Article Text

Abstract
Background Emergency departments (ED) are important providers of asthma care, particularly after-hours. We identified gaps for quality improvement such as suboptimal adherence rates to three key recommendations from the Global Initiative for Asthma (GINA) guidelines for discharge management asthma guidelines. These were: the prescription of oral and inhaled corticosteroids (OCS and ICS) and issuance of outpatient follow-up for patients discharged from the ED.
Aim To achieve an adherence rate of 80% to GINA guidelines for ED discharge management by providing after-hours asthma counselling services.
Methods We implemented Asthma-COPD Afterhours Respiratory Nurse at Emergency (A-CARE) according to the Plan-Do-Study-Act (PDSA) framework to provide after-hours asthma counselling and clinical decision support to ED physicians three nights a week. Data on adherence rates to the GINA guidelines were collected and analysed on a run chart.
Results After 17 months’ follow-up, a sustained improvement was observed in patients reviewed by A-CARE in the median adherence rates to OCS prescription (58% vs 86%), ICS initiation (27% vs 67%) and issuance of follow-up (69% vs 92%), respectively. The overall impact was, however, limited by a suboptimal referral rate to A-CARE (16%) in a clinical audit of all ED patients with asthma. Nonetheless, in this audit, attendance rates for patients referred to our respiratory department for follow-up were higher in those receiving asthma counselling compared with those who did not (41.7% vs 15.9%, p=0.0388).
Conclusion Sustained improvements in the adherence rates to guidelines were achieved for patients reviewed by A-CARE but were limited in overall impact due to suboptimal referral rate. We plan to improve the quality of asthma care by implementing further PDSA cycles to increase the referral rates to A-CARE.
- asthma
- emergency department
- patient education
- quality improvement
- nurses
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Problem description
Asthma is characterised by nocturnal worsening of symptoms and emergency departments (ED) are often the only place that patients can seek after-hours acute care for asthma. Worldwide, the ED continues to be a major source of asthma care1–3 despite being shown to be costly4–7 and inadequate with significant variation in evaluation and treatment.8 In addition, suboptimal adherence to recommended practices in guidelines has been reported in EDs around the world with low rates of prescription of systemic corticosteroids and inhaled corticosteroids (ICS),9 provision of written discharge advice and follow-up review on discharge.10 A retrospective analysis of patients who presented to our ED with a primary diagnosis of asthma was previously performed and inadequate adherence to clinical practice guidelines was similarly found.11 Only 59% of patients in our ED were given a course of systemic corticosteroids and poor adherence to guidelines was found to be associated with a higher ED reattendance rate. Suboptimal quality of asthma care in our ED is also further compounded by the lack of availability of asthma counselling after-hours.
Available knowledge
Despite advances in the quality and accessibility of healthcare in Singapore, asthma-related mortality and morbidity in Singapore continues to lag behind that of other developed countries.12 Efforts to improve the quality of primary care of asthma in Singapore through the Singapore National Asthma Programme13 have paid off with increased rates of guideline-recommended best practices such as the provision of written asthma action plans and use of controller medications.14 Unfortunately, there remains the subset of high-risk asthmatics who elude the primary care system by only seeking episodic symptomatic treatment for acute exacerbations in EDs without receiving controller treatment and regular follow-up. Only a minority of these patients consult primary care prior to ED attendance15 and they have been shown to significantly contribute to healthcare resource usage16 and mortality.17 These ‘frequent attenders’ have been found to disproportionately account for 45% of the total visits to our ED despite only comprising 17% of all ED patients with asthma with longer hours spent in the ED.16 It is now imperative that we look to improving the quality of asthma care in the ED as the next frontier if we are to achieve further reductions in asthma mortality and morbidity.
Methods
Context
This quality improvement (QI) project was conducted in the ED of Singapore General Hospital (SGH), the largest acute tertiary and teaching hospital in Singapore. SGH comprises 1785 beds that receives approximately 130 000 ED attendances annually. A multidisciplinary QI team was formed to study and implement a QI project under the Institute for Healthcare Improvement’s (IHI) Plan-Do-Study-Act (PDSA) framework to improve the quality of asthma care in our ED. This team comprised nurses and specialist physicians from both the departments of emergency and respiratory medicine.
