Article Text

Abstract
Context: Resistance training may be beneficial for patients with chronic heart failure (CHF).
Objective: To systematically review the methodological quality of, and summarise the effects of, moderate-to-high intensity resistance training in CHF.
Data sources: Medline/PubMed, Science Citation Index Expanded, SSCI and A&HCI.
Study selection: English language (non-)randomised controlled trials.
Data extraction: A predesigned data extraction form was used to obtain data on trial design and relevant results. Methodological quality of the identified trials were scored using the Delphi list.
Results: Most of the 10 trials identified had moderate-to-severe methodological limitations. Effects of resistance training (alone or in combination with endurance training) are inconclusive for outcomes like exercise capacity and disease-specific quality of life.
Conclusions: Even though moderate-to-high intensity resistance training does not seem be harmful for patients with CHF, the current peer-reviewed evidence seems inadequate to generally recommend incorporation of resistance training into exercise-based rehabilitation programmes for patients with CHF.
Statistics from Altmetric.com
Patients with moderate-to-severe chronic heart failure (CHF) have been shown to have a significantly lower daily physical activity level than healthy peers owing to daily symptoms of breathlessness or fatigue, or both.1 This may, at least in part, explain the presence of fat-free mass depletion and skeletal muscle weakness in CHF,2,3,4,5 which, in turn, has been shown to be related to an impaired peak aerobic capacity (Vo2).4,6,7,8,9,10,11 Additionally, patients with CHF with explicit reductions in skeletal muscle force and peak Vo2 have been shown to have a higher use of healthcare resources12 and a higher mortality rate than patients with CHF with relatively well-preserved outcomes of physical fitness.13,14,15,16 Therefore, exercise-based rehabilitation has become an important part in the integrated management of patients with clinically stable CHF.17,18
Supervised moderate-to-high intensity resistance training has been shown to be a highly specific training modality to enhance skeletal muscle mass and function, functional capacity and independence and quality of life (QoL).19 Indeed, the metabolic response and symptom perception during moderate-to-high intensity resistance training appear to be acceptable for patients with chronic organ failure.20,21 Therefore, moderate-to-high intensity resistance training may be a valuable training modality to counteract skeletal muscle weakness, wasting and morphological changes in patients with CHF,22 without an undesirable haemodynamic response of the impaired cardiovascular system.23,24
In 2001, the European Society of Cardiology recommended applying endurance training during CHF rehabilitation to improve peak Vo2 and health status.25 Meanwhile, the European Society of Cardiology has concluded that experience with resistance training in CHF is limited and more experience in larger patient populations is necessary before a general recommendation can be given.25 Recently, the American Heart Association stated that supervised resistance training can be incorporated safely into rehabilitation programmes for patients with CHF, although further study of this important area is needed.19
To date, only (critical) narrative reviews of the effects of resistance training in CHF have been published, mostly concluding that appropriate dynamic resistance exercise should be recommended as an effective alternative or supplementary training mode in order to improve skeletal muscle strength in CHF.22,26,27,28,29 Nevertheless, narrative reviews often provide insufficient insight or attention to detail, which, in turn, may result in erroneous recommendations.30 Surprisingly, a peer-reviewed systematic review on the effects of moderate-to-high intensity resistance training (alone or in combination with endurance training) in patients with CHF has not been previously performed.
This paper is a systematic review of the assumed positive effects of supervised moderate-to-high intensity resistance training (alone or in combination with endurance training) in patients with CHF as well as a critical appraisal of the literature. Additionally, we examined the reviewed trials for insight into the safety of the reported training modalities and evaluated them for methodological quality.
Methods
All details of the methods used are given in the online appendix.
