Article Text

Abstract
Objectives Diastolic dysfunction (DD), a key driver of long-term Fontan outcomes, may be concealed during standard haemodynamic evaluation. We sought to identify Fontan patients with occult DD using ‘ventricular stress testing’ with rapid volume expansion (RVE).
Methods Cardiac catheterisation with RVE was performed routinely in Fontan patients between 11/2012 and 4/2015. Baseline and post-stress haemodynamic data were compared using t test, Mann–Whitney U test, χ2 and Fisher's exact tests. A post-stress ventricular end diastolic pressure (EDP) threshold of 15 mm Hg defined occult DD.
Results Forty-six Fontan patients (48% female, median age 14.1 (IQR 9.1 to 21.3) years) were included. The median Fontan duration was 10.8 (IQR 5.1 to 17.8) years and dominant left ventricular morphology was present in 63% of patients. Volume expansion increased mean Fontan pressure (15.2±2.5 vs 12.4±2.2 mm Hg, p<0.001), pulmonary capillary wedge pressure (11.3±2.6 vs 7.9±2 mm Hg, p<0.001) and EDP (12.7±3.3 vs 8.5±2.1 mm Hg, p<0.001). Sixteen patients (35%) had occult DD, demonstrating higher baseline EDP (10.3±1.9 vs 7.6±1.5 mm Hg, p<0.001) and greater increase in EDP (6.3±2.4 vs 3.1±1.4 mm Hg, p<0.001) compared with patients without DD. Higher baseline EDP, lower baseline cardiac index and longer duration of Fontan circulation were associated with higher post-stress EDP. There were no complications related to RVE.
Conclusions Ventricular stress testing by RVE is feasible, safe and identifies a subgroup of Fontan patients with occult DD. Higher baseline EDP and longer duration of Fontan circulation are associated with worse diastolic function. Future work is necessary to better understand the aetiology, associations and clinical implications of occult DD in Fontan survivors.
Statistics from Altmetric.com
Major improvements in perioperative management have resulted in reduced early morbidity and mortality in patients with univentricular physiology.1–4 However, it remains common for Fontan-palliated survivors to encounter the early onset of symptomatic heart failure with associated multiorgan dysfunction (so-called ‘failing Fontan physiology’).1 ,3 ,5–8 Ongoing efforts to improve Fontan outcomes have largely shifted from the acute perioperative setting to longer-term management of presymptomatic and symptomatic failing Fontan physiology.9 ,10 In this regard, aggressive medical therapy has become the norm for treatment of single-ventricle systolic dysfunction, and a number of recent studies have evaluated the impact of pulmonary vasodilator therapy on functional outcomes including exercise capacity and quality of life.11–13 However, many patients with failing Fontan physiology have neither overt systolic dysfunction nor evidence of reversible pulmonary endothelial dysfunction.
Recent work from our group and others has suggested that diastolic dysfunction (DD) of the single ventricle may play a substantial role in the development of failing Fontan physiology.14–17 The diagnosis of DD is difficult in the univentricular heart. Nonetheless, the presence of abnormal diastolic function parameters, suggestive of abnormal early relaxation (reduced E-wave velocity) and elevated atrial filling pressure (abnormal E/e′ ratio), was reported in 72% of Fontan patients in the large Pediatric Heart Network Fontan Cross-Sectional Study.8 However, traditional echocardiographic indices of diastolic function have not been validated in the Fontan population, and there is no demonstrable relationship between these diastolic abnormalities and functional performance. Similarly, invasive haemodynamic evaluations are frequently unrevealing, with symptomatic patients often demonstrating unremarkable Fontan circuit pressure and single-ventricle end diastolic pressure (EDP). Improved diagnostic criteria are therefore necessary both to better understand the mechanisms and natural history of univentricular DD, and to identify patients who might benefit from targeted therapies. In an effort to better understand the prevalence and implications of DD in the Fontan cohort, we performed a proof-of-principle study to assess the feasibility and outcomes of a clinical protocol of invasive ‘ventricular stress testing’ performed using rapid volume expansion in Fontan patients without evidence of overt DD.
