Article Text

Abstract
Background Vasoreactivity testing is recommended in the management of pulmonary arterial hypertension (PAH), but its clinical relevance in congenital heart disease (CHD)-associated PAH has not been established.
Objective To determine whether residual pulmonary vascular responsiveness to intravenous. epoprostenol is predictive of clinical outcome in patients with CHD-PAH and Eisenmenger syndrome.
Methods and results A diagnostic right heart catheterisation with reversibility testing using epoprostenol infusion was performed in 38 consecutive patients with CHD-PAH and Eisenmenger syndrome. Patients were treated with bosentan and were assessed every 3 months. Clinical worsening was defined as death from any cause, heart–lung or lung transplantation (or on the waiting list for this procedure), hospitalisation for PAH, or symptom exacerbation defined as a ≥20% decrease in the 6 min walking distance on two consecutive tests, an increase in WHO functional class, or worsening right heart failure. The mean follow-up was 33±17 months. Sixteen patients showed clinical worsening. Although they did not differ from the other patients in their baseline exercise capacity, haemodynamic characteristics and underlying CHD, pulmonary vascular resistance index (PVRi) was less reversible (ΔPVRi 29±21 vs 52±14%, p=0.0003). At univariate analysis, systemic vascular resistance, PVRi and ΔPVRi were significant predictors of clinical worsening. At multivariate Cox proportional hazards regression model, ΔPVRi was found to be the only independent predictor of clinical worsening (HR=0.973, 95% CI 0.95 to 0.99; p=0.01). ΔPVRi ≥25% had a positive and negative predictive value for clinical worsening of 100% and 75.9%, respectively.
Conclusion Pulmonary vasoreactivity is a significant predictor of clinical worsening in patients with CHD-PAH.
- Pulmonary hypertension
- haemodynamics
- pulmonary arterial hypertension (PAH)
Statistics from Altmetric.com
Introduction
The diagnosis of pulmonary arterial hypertension (PAH) is based on a stepwise approach with confirmatory right heart catheterisation and reversibility testing.1 2 A marked decrease in pulmonary vascular resistance index (ΔPVRi) after acute administration of intravenous epoprostenol or inhaled nitric oxide (NO) has been shown to be associated with a better prognosis and response to calcium channel blocker treatment in patients with the idiopathic form of PAH.1–3 Whether this applies also to PAH with associated conditions or different types of severe pulmonary hypertension is less well established.1 2 Partial reversibility of chronic thromboembolic pulmonary hypertension after acute inhalation of NO has recently been shown to be associated with longer survival and freedom from lung transplantation in these patients.4 Reversibility of PVR by inhaled NO has been reported in a small group of patients with PAH related to congenital heart disease (CHD),5 and this was shown to be related to improved survival.6 Reversibility testing with oxygen and vasodilators is also an important step in the preoperative assessment of CHD with left-to-right shunt-induced pulmonary hypertension.7 8 However, the clinical relevance of PVR reversibility in CHD-PAH in patients with late-stage disease and Eisenmenger syndrome remains to be elucidated.8
The purpose of this study was to determine whether residual pulmonary vascular responsiveness to intravenous epoprostenol is predictive of clinical outcome in patients with CHD-PAH and Eisenmenger syndrome.
Methods and materials
Patient selection
Between January 2004 and June 2008, 40 consecutive patients referred to the Grown-Up Congenital Heart Disease Clinic of the Monaldi Hospital in Naples (Italy) for PAH owing to unoperated, non-restrictive intracardiac or extracardiac communication with a bidirectional or right-to-left shunt (Eisenmenger physiology) were enrolled. Fifteen patients had ventricular septal defect, eight atrioventricular canal, seven single ventricle, six atrial septal defect and two patent ductus arteriosus. Patients with anatomically small shunts and PAH (similar to patients with idiopathic PAH) were not included in the study. The diagnosis of PAH was established by a stepwise approach as recommended by expert consensus guidelines.1 2 The study protocol was approved by the institutional ethics committee and written informed consent was obtained from all patients before entering the study. Enrolled patients weighed >40 kg and were older than 16 years. No upper age limit was used. The patients had been in a stable condition for at least 3 months before study entry and were in WHO functional class II–IV. In addition, they had a systemic arterial oxygen saturation (SaO2) >60% at rest on room air and were not pregnant.