Results
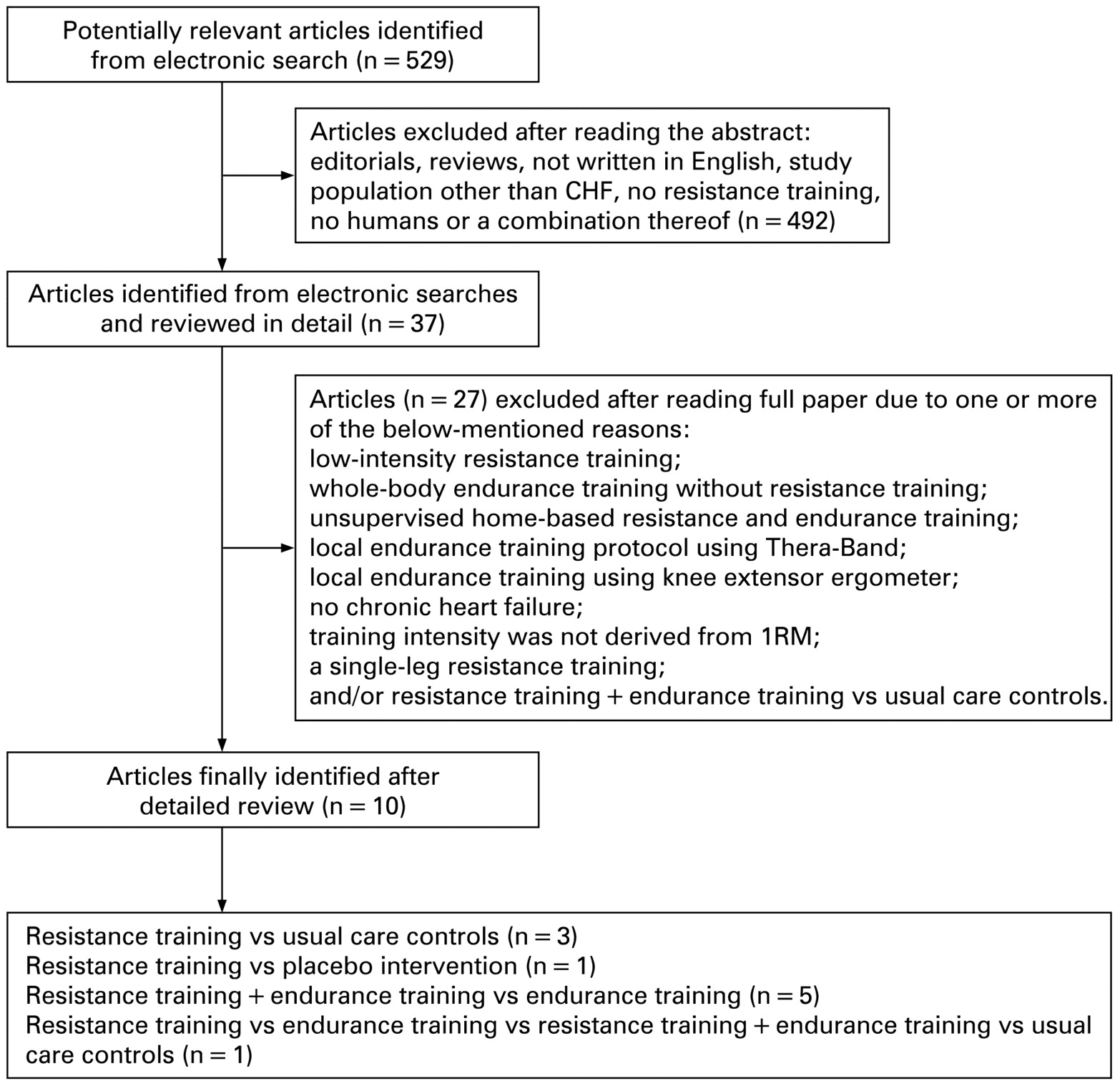
In total, 529 articles were found from the electronic searches. Of these articles, 37 were considered eligible after abstracts had been read and reviewed in detail. Twenty-seven trials31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57 were excluded for one or more of the following reasons: pooled data from multiple studies; low-intensity resistance training; whole-body endurance training without resistance training; unsupervised home-based resistance and endurance training; local endurance training protocol using Thera-Band; local endurance training using knee extensor ergometer; no CHF; training intensity was not derived from one-repetition maximum (1RM); resistance in combination with endurance training versus usual care controls and/or a single-leg resistance training. No trials were selected from reference lists of the remaining articles. Finally, 10 trials studying the effects of moderate-to-high intensity resistance training (alone or in combination with endurance training) were considered eligible58,59,60,61,62,63,64,65,66,67 (fig 1).