Methods
Since November 2012, Fontan patients undergoing elective and clinically indicated cardiac catheterisation followed a clinical ventricular stress testing protocol of rapid volume expansion. Patients with a baseline single-ventricular EDP ≥15 mm Hg, mean Fontan pressure ≥18 mm Hg, severe ventricular systolic dysfunction, determined to be in an acute or chronic volume overload state, undergoing non-elective catheterisation (eg, for arteriopulmonary collateral embolisation in the setting of haemoptysis) or at the discretion of the primary operator, were excluded from the clinical protocol. For the purposes of this study, a query of the institutional catheterisation database was performed to identify Fontan patients who underwent cardiac catheterisation between 11/2012 and 4/2015 at our institution. Patients with Fontan physiology who underwent clinically indicated catheterisation with protocoled ventricular stress testing were included in the analysis.
The ventricular stress testing protocol consisted of the following: After a complete baseline haemodynamic assessment and prior to contrast angiography, rapid volume expansion was performed. This consisted of a 15 mL/kg bolus of normal saline administered rapidly (<5 min) via central venous access (eg, the venous sheath). After a 5 min equilibration period, repeat haemodynamic assessment was performed, consistent with prior protocols employing rapid volume expansion.18 ,19 Pressure measurement was recorded using fluid-filled catheters and a digital transducer system. Cardiac index was determined using the Fick equation. When possible, oxygen consumption (VO2) was directly measured.20
Record abstraction was performed to identify selected patient characteristics, including primary cardiac diagnosis, morphology of single ventricle, age, weight, date of Fontan completion, type of Fontan, presence of fenestration and current cardiac medications. Procedural characteristics collected included haemodynamic variables measured at baseline and following fluid challenge: heart rate, mean Fontan circuit pressure (in the lateral tunnel or extracardiac conduit), mean pulmonary capillary wedge pressure, ventricular EDP, systolic aortic pressure, oxygen saturations (mixed venous, descending aorta, pulmonary arteries) and VO2 (measured or assumed). Adverse events possibly related to fluid administration (eg, need for additional diuresis or unplanned overnight admission) were collected.
Occult DD was defined as a baseline EDP of <15 mm Hg and a post-volume load EDP of ≥15 mm Hg. The selection of 15 mm Hg as an EDP cut-off for DD stems from the definition of DD employed in prior invasive studies using volume loading, such as in pulmonary hypertension and restrictive pericarditis populations.18 ,19
Statistical analysis
Data are presented as mean±SD or median (IQR) for continuous variables and frequency (%) for categorical variables. Continuous data were compared using independent t test and Mann–Whitney U test while categorical data were compared using χ2 or Fisher's exact tests, as appropriate. Logistic regression and Pearson's correlation coefficients were performed to identify factors associated with occult DD. Linear regression was performed to assess for predictors of post-volume loading EDP and the absolute change in EDP from baseline.
The cohort was analysed via two different approaches. In the first approach, the cohort was divided into subgroups by the presence or absence of occult DD. Factors were analysed for an association with occult DD. In the second approach, the entire cohort was evaluated using two clinically relevant haemodynamic variables as continuous outcome measures: (1) post-volume load EDP and (2) absolute change in EDP. Regression analysis was performed to assess for predictors of higher post-volume load EDP and absolute change in EDP. A p value of ≤0.05 was considered statistically significant. All statistical analyses were performed using SPSS V.21.0 (IBM Corporation, Armonk, New York, USA).
Results
Patients
Eighty-five cardiac catheterisations were performed in Fontan patients during the study period. In 39 cases (46%), patients did not receive a volume load due to provider preference (n=19), baseline EDP ≥15 mm Hg or Fontan pressure ≥18 mm Hg (n=8), non-elective procedure type (n=8), evidence of clinical fluid overload (n=2) and severe ventricular systolic dysfunction (n=2). Protocolised volume loading was performed in the remaining 46 (54%) procedures, which formed the study cohort. There were no adverse events related to volume loading.