Study design
This was an open-label, single-centre, retrospective study.
Clinical evaluation and laboratory tests
Clinical evaluation included medical history, assessment of WHO functional class and measurement of systemic arterial pressure, oxygen saturation and heart rate. SaO2 was measured after 5 min of rest in the sitting position by pulse oximetry, and the mean of three consecutive readings was recorded for analysis. Clinical findings such as ankle oedema, jugular venous pulse and hepatomegaly were recorded.
Routine laboratory evaluation also included measurements of liver enzymes, in particular alanine aminotransferase and aspartate aminotransferase and 3-monthly measurements of haematocrit, haemoglobin and serum iron.
Exercise capacity
Exercise capacity was evaluated with a non-encouraged 6 min walk test.9 Patients who had never performed a 6 min walk test underwent an initial familiarisation session, as previously recommended.9 Heart rate and SaO2 were recorded at rest and after exercise. The Borg dyspnoea score was measured after completion of the test. The 6 min walk test was performed in a 25 m long corridor under the same environmental conditions and at approximately the same time of the day (±2 h).
Heart catheterisation
Assessment of haemodynamic parameters was performed by right heart catheterisation, as previously described.10 Pulmonary artery, right atrial and systemic arterial pressures were recorded at the end of a quiet respiratory cycle. SaO2 in the superior vena cava, inferior vena cava, pulmonary artery and femoral artery was measured in triplicate. Because no patients showed significant lung disease or scoliosis that could affect the pulmonary venous oxygen saturation, it was assumed to be 96%. Pulmonary (Qp) and systemic (Qs) blood flows were obtained with the Fick principle using table-derived oxygen consumption values and assuming an O2 consumption index of 125 ml/min/m2. Pulmonary and systemic vascular resistance indexes were calculated using the standard formula. All haemodynamic measurements were obtained under basal conditions and after vasoreactivity testing with intravenous epoprostenol.
Vasoreactivity test
Epoprostenol was administered intravenously at a starting dose of 2 ng/kg/min with 2 ng/kg/min increments every 10 min to a maximum dose of 12 ng/kg/min as tolerated, according to current guidelines.1 2
Treatment
Conventional treatment included oxygen, digoxin (n=18), diuretics (n=22), aldactone (n=18), warfarin (n=19) and enalapril (n=5). No patient received calcium channel blockers, nitrates or amiodarone. After diagnostic investigation with right heart catheterisation and reversibility testing, patients were treated with bosentan at a dose of 62.5 mg twice daily, increased to the target dose of 125 mg twice daily after 4 weeks.10
Clinical worsening
Clinical worsening was defined as the occurrence during follow-up of death, heart–lung or lung transplantation (or on the waiting list for this procedure), hospitalisation for PAH, addition of other PAH therapeutic agents, a ≥20% decrease in the 6 min walking distance on two consecutive tests, an increase in WHO functional class, or right heart failure.
Statistical analysis
The normal distribution of variables was checked using normal probability plots and the Shapiro–Wilk test. All variables are expressed as mean ± SD. Statistical analysis consisted of paired t tests to compare values at baseline and after epoprostenol infusion and unpaired t tests to compare subgroups. A Bonferroni adjustment for multiple comparisons was applied. Patient outcome was assessed using Kaplan–Meier event-free survival curves. The log-rank test was performed to evaluate differences in survival.11 12 A univariate Cox proportional hazard regression model was used to select potential predictors of clinical worsening. Multivariate Cox proportional hazard regression with backward elimination was used to identify independent predictors of clinical worsening. The 0.05 probability level was adopted to consider the significance of the association between predictive variables and events. The risk associated with each variable was expressed as a HR with 95% CIs. The best threshold values of PVRi changes were determined by receiver operating characteristic (ROC) curve analysis for ΔPVRi, to discriminate between patients who developed clinical worsening and those who did not. Sensitivity, specificity and positive and negative predictive values were calculated for the threshold value. A p value of <0.05 was considered statistically significant. Statistical analysis was performed using SPSS for Windows release 11.0.
Results
Two patients discontinued bosentan treatment after 1 and 5 weeks, respectively, because of refractory oedema and were not included in the analysis. In the remaining 38 patients, conventional treatment was maintained. alanine aminotransferase and aspartate aminotransferase plasma levels remained below three times the upper limit of normal in all but two patients. In both patients, the dose of bosentan was reduced to 62.5 mg three time a day, with complete normalisation of liver function tests.
