Article Text

Abstract
Objective To determine whether occupational exposure to silica dust is associated with an increased risk of developing sarcoidosis.
Design Case–control study of all individuals between 20 and 65 years of age diagnosed with sarcoidosis (D86) in Sweden between 2007 and 2016. Controls were matched to cases (2:1) based on age, sex and county at the time of diagnosis. A Job Exposure Matrix was used to estimate the occupational silica exposure of all cases and controls.
Setting Medical and occupational data from the National Outpatient Register were used to implement a case–control analysis, while the two controls used for each case were selected from the National Register of the Total Population. Information about occupation and time of employment were collected from the Swedish Occupational Register.
Participants All men and women aged 20–65 years old who were diagnosed sarcoidosis (D86) from 2007 to 2016 were included and assigned two controls.
Main outcomes Silica dust exposure correlates with an increased risk of developing sarcoidosis in men.
Results The prevalence of silica exposure at work was statistically significantly higher among male cases than controls (OR 1.27, 95% CI 1.13 to 1.43). For men of an age of 35 years or younger the correlation seems to be stronger (OR 1.48, 95% CI 1.1 to 1.87) than in older men (OR 1.21, 95% CI 1.05 to 1.39). For men older than 35 with exposure to silica the prevalence of sarcoidosis increased with the exposure time, with an OR of 1.44 (95% CI 1.04 to 2.00) for exposure of more than 10 years.
Conclusions Occupational exposure to silica dust seems to increase the risk of sarcoidosis among men between 20 and 65 years of age. The risk is higher among exposed men 35 years or younger and older men with longer exposure (>6 years).
- occupational & industrial medicine
- epidemiology
- interstitial lung disease
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This case–control study includes all, in the included age groups, who were diagnosed with sarcoidosis in Sweden from 2007 to the end of 2016.
Sweden maintains high-quality registers that cover the entire population, together with unique personal identification numbers that can link patient data across different nationwide registers.
The diagnoses were based on data recorded in the National Non-primary Outpatient Visits Register, which is significantly more accurate than diagnoses based on questionnaires.
This study lacks information on potential confounders such as smoking habits, however cases and controls are matched based on age, sex and geographical area in order to reduce the impact of possible confounders.
Background
Sarcoidosis is a systemic inflammatory disease that is characterised by the formation of granulomas in various organs, most commonly the lungs and/or intrathoracic lymph nodes. There are three diagnostic criteria for sarcoidosis: clinical and radiological presentation, non-caseating granulomas in biopsy tissue from the affected organ and ruling out alternative diagnoses.1 In Sweden, the incidence is 11.5 per 100 000 per year with a peak in men aged 30–50 and in women aged 50–60. The incidence is heterogeneously spread across different counties. The proportion of men with sarcoidosis is slightly higher compared with women (56% vs 44%).2
The aetiology remains an unsolved problem. Suggestions have been made that sarcoidosis is a reaction to a currently unidentified environmental factor in genetically predisposed individuals.1 Proposed environmental and occupational risk factors are, as suggested by the ACCESS (A Case–Control Etiologic Study of Sarcoidosis) Study, insecticides, agricultural employment and mouldy, musty environments typically associated with bioaerosol exposure. In the ACCESS Study, no associations with silica were found.3 Another study, by Deubelbeiss et al, found that agricultural production and metal-processing industries near the residential area were environmental factors positively associated with the frequency of sarcoidosis.4 Respirable crystalline silica/respirable silica dust, has also been proposed to be an environmental factor, although there are currently only a handful of published studies on silica and sarcoidosis.
In Sweden, about 85 000 workers are exposed to respirable silica dust by their profession.5 Silica exposure is mainly known to cause silicosis, a fibrotic and potentially fatal lung disease.6 Yet silica is not only associated with silicosis; a large case–control study from the USA investigating occupational silica exposure and risk of various diseases found an association with lung cancer, chronic obstructive pulmonary disorder, pulmonary tuberculosis and rheumatoid arthritis (RA) as well. No associations with sarcoidosis were found.7
Two studies on workers in iron foundries and construction workers exposed to airborne silica, respectively, found an increased risk for sarcoidosis in exposed workers.8 9 In Iceland, a study on workers exposed to diatomaceous earth and cristobalite (crystalline silica) reported an increased incidence of sarcoidosis compared with the incidence for the general population of Iceland, however this study only included eight cases of sarcoidosis.10 Furthermore, there are also a few case reports where silica is said to have caused sarcoidosis. In one case, cat litter containing mainly silica was considered the cause, and in another case silica as an excipient in oral drugs was blamed. Even silicone implant placement is believed to have caused sarcoidosis in one subject.11–13 However, another case report argues that some cases of sarcoidosis might be misclassifications of silicosis.14
The aim of this study is to investigate whether sarcoidosis is associated with occupational exposure to respirable silica dust.