Baseline characteristics are demonstrated in table 1. Twenty-two (48%) of the patients were female. Median age of the cohort was 14.1 (IQR 9.1 to 21.3) years and mean weight 48.2±22.2 kg. The median duration of Fontan circulation was 10.8 (5.1 to 17.8) years. A dominant left ventricle was present in the majority (63%) of patients. Thirty-four (74%) of the patients were receiving ACE-inhibitor (ACE-I) therapy.
Baseline characteristics of the study cohort
Haemodynamics
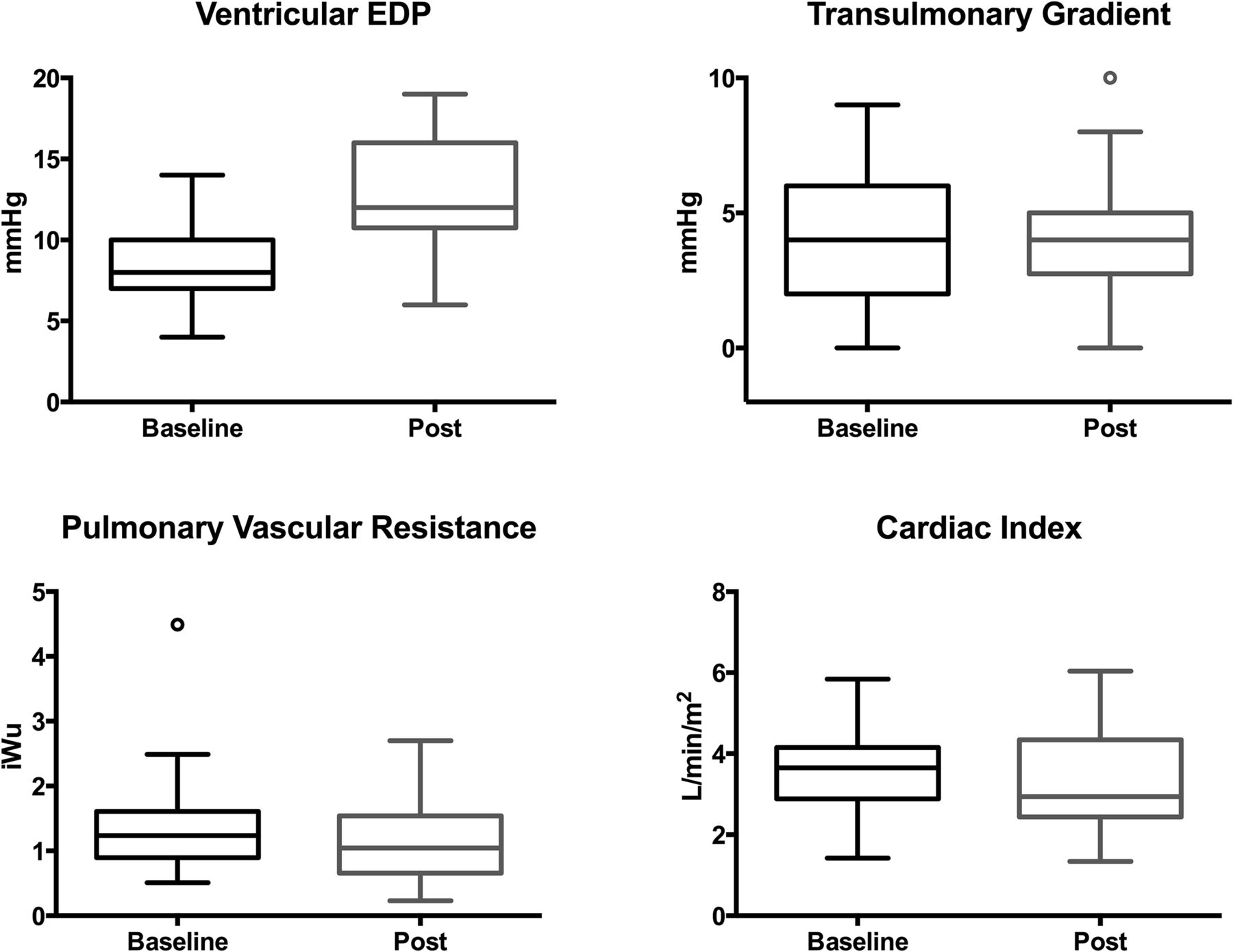
The changes in invasive haemodynamic measures obtained at baseline and following volume loading are summarised in table 2. Fluid administration resulted in a significant increase from baseline in mean Fontan pressure (15.2±2.5 vs 12.4±2.2 mm Hg, p<0.001), mean pulmonary capillary wedge pressure (11.3±2.6 vs 7.9±2 mm Hg, p<0.001) and ventricular EDP (12.7±3.3 vs 8.5±2.1 mm Hg, p<0.001). There were no significant changes in pulmonary vascular resistance (PVR), cardiac index or transpulmonary gradient (figure 1 and table 2). Sixteen patients (35%) were found to have occult DD (figure 2). Patients with occult DD had a higher baseline EDP (10.3±1.9 vs 7.6±1.5 mm Hg, p<0.001) and greater increase in EDP (6.3±2.4 vs 3.1±1.4 mm Hg, p<0.001) compared with patients without occult DD.