All 38 patients were followed up until September 2009. Clinical outcome data were based on the most recently available medical records. No patient was lost to follow-up. Sixteen patients showed clinical worsening: two deaths (one sudden, one for untreatable heart failure), eight hospitalisations for PAH and addition of other PAH treatments after right heart catheterisation, two increases in WHO functional class and four decreases in the 6 min walking distance of ≥20% on two consecutive tests. The median time interval between right heart catheterisation and the occurrence of clinical worsening (time to clinical worsening) was 28±16 months. The mean follow-up was 33±17 months, with no difference between the patients who deteriorated and those who did not. Three patients died. The overall survival rate was 92%.
The characteristics of the 16 patients who showed clinical worsening and the 22 who did not worsen are reported in tables 1 and 2.
Demographic, clinical status and exercise capacity
Haemodynamic measurements at right heart catheterisation
The groups did not differ in gender distribution, age, body dimensions (body mass index), duration of follow-up, type of cardiac lesions, SaO2, heart rate, WHO functional class and 6 min walking distance, or in heart rate, SaO2 and Borg dyspnoea score after the 6 min walk test (table 1). There were no differences in haemodynamic parameters (table 2).
Haemodynamic measurements at baseline and after the maximum dose of epoprostenol are shown in table 3.
Acute effects of epoprostenol infusion
The dose of 12 ng/kg/min was given to all but two patients, in whom the infusion rate was limited to 10 and 8 ng/kg/min, respectively, because of a decrease in systemic blood pressure at higher doses. No other side effects were seen during epoprostenol infusion and the subsequent 24 h. The patients with no clinical worsening showed a higher epoprostenol-induced increase in Qp and a decrease in PVR (figure 1).