Material and method
A unique personal identification number is distributed to all Swedish residents. Sweden holds various nationwide registers, and with the use of the unique personal identification number it is possible to link data from several different registers, which provides a unique opportunity to analyse the entire patient population of Sweden. Since healthcare is paid through taxes, all inhabitants have equal access to healthcare and hospital services. This makes Sweden a country well-suited for epidemiological studies.
All individuals between 20 and 65 years of age and diagnosed with sarcoidosis in Sweden (classified as D86 under the ICD10 standards) between 1 January 2005 and 31 December 2016 were collected from the National Non-primary Outpatient Care Register. This register is maintained and validated by the Swedish National Board of Health and Welfare and contains data on registered outpatients of healthcare facilities throughout Sweden since 2001. However, when investigating the annual cases of sarcoidosis there was an elevated number of cases in the first 2 years after the register was established (2005–2006). This might be as a result of individuals being registered in the newly established register during follow-up medical examinations in addition to new cases. As the date of the first diagnosis cannot be established for the patients registered in the follow-up medical examinations, cases from 2005 to 2006 were thus excluded (wash-out period).
For each case of sarcoidosis, two control individuals from the general population were assigned by Statistics Sweden (SCB). The controls were selected to match the cases by age, sex and the county of residence at diagnosis. The controls must not themselves have sarcoidosis or be a first grade relative (sibling, parent or child) to the case. In addition, the controls were selected as to not have the following diagnoses: ankylosing spondylitis (M45), rheumatoid arthritis with rheumatoid factor (M05), other rheumatoid arthritis (MO6), Crohn's disease (K50) or ulcerative colitis (K51). These other diagnoses were excluded as this cohort is part of a larger cohort used in other studies.15 16
To determine the occupation and time of employment in the cohort, the Swedish Occupational Register held and maintained by SCB was used. To be counted as silica-exposed, the individual must have worked within a profession with exposure to respirable silica dust within the last 5 years. Cases or controls exposed to respirable silica dust earlier in life but not within the past 5 years before diagnosis were thus excluded together with their matched controls/cases due to the gap between end of exposure and onset of disease. The exposure for respirable silica dust was estimated using an updated job-exposure matrix (JEM) based on the PARrticles and Cardio- and Cerebrovascular disease (PARCC)-JEM.17 18 The updated PARCC-JEM is a time-specific JEM compromising the time period 1955–2014 and stratified into six 10 year periods. For the last 2 years of this study (2015–2016) the exposure assessment was done using the exposure data from the last 10-year period in the JEM. This JEM was developed by combining exposure measurements from Sweden, or when not available, other Nordic countries. The JEM was based on already existing information from a Swedish JEM developed for the Nordic Occupational Cancer Study, as well as an Airway Irritant-JEM, and thus gives apart from exposed occupations also provides information on exposure prevalence and exposure levels for each exposed job-title.17 The exposure levels for each occupation were obtained by calculating the product of exposure prevalence and exposure level for the relevant time periods. The JEM classifies jobs as exposed when at least 5% of the workers in a job is exposed to an annual mean level of 0.02 mg/m³ respirable crystalline silica dust. Jobs that matched those criteria included concrete workers, casters, masons, ceramic and glass manufacturers, miners, and others. The background characteristics are presented using descriptive statistics and are reported as number (n), percentage (%), mean and ±SD. The OR of being exposed to respirable silica dust in cases compared with controls was calculated using conditional logistic regression and is presented with 95% CIs. Stratification according to age in years (>35/≤35), sex (male/female), cumulative exposure as mg/m3 year (0, 0.01–0.99, 1.0+), mean exposure as mg/m3 (0, 0.01–0.05, 0.051+) and length of exposure in years (0–1, 2–5, 6–10, 11+) were made. Thirty-five years of age was chosen as a stratification for age as to split the two incidence peaks found in the younger and older age groups.2 For mean exposure, the stratification was chosen as below or above 0.05 mg/m3 (which is 50% of the current Swedish occupational exposure level (OEL)). There were too few high exposed to justify further classes for higher exposures. For cumulative exposure a division of the exposure below or above 1.0 mg/m3 year was chosen on the basis that this is similar to 10 years of exposure at the current Swedish OEL (0.1 mg/m3).