Changes in invasive hemodynamic data following ventricular stress testing

Box and whisker plots comparing baseline and post-volume loading measurements of ventricular end diastolic pressure, transpulmonary gradient, pulmonary vascular resistance and cardiac index. The median is displayed as a line within the box, the box defines IQR and the whiskers define the range. Open circles represent outliers.

{kind=link}
{kind=link}
Paired line graph of baseline and post-volume loading ventricular end diastolic pressures for each individual case. Trend lines are displayed for the subgroups with (dashed line) and without (dotted line) occult diastolic dysfunction (p<0.001 for difference in trends).
Factors associated with occult diastolic dysfunction
Results of logistic regression analysis to evaluate for factors associated with occult DD are presented in table 3. In both univariate and multivariable analysis, baseline EDP was the sole analysed factor found to be associated with occult DD. Patient age, ventricular morphology, duration of Fontan circulation and use of ACE-I therapy were not associated with occult DD when assessed as a dichotomous outcome.
Baseline factors associated with occult diastolic dysfunction
Factors associated with post-volume load EDP and absolute change in EDP, when evaluated as continuous variables, are displayed in tables 4 and 5. In univariate linear regression analysis, higher baseline EDP (p<0.001), longer duration of Fontan circulation (p=0.02) and lower baseline cardiac index (p=0.03) were all associated with higher post-fluid challenge EDP. Longer duration of Fontan circulation (p=0.04) but not baseline EDP or cardiac index was associated with greater absolute change in EDP. In multivariable analysis, only higher baseline EDP (p<0.001) remained a significant factor associated with higher post-fluid challenge EDP. No factors remained independently associated with greater absolute change in EDP.
Baseline factors associated with final EDP
Baseline factors associated with change in EDP
Discussion
Heart failure with preserved ejection fraction (HFpEF) is a well-recognised entity in non-congenital patients, affecting approximately half of all patients with congestive heart failure.21 While the term HFpEF is not used as standard terminology in the univentricular heart disease literature, these patients are frequently recognised to be clinically symptomatic with DD or ‘restrictive ventricular physiology’ as a contributing or primary aetiology. DD has long been proposed to contribute to failing Fontan physiology, both early and late following Fontan completion.16 ,22 However, in the absence of a highly sensitive and specific diagnostic test—or even a gold standard for the diagnosis—Fontan patients infrequently acquire this diagnosis and even more rarely receive targeted therapy.
In this large single-institution series of Fontan survivors undergoing invasive evaluation, 35% of patients had occult DD unmasked by a clinical protocol of ventricular stress testing using rapid volume expansion. It is important to note that this group of patients with occult DD is distinct from Fontan patients with overt DD, who were ineligible for participation in the clinical protocol, but would serve to further expand the population of Fontan survivors with ventricular DD.
While the routine use of rapid volume expansion during invasive assessment is novel in the Fontan population, it has long been employed in other populations for similar diagnostic purposes. The invasive ‘fluid challenge’ was first described in 1977, where it was used to facilitate the diagnosis of occult constrictive pericardial disease.18 More recently, the use of volume loading has been used to aid in distinguishing pulmonary venous hypertension from primary pulmonary arterial hypertension in patients with elevated pulmonary artery pressure.19 ,23 As with these prior studies, we have shown that volume loading can be a useful diagnostic tool for demonstrating occult abnormalities in ventricular diastolic function.