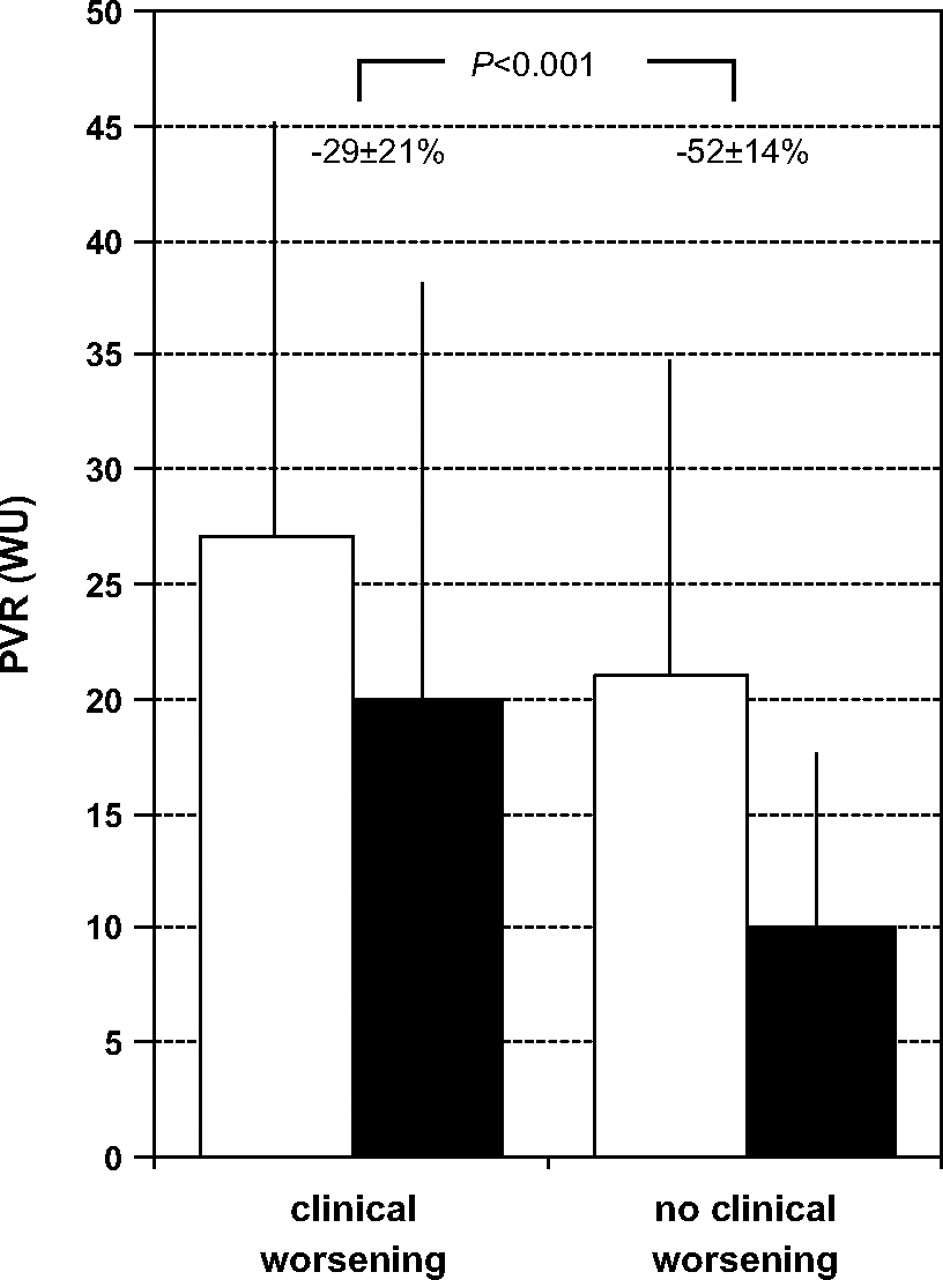
Pulmonary vascular resistance (PVR) before (white bars) and after (black bars) epoprostenol infusion in patients with or without clinical worsening at follow-up.
A ΔPVR of <25% after epoprostenol infusion was predictive of clinical worsening with a sensitivity and specificity of 56% and 100%, respectively (negative predictive value 75.9%, positive predictive value 100%). The area under the ROC curve was 0.773 (95% CI 0.608 to 0.892), indicating a good discrimination power (figure 2).
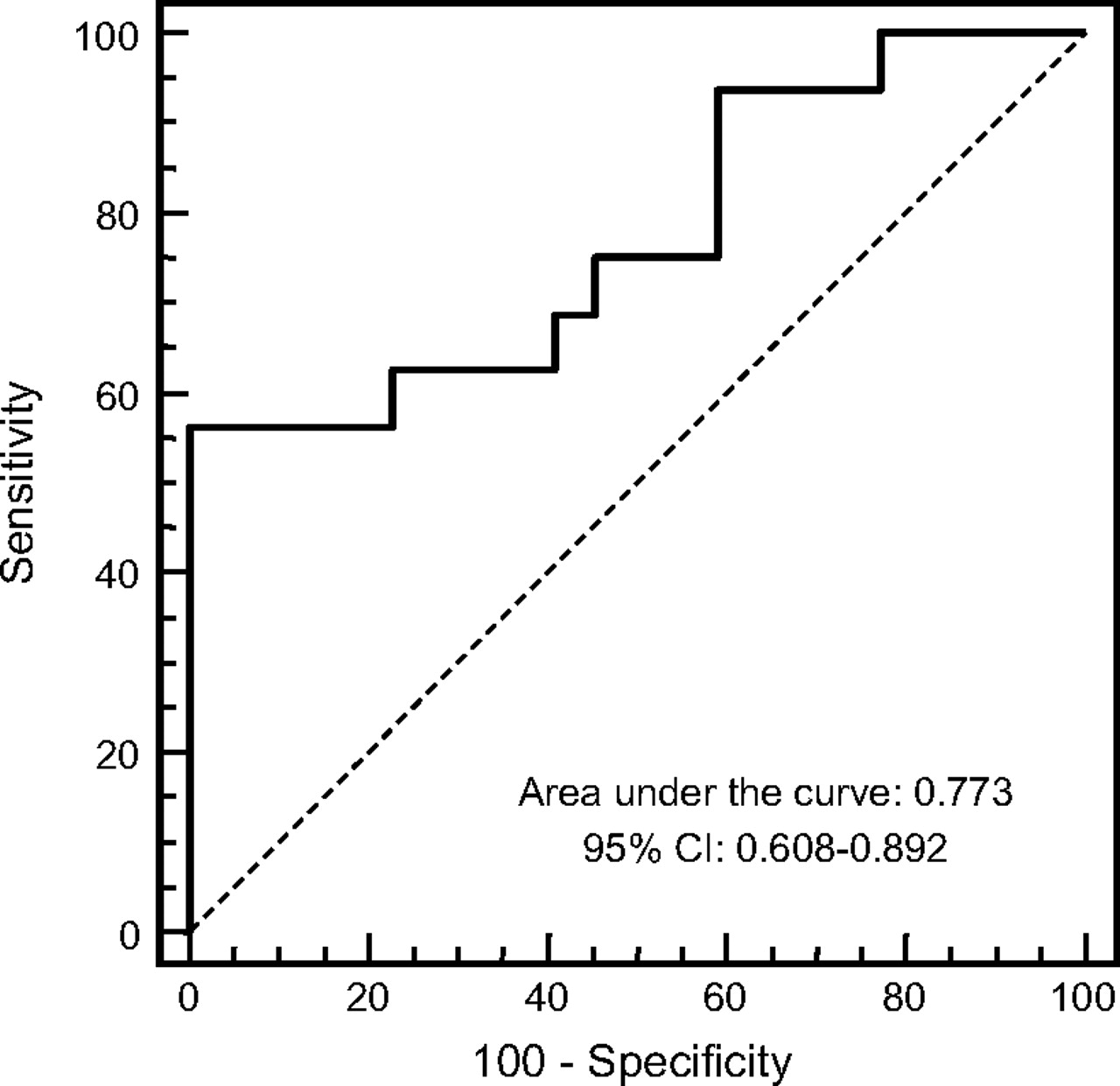
Receiver operating characteristic (ROC) curve that identifies a decrease in pulmonary vascular resistance index (ΔPVRi) of <25% after epoprostenol infusion as the threshold level with the best discriminating power for clinical worsening, with an area under the ROC curve of 0.773. A ΔPVRi of <25% after epoprostenol infusion was predictive of clinical worsening with a sensitivity and specificity of 56% and 100%, respectively (negative predictive value 75.9%, positive predictive value 100%).
Nine patients with ΔPVRi <25% showed clinical worsening (positive predictive value 100%) and 22/29 patients with ΔPVRi >25% did not worsen (negative predictive value 75.9%). The event-free survival curves were significantly different between these two subgroups (log-rank: p=0.0005; HR=0.196; 95% CI 0.072 to 0.528, p=0.0013) (figure 3A,B).

{kind=link}
{kind=link}
{kind=link}
Event-free survival curves in the overall study population (A) and in patients with a decrease in pulmonary vascular resistance index (ΔPVRi) of <25% (solid line) or ≥25% (dashed line) after vasoreactivity testing (B).
