Article Text

Abstract
Objectives To compare hospitalisation rates, intensive care unit (ICU) admissions and mortality for patients with COVID-19 who were consistently inactive, doing some activity or consistently meeting physical activity guidelines.
Methods We identified 48 440 adult patients with a COVID-19 diagnosis from 1 January 2020 to 21 October 2020, with at least three exercise vital sign measurements from 19 March 2018 to 18 March 2020. We linked each patient’s self-reported physical activity category (consistently inactive=0–10 min/week, some activity=11–149 min/week, consistently meeting guidelines=150+ min/week) to the risk of hospitalisation, ICU admission and death after COVID-19 diagnosis. We conducted multivariable logistic regression controlling for demographics and known risk factors to assess whether inactivity was associated with COVID-19 outcomes.
Results Patients with COVID-19 who were consistently inactive had a greater risk of hospitalisation (OR 2.26; 95% CI 1.81 to 2.83), admission to the ICU (OR 1.73; 95% CI 1.18 to 2.55) and death (OR 2.49; 95% CI 1.33 to 4.67) due to COVID-19 than patients who were consistently meeting physical activity guidelines. Patients who were consistently inactive also had a greater risk of hospitalisation (OR 1.20; 95% CI 1.10 to 1.32), admission to the ICU (OR 1.10; 95% CI 0.93 to 1.29) and death (OR 1.32; 95% CI 1.09 to 1.60) due to COVID-19 than patients who were doing some physical activity.
Conclusions Consistently meeting physical activity guidelines was strongly associated with a reduced risk for severe COVID-19 outcomes among infected adults. We recommend efforts to promote physical activity be prioritised by public health agencies and incorporated into routine medical care.
- COVID-19
- physical activity
- exercise
Data availability statement
No data are available.
This article is made freely available for use in accordance with BMJ’s website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
https://bmj.com/coronavirus/usageStatistics from Altmetric.com
Introduction
The US Centers for Disease Control and Prevention (CDC) has identified risk factors for severe COVID-19, including advanced age, sex (male) and the presence of underlying comorbidities, such as diabetes, obesity and cardiovascular disease.1 However, there are no data regarding the effect of regular physical activity (PA) on COVID-19 outcomes, even though a lack of PA is a well-documented underlying risk factor for multiple chronic diseases, including those associated with severe COVID-19.1 2
The US Physical Activity Guidelines call for all adults to engage in at least 150 min/week of moderate to vigorous physical activity (MVPA).3 Similar guidelines have been promoted in many countries based on strong evidence that regular PA results in a broad range of health benefits.4–6 It is reasonable to expect regular PA may mitigate poor COVID-19 outcomes. It is well known that immune function improves with regular PA, and those who are regularly active have a lower incidence, intensity of symptoms and mortality from various viral infections.7–9 Regular PA reduces the risk of systemic inflammation, which is a main contributor to lung damage caused by COVID-19.10 Additionally, exercise benefits cardiovascular health, increases lung capacity and muscle strength, and improves mental health.3 11 These are mechanisms by which regular PA could play an important role in mitigating the severity of the COVID-19 pandemic, in addition to its beneficial effects on multiple chronic diseases.
During the pandemic, populations across the globe have been advised to stay home and avoid contact with individuals outside of one’s household. Lockdowns and other measures that constrain travel have restricted access to gyms, parks and other venues where people can be active.12 In the USA, education about the benefits of PA and advice to maintain or increase PA during the pandemic has been essentially absent. While prepandemic levels of PA were generally insufficient,13 pandemic control measures have likely had the unintended consequence of reducing PA even more. Indeed, early studies indicated a significant reduction in PA levels since the beginning of the pandemic.14–16
In this study, we used an electronic health record (EHR) that captured self-reported PA behaviours prior to the pandemic to evaluate the hypothesis that consistently meeting guidelines prior to diagnosis is associated with more favourable COVID-19 outcomes among infected adults. If regular PA is shown to be a protective behaviour for COVID-19, efforts should be made to enable and encourage regular PA as a means of protecting individuals from severe COVID-19 outcomes.
Methods
Study design
This is a retrospective observational study in which PA was documented in the EHR in the 2 years preceding the March 2020 pandemic lockdown.