{kind=link}
Summary of trials studying the effects of moderate-to-high intensity resistance training (alone or in combination with endurance training). CHF, chronic heart failure; 1RM, one-repetition maximum.
Methodological quality
None of the 10 identified trials had a perfect score ( = 9 × “yes”) on the Delphi list. Pu and colleagues67 had the highest score (8 × “yes”), while four trials (40%) scored ⩽3 × “yes”.61,63,65,66 Consequently, the mean (standard deviation) score of the identified trials of the Delphi list was poor: 4.3 (1.7) points (table 1).
Methodological quality of trial designs
Safety monitoring and drop out
Only one trial defined safety/adverse events (defined as “all-cause mortality and non-elective cardiac-related hospital admission”) as a secondary outcome measure.59 Indeed, drug treatment remained unchanged during the trial; no adverse events were reported; and owing to permanent telemetry, major arrhythmic disturbances were excluded. Beckers and colleagues did report the dropout of two patients (7.1%) owing to lymphoma and ischialgia during combined resistance and endurance training, while no dropout was reported in the endurance training group.59
The remaining nine identified trials did not define safety as a primary or secondary outcome. Nevertheless, serious adverse events and/or minimal changes in cardiac drug treatment were reported to be rare.58,63,65,66,67 Five trials (50%) reported anecdotal serious adverse events: a period of severe hypotension in one patient with CHF, requiring a 2-day hospital admission62; withdrawal due to worsening of CHF (n = 1) or because unable to make the time commitment for the study (n = 2)61; and one patient with CHF was reported to drop out owing to hospitalisation for an episode of rapid rate atrial fibrillation.60 These patients with CHF, however, had all been allocated to the endurance-training group, which did not undergo resistance training. To date, only Cider and colleagues have reported the drop out of one patient with CHF of the resistance training group owing to a severe asthma attack requiring hospitalisation.64 Finally, Feiereisen and colleagues reported 1 week of rest in one patient allocated to resistance training owing to low-back pain that could not be directly related to the intervention.58
Patients were supervised during the resistance training programme by a cardiologist, physiotherapist, physical coach, exercise physiologist, registered nurse, “a research assistant” (without further specifications of their background) or a combination thereof.59,60,61,62,63,67 In addition, several trials included a central monitoring system permitting arrhythmia detection during resistance training and/or endurance training59,60,61,62,63; and before the start or at the end of every training session the individual pulse rate and/or blood pressure were assessed.60,61,62,64 None of these trials reported exercise-induced malignant ventricular arrhythmia during resistance training. Finally, six trials (60%) included a warm-up period (consisting of short-lasting, low-intensity walking or cycling, light calisthenics and/or stretching) and/or a cooling down period (consisting of some stretching).58,59,64,65,66,67
Description of actual resistance training programme
Seven trials (70%) reported a mean compliance rate of between 75 and 100%.58,61,62,64,67 Finally, Beckers and colleagues only reported that adherence and compliance were “excellent”.59
Surprisingly, none of the 10 identified trials provided detailed information about the actual training load during progressive moderate-to-high intensity resistance training in CHF. Only Pu and colleagues reported the mean training load during a 10-week resistance training programme (eg, 82% of the most recent 1RM, which was retested every tenth resistance training session). Moreover, these authors did report that four patients with CHF (44.4%) required minor modifications in their resistance regimen because of intermittent mild musculoskeletal symptoms.67
Effects of resistance training
Resistance training does not appear to affect left ventricular contractile function or enhance myocardial deterioration compared with usual care or low-intensity stretching (tables 2 and 3).
Effects of resistance training in chronic heart failure
Summary of effects of resistance training (alone or in combination with endurance training)
There were conflicting results on the mean changes in peripheral muscle strength and endurance, submaximal exercise capacity, peak Vo2 and disease-specific QoL after resistance training compared with usual care controls, while the effects on New York Heart Association (NYHA) classification and body composition have never been studied (tables 2 and 3).