At univariate analysis using the Cox regression model, systemic vascular resistance index (HR=1.058; 95% CI 1.02 to 1.10; p=0.002), PVRi (HR=1.024; 95% CI 1.00 to 1.05; p=0.01) and ΔPVRi (HR=0.972; 95% CI 0.95 to 0.99; p=0.02) were predictive parameters of clinical worsening during vasoreactivity testing.
The only independent predictor of clinical worsening, as identified by multivariate Cox proportional hazard regression analysis, was ΔPVRi after vasoreactivity testing (HR=0.973; 95% CI 0.95 to 0.99; p=0.01).
Discussion
Our findings suggest that persistent pulmonary vasoreactivity in patients with Eisenmenger syndrome is relatively common and is associated with a favourable outcome.
In CHD with left-to-right shunt and increased PVR, vasodilator testing is usually performed to predict reversibility of pulmonary hypertension after corrective surgery.7 8 In these patients, acute reversibility of PVR is known to be associated with pulmonary arteriolar remodelling limited to medial hypertrophy, with no or minimal intimal proliferation.13 In patients with CHD-PAH and shunt reversal-induced Eisenmenger syndrome, it is generally assumed that extensive structural changes in the pulmonary resistive vessels may prevent the persistence of significant vasoreactivity.1 2 7 8 13 14
Reversibility testing in PAH with inhaled NO, intravenous adenosine or prostacyclin is recommended to identify patients with marked reversibility of PVR who may benefit from chronic calcium channel blocker therapy.1–3 The clinical relevance of this approach, however, has been established only in idiopathic PAH.3 Calcium channel blockers are not indicated in CHD-PAH because of their negative inotropic and systemic vasodilator effects.7 8 This accounts for the limited interest in reversibility testing in patients with Eisenmenger syndrome.