Setting
This study was conducted at Kaiser Permanente Southern California (KPSC), which is an integrated healthcare system that serves approximately 4.7 million residents in Southern California at 15 medical centres. Racial/ethnic make-up, neighbourhood education and household income are generally similar to the area population.17 KPSC uses a comprehensive EHR that links all laboratory results, healthcare visits and diagnoses in both inpatient and outpatient settings and even outside the system.
Study cohort
Inclusion criteria consisted of KPSC health plan members aged 18 years and older with a positive COVID-19 test or diagnosis between 1 January 2020 and 21 October 2020. Participants were continuously enrolled at KPSC for at least 6 months prior to their COVID-19 diagnosis. We required patients to have at least three outpatient visits with an exercise vital sign (EVS) measure between 19 March 2018 and 19 March 2020 to increase the likelihood that the assessment captured regular PA habits.
Exercise vital sign
The EVS is used at every outpatient encounter within the KPSC system since 2009 and has been described elsewhere.18 Briefly, trained medical assistants or nurses ask patients two questions about their typical exercise habits over the previous 2 months or more during the intake at each outpatient visit: ‘On average, how many days per week do you engage in moderate to strenuous exercise (like a brisk walk)?’ and ‘On average, how many minutes do you engage in exercise at this level?’. Response choices for days are 0–7, and minutes are recorded as 0, 10, 20, 30, 40, 50, 60, 90, 120 and 150 or greater. The responses are recorded in each patient’s EHR and minutes per week of MVPA are calculated. The EVS has been shown to have good face and discriminant validity.18 19
Three categories of PA were created for this study based on the US Physical Activity Guidelines3: consistently meeting guidelines (EVS >150 min/week at all assessments during the study period), consistently inactive (EVS 0–10 min/week at all assessments) and some activity (EVS 11–149 min/week or those with variability in their EVS measures).
Data analysis
The primary outcomes examined were hospitalisation, admission to the intensive care unit (ICU) and death due to COVID-19. Patient demographics, utilisation, clinical characteristics and comorbidities among different PA groups were compared using χ² test for categorical variables, exact test for categorical variables with a count <5 (none of the cell expected values were less than 1 and fewer than 20% of the cell expected values were less than 5) and the Kruskal-Wallis test for continuous variables. Covariates included age, sex and race, along with underlying medical conditions associated with increased risk for severe illness from COVID-19 as defined by the CDC.2 These underlying conditions included a history of cancer (primary and metastatic), chronic kidney disease, chronic obstructive pulmonary disease, cardiovascular disease (including myocardial infarction, congestive heart failure, peripheral vascular disease and cerebrovascular disease), history of organ transplant, obesity (body mass index (BMI) 30–39 kg/m2) and class 3 obesity (BMI ≥40 kg/m2), pregnancy, current smoking status and diabetes. In addition, we included history of hypertension and an emergency department visit or hospitalisation in the 6 months prior to COVID-19 diagnosis as covariates. We conducted logistic regressions to estimate the ORs (and 95% CIs) for the association of these factors with the EVS categories, with separate models for each of the outcomes. Data were analysed using SAS (V.9.4 for Windows; SAS Institute)
Patient and public involvement
Patients and the public were not involved in the design or conduct of this study.
Results
We identified 103 337 patients with a diagnosis of COVID-19 or positive result on PCR testing during the study period. Of these, 84 377 were 18 years or older and continuously enrolled in the KPSC health plan during the 6 months prior to their COVID-19 diagnosis. Among these, 48 440 patients had three or more EVS measurements within the 2 years prior to the California pandemic lockdown on 18 March 2020, which comprised the analytical cohort for this study (see figure 1). The majority of patients (61.2%) in our cohort had five or more EVS measures in that 2-year time frame (see online supplemental table).
