s Fund, Copenhagen, Denmark.