In earlier studies, Wood had observed reversibility with acetylcholine in idiopathic PAH and mitral stenosis but not in CHD-PAH.15 However, the administration of vasodilators such as tolazoline was later proved to decrease PVR in patients with CHD-PAH.16 A ΔPVR of >20% was documented in four of 22 patients after 20 ppm inhaled NO and in six of 21 patients after 80 ppm inhaled NO in a heterogeneous population with CHD-PAH, including patients with Eisenmenger syndrome.5 Interestingly, a reduced reactivity was seen in the presence of right-to-left shunting.5 In a subsequent study from the same centre, an NO-induced ΔPVR of >20% was seen in 10 of 21 patients with CHD-PAH either undergoing surgical correction or affected by Eisenmenger syndrome (n=10). In this subset of patients, vasoreactivity was associated with improved outcome.6
The use of epoprostenol has some theoretical and safety concerns in patients with Eisenmenger syndrome because in the presence of a right-to-left shunt epoprostenol may have a larger effect on systemic than on pulmonary circulation. However, because the majority of patients with Eisenmenger syndrome have a bidirectional shunt and epoprostenol acts widely on pulmonary circulation it is not surprising that the epoprostenol response is qualitatively similar to NO.5 6 This study on a larger population of patients with Eisenmenger syndrome suggests that persistent pulmonary vasoreactivity is common and predicts a better outcome.
Patients with CHD-PAH and Eisenmenger syndrome show marked functional impairment and reduced exercise capacity,17 although survival is much longer than in patients with PAH and other associated conditions.18 This is probably owing to the persistence of fetal features of hypertrophy, which allow the right ventricle to compensate for chronically increased after load and to right-to-left shunting, which reduces right heart chamber enlargement.8 18 Owing to long-term clinical stability, preserved right ventricular function, advanced structural changes in the pulmonary circulation and the risk of potential life-threatening side effects (eg, a fall in systemic blood pressure or oxygenation), it has long been assumed that these patients may not benefit from targeted pulmonary vasodilator therapy.8 Notwithstanding this, results from several open-label studies are encouraging.8 10 In addition, a randomised controlled trial of bosentan in patients with CHD-PAH and Eisenmenger syndrome has shown that, after a few months of treatment, clinical improvement is more likely to occur in other PAH categories.19 Furthermore, evidence from the open-label extension of this study suggests long-term persistence of these beneficial effects.20 On this basis, patients with CHD-PAH and Eisenmenger syndrome are treated with bosentan at our centre. Accordingly, it remains to be clarified whether the prognostic value of reversibility testing in patients with CHD-PAH and Eisenmenger syndrome, as reported in this study, reflects an intrinsic characteristic of the disease and/or a therapeutic effect.
Our study has limitations. The design was open label, retrospective, non-randomised and monocentric.
Patients with CHD-PAH are by definition a heterogeneous population, but unlike in other studies, we considered only patients with non-restrictive unoperated shunts.
At right heart catheterisation we assumed that the pulmonary vein saturation was 96%. In the absence of an atrial septal defect we did not directly measure it with trans-septal puncture because of an ethical concern. Although this is standard in current clinical practice, it is probably a limitation in a pharmacological test looking for acute changes.
Finally, the cut-off point of 25% for ΔPVR was not prespecified and thus might seem arbitrary. However, the number resulted from a rigorous ROC curve analysis and as such is probably worth consideration in further prospective studies on the clinical relevance of persistent pulmonary vasoreactivity of patients with CHD-PAH and Eisenmenger syndrome.
Acknowledgments
We thank all the nurses of the Division of Adult Cardiology and GUCH Unit of Monaldi Hospital, for their technical support and cooperation in the outpatient clinic and in the catheter laboratory—particularly, Mrs Assunta Carandente, Mrs Antonella Nannolo, Mrs Assunta Di Vaio, Mrs Deborah De Santis, Mrs Ada Orefice, Mrs Patrizia Sannino, Mrs Marina Battista, Mr Pasquale Canzanella, Mr Domenico Puzone, Mr Gianfranco Paliotti and Mrs Gabriella Lettieri.
References
Footnotes
Competing interests None.
Patient consent Obtained.
Ethics approval This study was conducted with the approval of the Ospedale Monaldi, Naples.
Provenance and peer review Not commissioned; externally peer reviewed.