Supplemental material
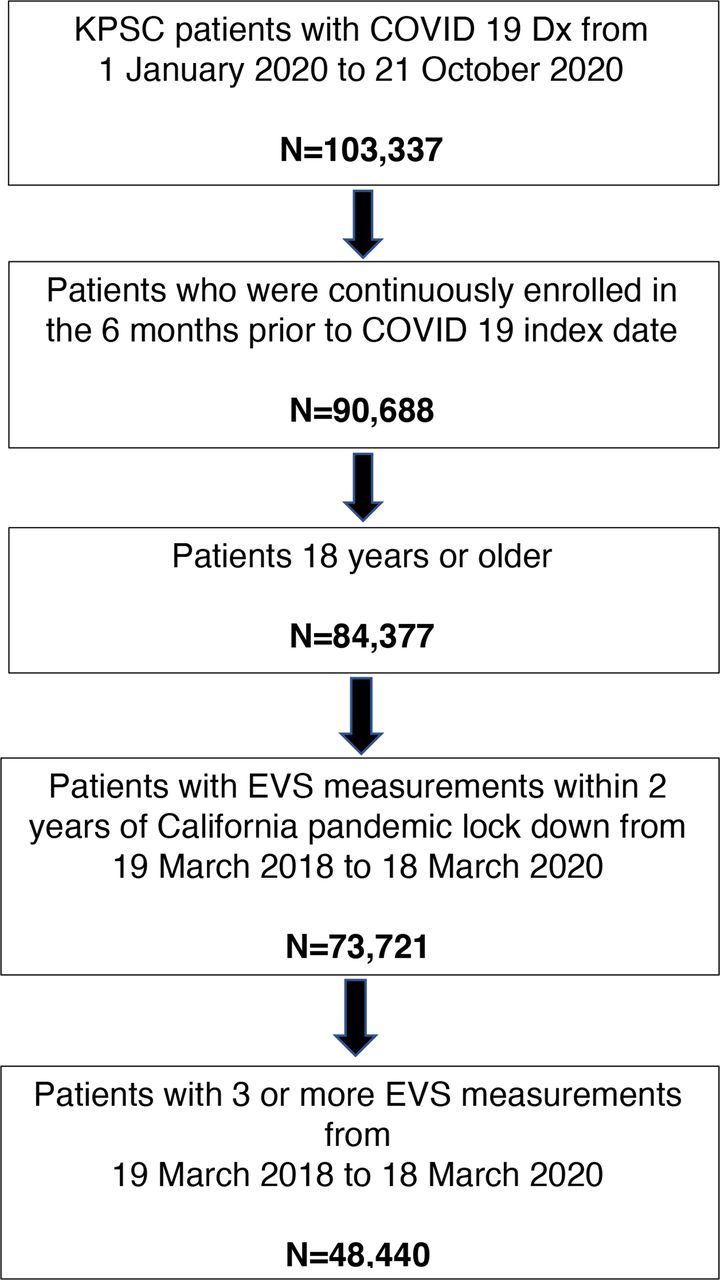
Flow chart of patient selection. EVS, exercise vital sign; KPSC, Kaiser Permanente Southern California.
Demographics
The population had a mean age of 47.5 years (SD 17.0), with a median of 47 years (IQR 33.0, 60.0) and included 61.9% females (table 1). 6.4% were consistently meeting PA guidelines and 14.4% were consistently inactive, with the remainder falling in the some activity category. White patients were most likely to consistently meet PA guidelines (9.4%), followed by Asian patients (7.3%), Hispanic patients (5.5%) and African-American patients (4.6%). The mean BMI was 31.2 (SD 7.07). 51.4% of the study cohort had no comorbidities while 17.4% had only one, and 31.3% had two or more. The percentage of those who were consistently meeting PA guidelines was lower among those with chronic diseases (including obesity) and those who smoked.
Patient characteristics by exercise level
Among all patients with COVID-19, 8.6% were hospitalised, 2.4% were admitted to the ICU and 1.6% died (table 2). Those who were consistently meeting PA guidelines were less likely to be hospitalised, admitted to the ICU or die related to COVID-19 than those who were consistently inactive or doing some activity. In addition, a similar trend was observed for those who were doing some activity compared with those who were consistently inactive.
Hospitalisations, ICU admissions and deaths among patients with COVID-19
Outcomes and adjusted analyses
Controlling for demographics and other risk factors for severe COVID-19, being consistently inactive resulted in significantly higher odds for the three outcomes compared with being either consistently meeting PA guidelines or doing some activity (figures 2–4). Being consistently inactive increased the odds of hospitalisation 2.26-fold (95% CI 1.18 to 2.83) compared with consistently meeting PA guidelines (figure 2). Those who were doing some activity had 1.89 times greater odds of hospitalisation (95% CI 1.53 to 2.33) than those who were consistently meeting PA guidelines. In addition, patients who were consistently inactive had greater odds of being hospitalised (OR 1.20; 95% CI 1.10 to 1.32) than patients who were doing some activity. Other than age, pregnancy and a history of organ transplant, being consistently inactive conferred the highest odds for hospitalisation with COVID-19.