Results
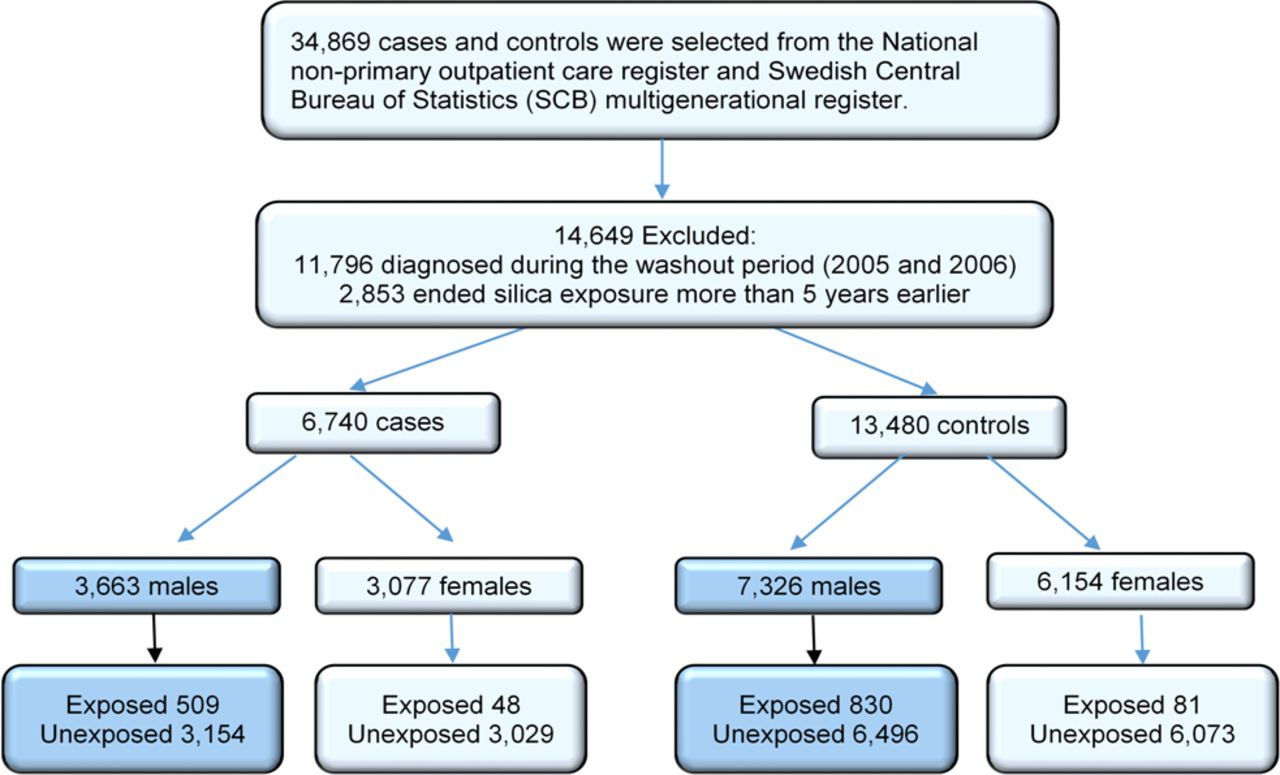
From the National Non-primary Outpatient Care Register 11 623 cases of sarcoidosis in the ages between 20 and 65 years were collected. Each case was assigned two controls as described above giving in total 34 869 cases and controls (figure 1). Of these 14 649 cases and controls were excluded: 11 796 due to the cases being diagnosed during the wash-out period and 2853 due to either the case (480) or at least one of the controls (812) only having exposure to respirable silica dust that ended more than 5 years ago (ie, they had been exposed to respirable silica dust earlier, but not within the past 5 years). In addition, when using the JEM to evaluate silica exposure, the number of women exposed to silica was low (48 cases and 81 controls). The following results presented in this study were consequently only based on data from the male cases and controls.