Our data may help in the understanding of late functional decline, and overt Fontan failure, that occurs in patients with Fontan physiology. Although 20-year freedom from mortality or cardiac transplantation in Fontan patients is now >80%, this still represents a significant burden of disease that may be modifiable.1 ,24 Furthermore, many survivors have symptomatic functional decline that increasingly manifests in early adult life. Consequently, the focus of care has shifted to identification and management of long-term Fontan-related morbidities, which are myriad.1 ,5 A key driver of chronic low cardiac output and poor cardiopulmonary health in Fontan patients is an inadequate stroke volume reserve.25 In the setting of normal systolic function, the primary determinants of stroke volume reserve are systemic venous return, PVR and diastolic function of the single ventricle. The adequacy of systemic venous return may also play a role, but is likely not the primary mechanism of circulatory limitation in most Fontan survivors.17 ,26 In the data presented herein, we did not find an increase in cardiac output following volume administration, supporting the assertion that adequate systemic venous return is not the primary limitation of Fontan cardiac output, at least in the resting state.
Dysfunction of the Fontan pulmonary vascular endothelium is demonstrable in a large proportion of patients and has been a target of pharmacological therapy.5 ,11–13 ,17 However, early studies of pulmonary vasodilator therapy in Fontan survivors have yielded mixed results to date.5 ,11–13 It is possible that future trials will demonstrate greater pharmacological benefit if patient recruitment were targeted to subjects with documented evidence of increased resting and/or exertional PVR (or transpulmonary gradient). However, our data add an additional note of caution: even in the presence of demonstrable pulmonary endothelial dysfunction, pulmonary vasodilation may be an unsuccessful pharmacologic strategy if there is coexisting occult DD. Under such circumstances, increasing the preload to the ventricle (much as is achieved by our protocol of rapid volume expansion described herein) may lead to increased EDP and generate a paradoxical increase in symptoms and reduction in functional capacity; much has been observed with the use of pulmonary vasodilators in the presence of structural left heart disease (eg, pulmonary veno-occlusive disease, mitral stenosis, restrictive cardiomyopathy). We suggest, therefore, that a comprehensive invasive evaluation of both pulmonary and ventricular haemodynamics may be necessary to adequately assess patient suitability prior to consideration of pulmonary vasodilator pharmacotherapy.
The acute reduction in ventricular preload that occurs following surgical conversion to Fontan circulation leads to an immediate increase in mass to volume ratio, with predominately early DD (incoordinate relation, reduced Tau and reduced early rapid filling) manifest acutely in the postoperative period.16 ,27 ,28 Although the mass to volume ratio normalises over time, impaired ventricular filling (DD) tends to persist in the long term.16 Based on a threshold EDP value of 15 mm Hg, 35% of the subjects in this cohort were found to have occult DD. Moreover, this subgroup demonstrated a significantly greater absolute increase in EDP after rapid volume expansion compared with those without occult diastolic disease, suggesting the group with occult DD demonstrated diminished ventricular compliance. The aetiology of this abnormality of single-ventricular compliance has not yet been demonstrated conclusively, although myocardial fibrosis may play an important role.29
Not unexpectedly, baseline ventricular EDP was associated with final EDP and the presence of occult DD. However, as demonstrated in figure 2, not all patients with borderline elevated baseline EDP demonstrated poor ventricular compliance with high post-fluid challenge EDP. That is to say, volume expansion served to distinguish two distinct populations of patients—those with normal to mildly elevated EDP and poor ventricular compliance and those with normal to mildly elevated EDP but normally compliant ventricles. Duration of Fontan circulation was also demonstrated to be modestly associated with post-volume load EDP and absolute change in EDP. It is possible that this reflects an era effect, related to the generally improved outcomes that we have observed in Fontan patients over time. However, our data are complimentary to previous longitudinal Doppler-echocardiographic assessment of systemic ventricular diastolic function showing changes compatible with worsening late diastolic compliance in the setting of persistently abnormal early diastolic function.16 This finding may suggest that chronic exposure to Fontan circulation is ‘additive’ with the long-term result being pathological ventricular relaxation with later worsening of ventricular compliance, possibly mediated through a fibrosis pathway.