Adjusted risk factors for hospitalisation in patients with COVID-19. BMI, body mass index; ED, emergency department.
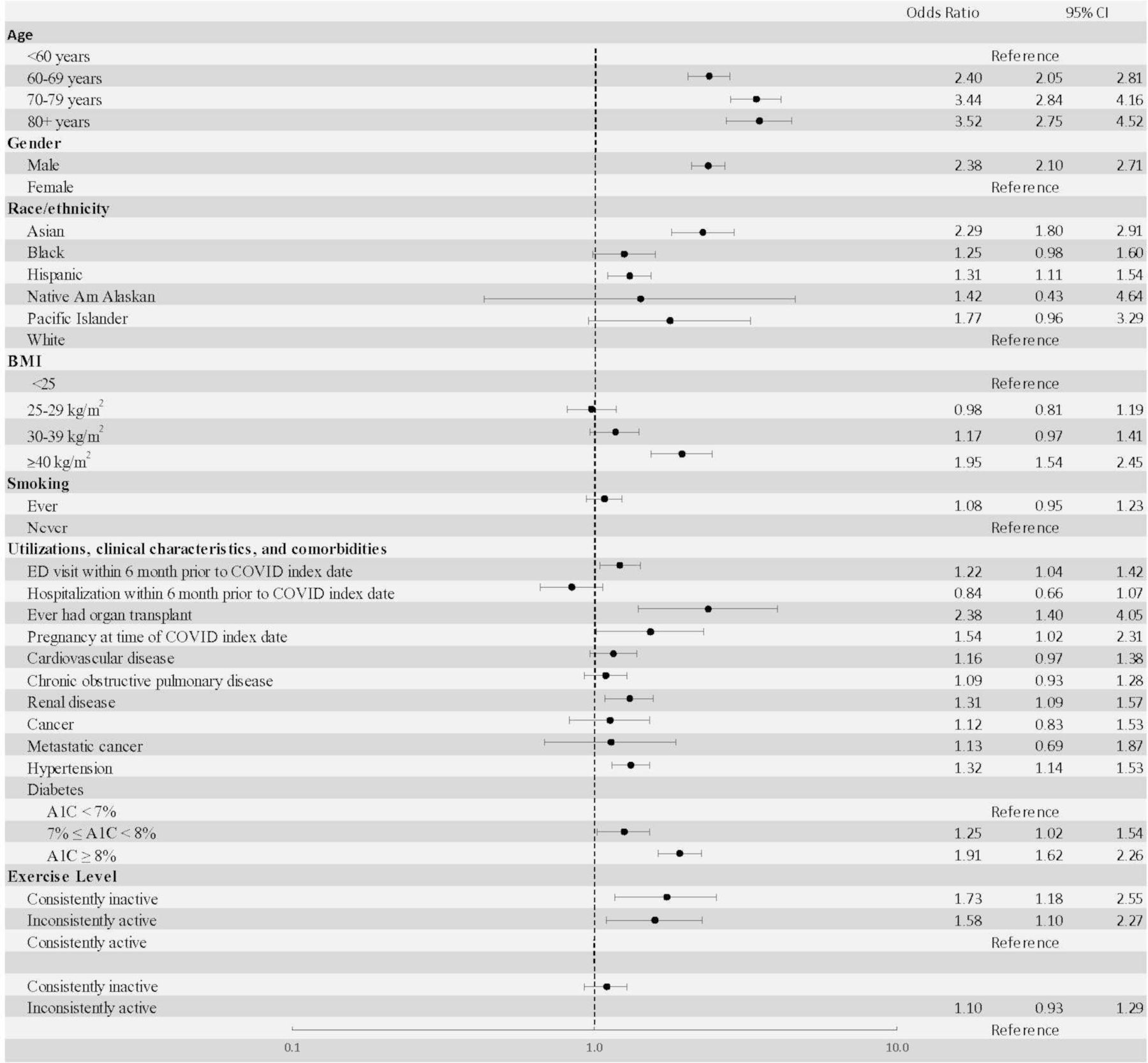
Adjusted risk factors for admission to intensive care unit (ICU) in patients with