{kind=link}
Flowchart that visualises inclusion and exclusion of the study population.
Included in the study were thus 3663 cases and 7326 controls, all men. The mean age of cases and controls was 44.7 years old (±10.9 SD). Of cases, 13.9% were exposed to respirable silica dust within the latest 5 years, of controls the proportion was 11.3%. The background characteristics are presented in table 1.
Background characteristics
Overall, men with sarcoidosis were more likely to have been exposed to respirable silica dust in their occupation within the previous 5 years (OR 1.27, 95% CI 1.13 to 1.43), as seen in table 2. The association is statistically significantly stronger (p=0.02) in men diagnosed before 35 years of age (OR 1.48, 95% CI 1.16 to 1.87), than in men older than 35 years at the time of diagnosis (OR 1.21, 95% CI 1.05 to 1.39).
Prevalence of sarcoidosis in men exposed to respirable silica dust within 5 years of diagnosis stratified into length of exposure and age of diagnosis
Number of years with exposure seems to matter. In all men with sarcoidosis, it was significantly more likely to have been exposed to silica for 2–10 years before diagnosis, than it was to not have been exposed at all. For men exposed to silica for more than 11 years there was also an increased risk for sarcoidosis, however not statistically significant.
When men were divided into age at diagnosis, the younger population with sarcoidosis (35 years or younger) was more likely to have been exposed to silica for a year or more, while the older population with sarcoidosis (older than 35 years) was more likely to have been exposed to silica for 6 or more years.
When the JEM was used to estimate the exposure frequency and exposure levels, exposure to respirable silica dust statistically significantly increase the OR for sarcoidosis, but neither the cumulative nor mean exposure show a statistical significant dose–response association (table 3).
Prevalence of sarcoidosis in men exposed to respirable silica dust within 5 years of diagnosis stratified into cumulative (mg/m3 years) and mean (mg/m3) exposure and age of diagnosis
Discussion
The aim of this longitudinal case–control study of the Swedish population was to examine whether cases with sarcoidosis have been exposed to respirable silica dust at the workplace during the years 2007–2016 more often than controls. The incidence of sarcoidosis in Sweden found in this study was 12 per 100 000. This is in agreement with a previous study that found an incidence of sarcoidosis in Sweden of 11.5 per 100 000.2 However, the current study only investigated the age groups between 20 and 65 years of age.
Exposure to respirable silica dust seems to result in an increased risk for developing sarcoidosis in men. For women the prevalence of silica exposure was low (only 48 cases and 81 controls), and they were thus not included in this study (figure 1). The prevalence of silica exposure at work was statistically significantly higher among male cases than controls (OR 1.27, 95% CI 1.13 to 1.43). For men of an age of 35 years or younger the correlation was statistically significant stronger (OR 1.48, 95% CI 1.1 to 1.87) than in older men (OR 1.21, 95% CI 1.05 to 1.39) (p=0.02) (table 2).
For the younger men (≤35 years) exposure to respirable silica dust resulted in an increased risk of sarcoidosis, especially at shorter exposure time. Sarcoidosis can be subdivided into an acute form, Löfgren syndrome, which in Scandinavia can account for up to 30% of the sarcoidosis cases; and a more chronic form, the acute form culminates at age 25–30.19–21 This may explain why younger individuals have a shorter exposure time to the onset of disease than do older individuals. There are some reports in the literature that silicosis can be misdiagnosed as sarcoidosis particularly in young men.14 However, as sarcoidosis in Sweden is diagnosed using bronchoscopy, biopsy or bronchoalveolar lavage the risk for misdiagnosis is small. Also silicosis is currently rare in Sweden due to the fact that the legislation against respirable silica dust exposure has successfully reduced the OELs.22 For men older than 35 with exposure to respirable silica dust the risk of sarcoidosis increased with the exposure time, with an OR of 1.44 (95% CI 1.04 to 2.00) for exposure of more than 10 years (table 2). When applying information about respirable silica dust exposure from the JEM, neither stratified cumulative nor mean exposure showed a statistical significant dose–response association (table 3). There are, however, few high exposed individuals among the study population (online supplementary file 1). A previous study on respirable silica exposure and sarcoidosis in iron foundry workers found highest incidence rates among the individuals with the highest mean exposure.8
Supplemental material
The increased risk for sarcoidosis among young men (<35 years) exposed to respirable silica dust is in line with observations from other studies which indicate that men seem to develop sarcoidosis at an earlier age than women, probably due to an environmental factor.2 This suggested external factor could thus be occupational exposure to silica. A potential causative mechanism of sarcoidosis is the activation of an immune response in genetically predisposed individuals by an inhaled exogenous substance.23 As noted above, our results suggest that inhaled silica dust may be such a causative or contributing exogenous factor. The mechanisms for how silica works as an exogenous factor are not known, but it has been shown that presence of silica in the lungs can drive macrophage polarisation towards type 2 macrophages.24 Type 2 macrophages are suggested to be of importance for the formation of granulomas.25 26 Silica exposure has also been shown to increase the risk for tuberculosis;27 the explanation for this could also be the increased pool of M2 macrophages driven by silica exposure.24 25 As suggested by Agrawal et al, perhaps sarcoidosis and tuberculosis are opposite ends of the same disease,28 but with silica driving the formation of granulomas.