The identification of a cohort of Fontan patients with occult DD is a necessary first step to improving long-term outcomes in this high-risk population. Future work will need to relate the presence of occult or overt DD to underlying phenotypic features of the endomyocardium, genotyping and clinical outcomes (eg, incidence of major adverse cardiovascular events (MACE)). Use of the fluid challenge as a stratification or ‘early identification’ tool, perhaps along with underlying phenotype and/or genotype, may allow for trials of targeted therapies to improve ventricular compliance and reduce the physiological implications of chronic DD. Moreover, should the occult DD subgroup be demonstrated to encounter a higher incidence of MACE in follow-up, this stratification tool might be used to identify patients who would potentially benefit from earlier evaluation for cardiac transplantation or other innovative support strategies.30
While our data are entirely novel, this proof-of-principle study has several important limitations. First, due to the study design (use of a clinical protocol with retrospective data collection), data collection was occasionally incomplete. Ascertainment of baseline medical characteristics was frequently limited in nature. Potentially relevant factors, such as cumulative lifetime cardiopulmonary bypass or circulatory arrest time, for example, were not collected or analysed, and concomitant echocardiographic or cardiac magnetic resonance functional and Doppler/flow data were not available in a large enough sample of the study cohort to facilitate an analysis of these clinically important data. Second, the assessment of ventricular diastolic function was limited to measurement of EDP using a fluid-filled catheter. Future investigations may provide additional insight into single-ventricular mechanics with the use of high-fidelity pressure sensors or conductance catheters. Third, in this study, we set a threshold EDP value of 15 mm Hg as the cut point for defining DD. While this value was based on prior investigations using volume loading in non-congenital populations, ultimately, a cut point for DD specific to the Fontan circulation will need to be determined based on the relationship between EDP and longer-term clinical outcomes. Lastly, this investigation did not include a concomitant assessment of anatomic phenotype (either by echocardiography or cardiac magnetic resonance) or clinical status, which might have allowed for confirmation of the clinical–pathological correlation with occult DD.
In conclusion, ventricular stress testing by rapid volume expansion is feasible, safe and identifies a subgroup of Fontan patients with occult DD. Higher baseline EDP and longer duration of Fontan circulation are associated with worse diastolic function. Future work is necessary to better understand the aetiology, associations and clinical implications of occult DD in Fontan survivors.
Key messages
What is already known on this subject?
It has been recognised that diastolic dysfunction can contribute to failing Fontan physiology. However, echocardiographic indices of diastolic function in the univentricular heart remain largely unvalidated and routine invasive haemodynamic studies are frequently unrevealing.
What might this study add?
The use of ‘ventricular stress testing’ with rapid volume expansion identifies an important subset of Fontan patients with diastolic dysfunction not manifest during baseline evaluation (so-called ‘occult diastolic dysfunction’). These patients demonstrated evidence of normal pulmonary vascular resistance (PVR).
How might this impact on clinical practice?
In current practice, medical interventions for the ‘failing Fontan’ patient focus largely on the pulmonary vasculature. The identification of a subset of Fontan patients with occult diastolic dysfunction and normal PVR suggests that targeted therapies for diastolic dysfunction may be more appropriate in many Fontan survivors.
References
Footnotes
Contributors KA: contributed to study design, data analysis and interpretation, manuscript development and gave final approval. Is responsible for overall content. RH, WW and RHB: contributed to data interpretation, critical manuscript revision and gave final approval. MDS: contributed to study design, data analysis and interpretation, critical manuscript revision and gave final approval. BHG: contributed to study conception and design, data analysis and interpretation, manuscript development and gave final approval. Is responsible for overall content.
Competing interests None declared.
Patient consent A waiver for informed consent was granted due to the retrospective nature of this study.
Ethics approval Institutional Review Board at Cincinnati Children's Hospital Medical Centre.
Provenance and peer review Not commissioned; externally peer reviewed.