COVID-19. BMI, body mass index; ED, emergency department.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
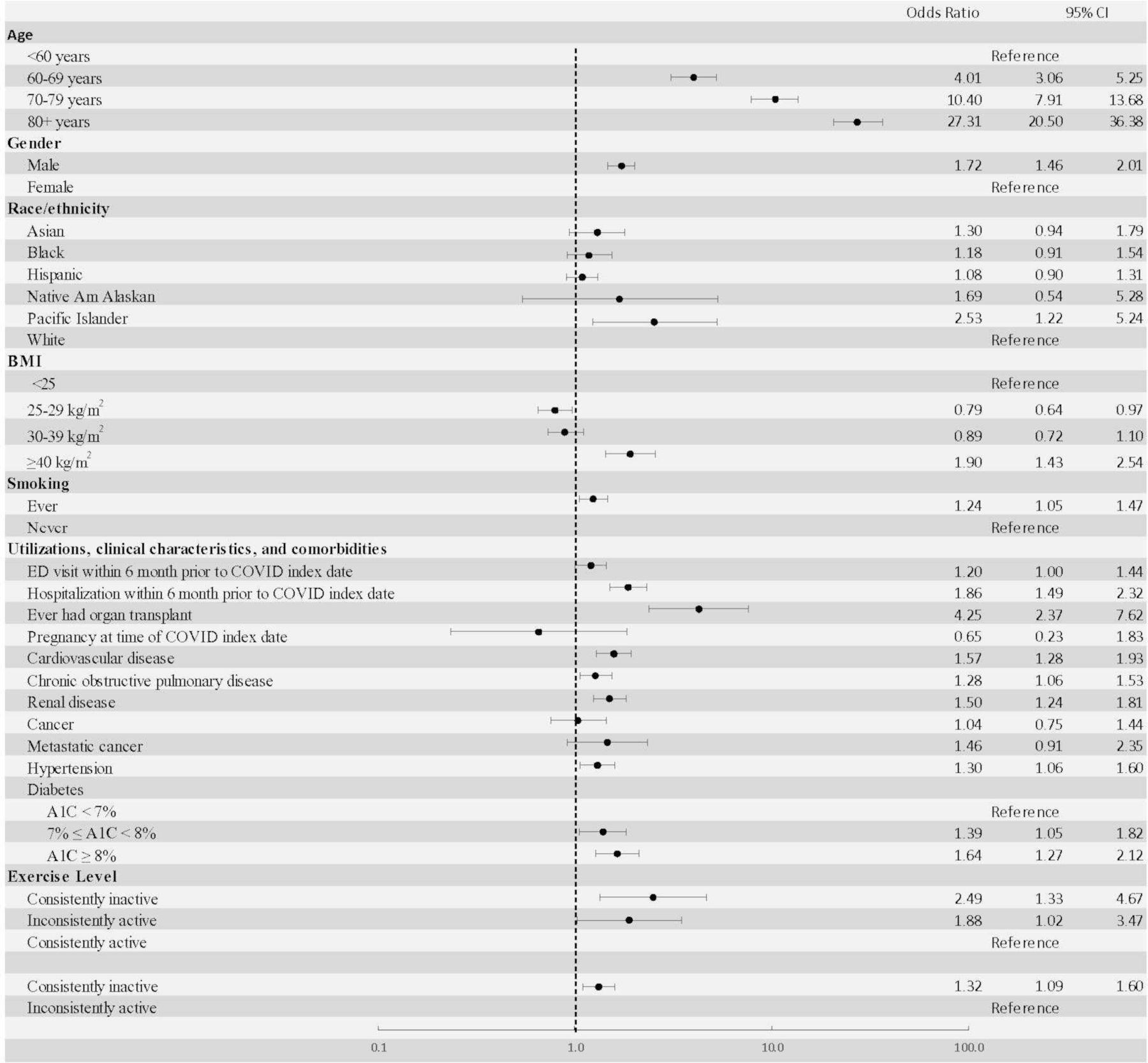
Adjusted risk factors for death in patients with COVID-19. BMI, body mass index; ED, emergency department.