The only randomised placebo-controlled trial did show significant improvement in strength, endurance, and functional exercise capacity following a 10-week resistance training programme compared with a 10-week low-intensity stretching programme.67 However, body composition, vastus lateralis muscle enzyme activity and peak exercise capacity were not significantly different between the two groups. Moreover, effects of resistance training on cardiac function, NYHA classification, disease-specific QoL, body composition, peripheral muscle strength and peak Vo2 seem to be similar to endurance training (alone or in combination with resistance training).58
Effects of resistance training in combination with endurance training
Resistance training in combination with endurance training does not appear to affect left ventricular contractile function or enhance myocardial deterioration compared with endurance training (tables 3 and 4).
Effects resistance training in combination with endurance training in CHF
Resistance training in combination with endurance training does appear to improve peripheral muscle strength compared with endurance training. Mean changes in NYHA classification, body composition, peripheral muscle endurance and peak VO2 were similar (tables 3 and 4). Effects on 6 min walking distance and treadmill endurance time have never been studied.
Discussion
Moderate-to-high intensity resistance training has been shown to be a valuable exercise modality in healthy subjects and in patients with (complex) chronic organ failure.19,68,69 Indeed, resistance training should be routinely incorporated in respiratory rehabilitation.70 Based on the striking similarities in systemic factors contributing to exercise intolerance in patients with chronic obstructive pulmonary disease and CHF,4 we reasoned that it might be worthwhile to add moderate-to-high intensity resistance training to exercise-based cardiac rehabilitation programmes.
Even though resistance training at moderate-to-high intensity appears to be safe, its effects in patients with CHF are inconclusive. Indeed, this systematic review of the peer-reviewed English literature identified only one randomised placebo-controlled trial assessing the effects of moderate-to-high intensity resistance training in patients with stable CHF.67 Additionally, moderate-to-high intensity resistance training does not appear to augment the positive effects of aerobic training in CHF, except for peripheral muscle strength. Finally, the methodological quality of the identified trials is generally poor, which limits the validity of most findings.
Methodological considerations
Internal and external validity
None of the 10 identified trials had a perfect score on the Delphi list (table 1). These methodological shortcomings may seriously diminish the internal validity of the reviewed trials.71,72,73 Moreover, we feel it is safe to conclude that the external validity of the reviewed trials is rather limited. Indeed, when it was reported, all trials were performed in a secondary or tertiary care outpatient setting; 72.7% of the patients were men; 60.0% of the patients had an ischaemic aetiology of their disease; and mean left ventricular ejection fraction was 27.9%. Moreover, patients with CHF with coexisting morbidities, like diabetes, intermittent claudication, chronic lung disease, status after stroke, orthopaedic problems, current smokers, pulmonary hypertension, renal impairment, hypercholesterolaemia, arterial hypertension, actively listed on the transplant list or a combination thereof, were mostly ineligible to enrol.58,59,60,64,65,66 Then again, the only randomised placebo-controlled trial comparing progressive resistance training with a low-intensity stretching programme did include patients with CHF with coexisting morbidities, like arthritis, arterial hypertension, coronary artery disease, diabetes and osteoporosis.67 Unfortunately, Pu and colleagues enrolled only older (⩾65 years) community-dwelling female patients with CHF without specification of current cardiac drug treatment.67
Interpretation of current literature
On average, the effects of moderate-to-high intensity resistance training on peak Vo2 and disease-specific QoL in patients with CHF seem inconclusive. At first sight, this may be somewhat surprising, in particular because of the cross-sectional positive relationship between skeletal muscle function and peak Vo2 in CHF.4,6,7,8,9,10,11 Nevertheless, in light of the various methodological shortcomings it is rather difficult to speculate whether or not the lack of improvement in peak Vo2 and disease-specific QoL is due to problems with study design or truly reflects the lack of a causal relationship. Then again, Feiereisen and colleagues did not find significant correlations between changes in peak Vo2, LVEF and skeletal muscle strength after resistance training, endurance training or a combination thereof in CHF.58
Surprisingly, in this systematic review, only four trials (40%) reported a hypothesis,59,61,64,67 while only two trials (20%) clearly stated their primary outcome(s).59,67 This, together with the lack of statistical comparisons for one or more (baseline) outcome(s) between the experimental group and the control group60,61 makes the process of scientific inference about the effects of resistance training (alone or in combination with endurance training) in patients with CHF less consistent and unclear. Additionally, sometimes interpretations of the results do not seem entirely consistent with the reported results59,61,62,67 (see online appendix for details). Finally, differences in baseline peak Vo2, differences in the duration and intensity of the intervention(s) and the diversity in exercise outcomes may also partially explain conflicting results between the identified trials (tables 2 and 4).