Apart from silicosis, silica has also been associated with various systemic autoimmune diseases including RA, but also with systemic lupus erythematosus, systemic sclerosis and antineutrophil cytoplasmic antibody-related vasculitis.8 29 30 This could also be attributed to M2 polarisation after silica exposure, as M2 macrophages might be a driver of the autoimmunity.31
The main strength of this study is that all registered cases of sarcoidosis in Sweden between 2007and 2016 were included by using a national, well maintained and validated register, and that not only sarcoid cases from specific occupations were included, as in previous studies.8 9 The study’s main weakness is the use of a JEM as an exposure matrix. The presence of respirable silica dust at a job site does not in itself mean that all employees would have been exposed. The JEM we have used tries to take this into account by estimating fraction of exposed within each job category, however it cannot be ruled out that this may have exaggerated the number of exposed individuals. However, the JEM has been developed independently of this study and if the JEM overestimated the detrimental level of silica exposure for non-exposed cases in the exposed occupations, this would only weaken the correlation between exposure and morbidity. Another limitation of this study is that as this is a register study there is a lack in information on potential confounders, such as smoking habits. In addition, other aspects which could influence the course of the disease, such as therapy, are not part of the register. However, cases and controls are matched based on age, sex and geographical area in order to reduce the impact of possible confounders. The JEM used in this study only gives information on respirable silica exposure, hence other occupational exposures that might be linked to either sarcoidosis or sarcoid-like granulomatous lung diseases such as chronic beryllium disease have not been investigated.
In Sweden it is mandatory to undergo medical controls on a regular basis that include lung X-ray and spirometry when exposure to respirable silica dust is above 0.05 mg/m3. Chest X-ray is conducted at start of work and then on regular basis (after 9 years and then every 6th year). It is therefore a risk for detecting asymptomatic cases of sarcoidosis among the exposed and the extra chest X-ray is a potential confounder. However, the increase in sarcoidosis is higher in low exposed groups that are not required to undergo medical controls with chest X-ray. Also, workers with asymptomatic sarcoidosis would probably be predominantly identified at the first chest X-ray rather than later, and in this study the highest ORs are found among the individuals with longer exposure times (table 2).
Conclusion
Exposure to respirable silica dust increases the risk of sarcoidosis among men between 20 and 65 years of age. The risk seems to be higher among exposed men 35 years or younger and older men with longer exposure (>6 years).
References
Footnotes
Contributors PV, I-LB and PG conceived and designed the study. PW constructed the adopted JEM. I-LB did the main data analysis and JL, PV, I-LB and PG interpreted the results. JL, PW, PV, I-LB and PG participated in the writing of the manuscript. All authors approved the final version.
Funding This study was done with support from Region Örebro County.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The study was approved by the Swedish Ethical Review Authority; DNR 2017/252.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. The data used in this study were derived from The Swedish National Patient Register, which is collected, maintained and owned by the Swedish National Board of Health and Welfare (http://www.socialstyrelsen.se). Access to data on the incidence of sarcoidosis was granted based on the ethical committee's approval of undertaking this study. Any researcher, granted that they have an ethical approval from a regional ethical board, can use the data in the Swedish National Patient Register. However, the Swedish National Board of Health and Welfare will also put restrictions on sharing sensitive information. Data access requests can be directed to the Regional Ethical Board in Uppsala: https://www.epn.se/start/ or registrator@uppsala.epn.se.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.