Figure 3 displays the adjusted odds of ICU admission. Patients who were consistently inactive had 1.73 times greater odds (95% CI 1.18 to 2.55) of ICU admission than patients who were consistently meeting PA guidelines. Patients who were doing some activity had 1.58 greater odds for ICU admission (95% CI 1.10 to 2.27) than those who were consistently meeting PA guidelines. Patients who were consistently inactive also appeared to have greater odds of being admitted to the ICU (OR 1.10; 95% CI 0.93 to 1.29) than patients who were doing some activity, though this was not statistically significant.
The adjusted odds of death from COVID-19 are displayed in figure 4. The odds of death were 2.49 times greater (95% CI 1.33 to 4.67) for patients who were consistently inactive compared with patients who were consistently meeting PA guidelines. Patients who were doing some activity had 1.88 times greater odds (95% CI 1.02 to 3.47) of death than those who were consistently meeting PA guidelines. Patients who were consistently inactive also had a greater risk of death (OR 1.32; 95% CI 1.09 to 1.60) than patients who were only doing some activity. Odds of death for consistently inactive patients was robust, and in most instances was higher than the odds of other COVID-19 risk factors.
Discussion
Main findings
Prior PA meeting current guidelines was associated with reduced odds for hospitalisation, ICU admission and death among patients with COVID-19 enrolled in a large integrated healthcare system. Kaiser Permanente is one of the few (and largest) healthcare systems that collect PA data at every outpatient encounter with a healthcare provider. This is the first study we are aware of to demonstrate PA is an important and modifiable risk factor for severe COVID-19 outcomes. The magnitude of risk for all outcomes associated with being consistently inactive exceeded the odds of smoking and virtually all the chronic diseases studied in this analysis, indicating physical inactivity may play a crucial role as a risk factor for severe COVID-19 outcomes. It should be noted that the elevated hospitalisation rate for pregnant patients is due to the fact that all are admitted to the hospital to deliver their baby, and likely does not suggest an increased risk for severe COVID-19-related hospitalisations. In fact, pregnant patients with COVID-19 had a much lower risk of death.
When compared with consistently inactive patients, those in the some activity category had lower odds for hospitalisation and death, suggesting any amount of PA may have benefit. However, doing only some activity provided substantially higher odds for all COVID-19 adverse outcomes than consistently meeting PA guidelines.
The reported ORs for physical inactivity are strong but likely conservative, because the models are adjusted for several chronic conditions that benefit from PA and increase the risk for severe COVID-19. For instance, because physical inactivity is associated with higher BMI and greater risk of diabetes, both comorbidities associated with severe COVID-19 outcomes, the association of PA with negative COVID-19 outcomes may be larger than indicated by our estimates. The ORs for the consistently inactive group were larger than those for almost all the chronic conditions and risk behaviours in the models, so PA may be the most important modifiable risk factor for severe COVID-19. Although data on PA during the COVID-19 pandemic are scarce, a study from the UK found adults with chronic conditions were most likely to report reducing their PA due to the COVID-19 lockdown.20 Thus, promoting PA may be especially important for those with chronic diseases.
PA goals
The US Physical Activity Guidelines established a goal of 150 min/week of MVPA (like a brisk walk) to maximise health benefits.3 This amount can be accrued in small units, making achievement of the guidelines within reach for nearly all people. Other studies have shown that on average, Americans have at least 4–6 hours each day of leisure time, the majority of which is devoted to sedentary activities, particularly electronic media.21 The findings here provide additional rationale and motivation for individuals to be more physically active, as well as for communities to design environments that are more conducive to routine PA,22 23 especially amid the COVID-19 pandemic.
Strengths and limitations
The study’s main strength is the large number of patients with COVID-19 with serial assessment of prediagnosis PA levels. An additional strength is the demographic diversity of the study sample, including almost 65% patients of Hispanic descent. Another important strength is the ability to adjust for a wide range of demographic and health variables that are included in the EHR system. A final strength is the COVID-19 outcomes measured were objective and indicative of COVID-19 severity.