Safety
Although safety has never been set as a primary outcome, our systematic review does not provide evidence that resistance training at an intensity of 50–80% of the 1RM is hazardous for patients with clinically stable CHF. In fact, the drop-out rates were rather low and serious adverse events related to the intervention appear absent. This may be due to careful screening at baseline and/or during follow up, together with the supervised setting. Moreover, resistance training does not appear to cause a reduction of the left ventricular contractility function or to enhance myocardial deterioration in patients with CHF.
Clinicians who consider resistance training in patients with CHF do have to take into account the above-mentioned methodological limitations. None of the identified trials included patients with CHF with unstable angina pectoris, complex ventricular arrhythmias, uncontrolled atrial fibrillation and/or pulmonary hypertension; and only one trial reported the enrolment of a patient with CHF with an internal cardioverter-defibrillator, without reporting group allocation.62 Finally, endurance training has been shown to partially reverse left ventricular remodelling in patients with clinically stable CHF. This benefit was not confirmed with combined resistance and endurance training.74 It may therefore be premature to generally add resistance training to endurance training in CHF rehabilitation.
Recommendations
It seems appropriate to design new randomised controlled trials to quantify the effects of moderate-to-high intensity resistance training in CHF. These randomised controlled trials have to include a larger and more heterogeneous sample of clinically stable patients with CHF with short-term and long-term follow-up. It may even be worthwhile assessing the effects of a multidisciplinary approach, in which cardiologist and physiotherapist collaborate closely with specialised nurses, psychosocial counsellors, occupational therapists and dieticians.
Left ventricular remodelling,74 submaximal exercise parameters, skeletal muscle endurance and patient-centred outcomes, like daily physical activity level using validated accelerometers may be of clinical relevance75 and, in turn, should be considered as possible future primary or secondary outcomes.
Finally, authors have to report more carefully the safety of resistance training as well as the actual training load over time of individual patients with CHF to make a continuous evaluation and evolution of these programmes possible. Future studies should also consider moderate-to-high intensity single-leg resistance training49 and be more specific about patient selection. Indeed, resistance training may be of particular interest in disabled patients with CHF and skeletal muscle atrophy or weakness, or both.2,4
Conclusions
We believe that there is a clear rationale for studying the effects of moderate-to-high intensity resistance training in clinically stable patients with moderate-to-severe CHF. Nevertheless, the current peer-reviewed literature does not provide good evidence that moderate-to-high intensity resistance training has statistically significant and clinically relevant positive effects on important outcome measures, such as peak Vo2, skeletal muscle endurance, submaximal exercise capacity and disease-specific QoL. On the contrary, most of the included trials had substantial methodological limitations. Consequently, our current understanding of the effects of moderate-to-high intensity resistance training in CHF is limited. Even though moderate-to-high intensity resistance training does not seem be harmful for patients with CHF, the current peer-reviewed evidence is inadequate to generally recommend its incorporation into exercise-based rehabilitation programmes for these patients.
Acknowledgments
We are grateful to the following authors for providing additional information about their trial(s): Drs Itamar Levinger, Jukka Kemppainen, Andrew Maiorana, Andrew Williams, Steve Selig, Francis Degache, Eckart Miche, Åsa Cider, Maria Singh, Paul Beckers, Charles Delagardelle and Patrick Feiereisen. We acknowledge Dr Scott S Wagers for his assistance in editing the manuscript.
REFERENCES
Supplementary materials
Web only appendix 95;17:1399
Files in this Data Supplement:
Footnotes
Competing interests None.