The main limitations of this study are that the measure of PA was self-reported and there was no measure of the intensity of exercise beyond the threshold of ‘moderate to strenuous exercise (like a brisk walk)’. However, this assessment of PA has previously been validated,18 19 and the use of three or more EVS measures allowed for improved estimates of PA and the identification of patients with consistently high and low PA patterns. As an example of validity results, a single EVS assessment obtained up to 2 years prior to accelerometry monitoring for 7 days yielded sensitivity, specificity and positive and negative predictive values for meeting US Physical Activity Guidelines or not of 67%, 68%, 61% and 73%, respectively.24 Importantly, because this is an observational study, it is not possible to definitively conclude PA is causally related to less severe COVID-19 outcomes. These associations could potentially be in reverse; that is, those who have more significant underlying illness may be less likely to include PA in their daily routine or lack the capacity to do so. There is also the potential issue of residual confounding due to unmeasured confounders or measurement error. However, many studies have demonstrated numerous strong benefits from PA, especially among those who suffer from a variety of chronic diseases.25–28
Other limitations include the potential for sparse data in some of the variables. For example, the OR for PA and death outcomes in the highest age category resulted in high ORs and wider CIs. The 80+ age confounder variable in the death regression has an OR of 27.31 and a wide CI (20.50 to 36.38), suggesting that there may be a sparse data problem (and perhaps for other confounding variables). However, confounder imprecision does not bias the target estimator, that is, the association of PA on severe COVID-19 outcomes.29 In addition, some of the confounders are time varying and may not continuously reflect the information recorded during patient interviews.
Conclusion
We found that consistently meeting PA guidelines was strongly associated with a reduced odds for severe COVID-19 among infected adults. Specifically, when compared with those who reported being consistently inactive, those who were consistently meeting PA guidelines had lower odds of being hospitalised, requiring ICU admission and dying from COVID-19. Even activity levels that did not meet the PA guidelines were significantly associated with reduced odds of hospitalisation and death. It is notable that being consistently inactive was a stronger risk factor for severe COVID-19 outcomes than any of the underlying medical conditions and risk factors identified by CDC except for age and a history of organ transplant.1 In fact, physical inactivity was the strongest risk factor across all outcomes, compared with the commonly cited modifiable risk factors, including smoking, obesity, diabetes, hypertension, cardiovascular disease and cancer.
This evidence that physical inactivity is a strong modifiable risk factor for severe COVID-19 contrasts with the limited efforts by US public health authorities to educate the population about the benefits of PA related to adverse COVID-19 outcomes or to systematically promote regular PA during the pandemic. We recommend that public health authorities inform all populations that short of vaccination and following public health safety guidelines such as social distancing and mask use, engaging in regular PA may be the single most important action individuals can take to prevent severe COVID-19 and its complications, including death. This message is especially important given the increased barriers to achieving regular PA during lockdowns and other pandemic restrictions. The results of the present study suggest a clear and actionable guideline for reducing the risk of severe COVID-19 outcomes.
Summary box
What are the findings?
Patients with COVID-19 who were consistently inactive during the 2 years preceding the pandemic were more likely to be hospitalised, admitted to the intensive care unit and die than patients who were consistently meeting physical activity guidelines.
Other than advanced age and a history of organ transplant, physical inactivity was the strongest risk factor for severe COVID-19 outcomes.
Meeting US Physical Activity Guidelines was associated with substantial benefit, but even those doing some physical activity had lower risks for severe COVID-19 outcomes including death than those who were consistently inactive.
How might it impact on clinical practice in the future?
The potential for habitual physical activity to lower COVID-19 illness severity should be promoted by the medical community and public health agencies.
Pandemic control recommendations should include regular physical activity across all population groups.
Data availability statement
No data are available.
Ethics statements
Patient consent for publication
Ethics approval
This study was approved by the Kaiser Permanente Southern California Institutional Review Board.
Acknowledgments
The authors thank Dianne Taylor for her excellent editorial support, Vennis Hong for her outstanding programming support and Jiaxiao M Shi for his project oversight.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @drbobsallis
Contributors RS, DRY and SYT gained funding for the study. RS, DRY, SYT, JFS, JS, GNS and DAC conceived the study idea and contributed to writing of the first draft of the manuscript. RS, DRY, SYT, JFS, JS, QL, GNS and DAC interpreted the data analysis, and conducted data validation and data visualisation. All authors contributed to revisions of the manuscript and approved the submitted version.
Funding This study was supported in part through funding from the Kaiser Permanente Community Benefits Funds.
Competing interests SYT reports grants from Roche/Genentech during the conduct of the study.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.