Assessment of problems
A root cause analysis was first performed by the QI team to identify the factors that contributed to low adherence to guidelines (figure 1). Through a Pareto vote analysis, the multidisciplinary QI team assessed that the lack of knowledge of clinical guidelines, particularly front-line junior physicians, was the most significant contributory factor to low adherence to asthma clinical guidelines. First, many junior ED physicians were residents of various medical and surgical specialist training programmes undergoing a rotation in the ED as part of their training schedule. Front-line junior ED physicians therefore had wide variation in clinical knowledge and often lacked experience in holistic management of asthma. Second, there was high staff turnover of junior ED physicians who undergo rotations in ED ranging from 1 to 6 months after which they would be rotated back to their primary training programme. Continuing medication education (CME) activities on asthma management were therefore unable to match the pace of staff turnover. In addition, the attendance of CME activities was also often low due to the nature of shift work, where approximately a third of all ED physicians would be on active clinical duty at any time of the day. Third, asthma clinical guidelines are lengthy and revised frequently on an annual basis, making them inaccessible to non-respiratory specialist end users.18
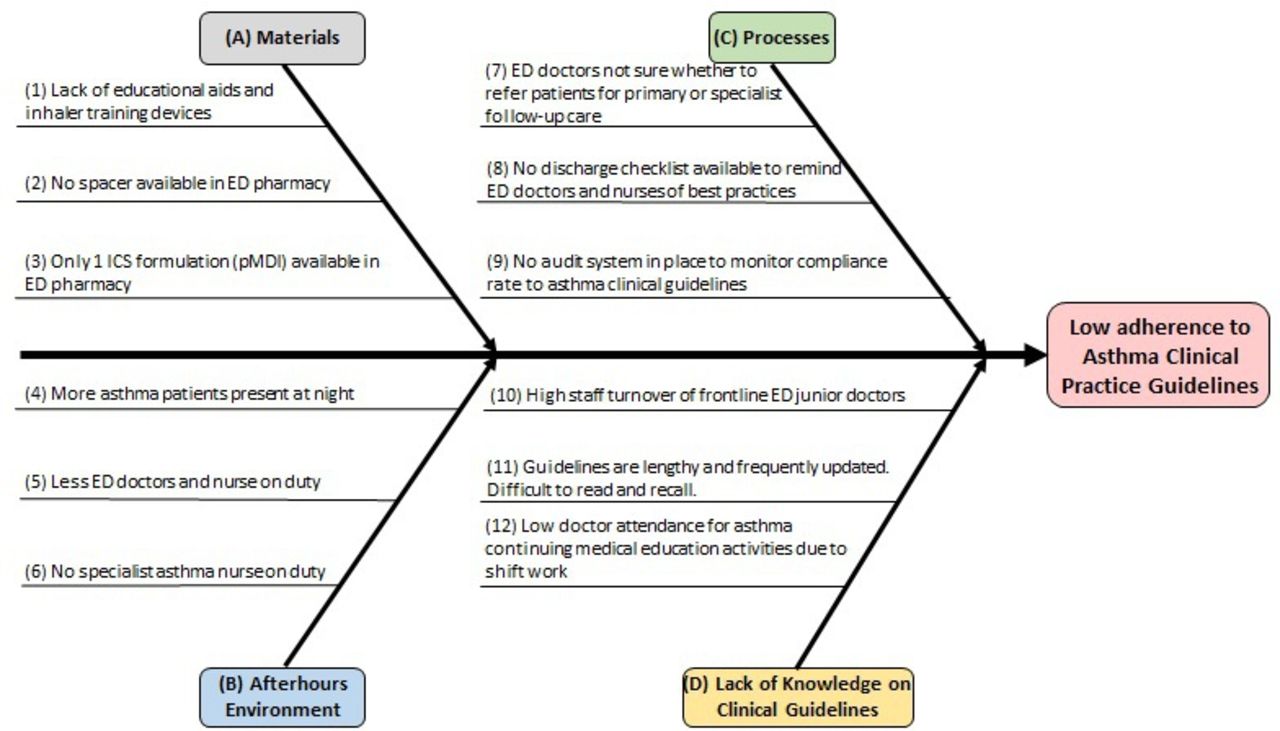
Fishbone diagram: root cause analysis of low adherence to asthma clinical practice guidelines in the emergency department (ED). ICS, inhaled corticosteroids; pMDI, pressurised metered-dose inhaler.
The QI team also referenced a pilot asthma programme that was conducted in another acute general hospital in Singapore where specialist asthma nurse care was made available to ED patients during office hours.19 In this study, asthma nurses provided brief asthma education, issued self-management plans to patients, recommended asthma inhaler therapy to ED physicians based on a clinical protocol and advocated for appropriate postdischarge follow-up. This resulted in improvements in the prescription rates of ICS with modest reductions in hospitalisation and ED reattendance rate. An important limitation of this intervention cited by the study team, however, was the fact that the majority of asthma cases would typically present at 15:00–06:59 hours which was when the ED was typically busiest.20 Our QI team therefore hypothesised that extending the pre-existing asthma counselling service from ‘office hours only’ to include ‘afterhours’ could further improve adherence to clinical guidelines. This would be achieved by providing onsite clinical decision support to front-line ED healthcare providers, particularly junior physicians, who may lack experience and expertise in asthma management.
QI objectives
An after-hours asthma counselling service named Asthma-COPD Afterhours Respiratory Nurse at Emergency (A-CARE) was therefore initiated to improve the quality of asthma care in the ED by providing after-hours asthma counselling and clinical reminders to ED physicians. We aimed to achieve an 80% rate of adherence to three key recommendations from the Global Initiative for Asthma (GINA) guidelines for discharge management after emergency or hospital care for asthma.21 These were: the prescription of oral corticosteroids (OCS) and ICS, and issuance of outpatient follow-up review within 2 weeks.
Role of the A-CARE nurse
A certified nurse was engaged under A-CARE to provide after-hours specialist asthma nurse support on three nights per week (Monday, Tuesday, Friday) for patients who presented to our ED from 18:00 to 08:00 hours (figure 2). The A-CARE nurse would first provide asthma counselling to patients comprising education, inhaler device training and provision of personalised written action plans. When patients were subsequently assessed to be medically fit for discharge from the ED, the A-CARE nurse would provide face-to-face clinical decision support with the ED physician. This consisted of recommendations and reminders to prescribe a course of OCS, initiate controller-naïve patients on ICS and issue outpatient asthma follow-up review. Finally, the A-CARE nurse systemically tracked the attendance rates of patients who were referred to our respiratory clinics for follow-up after discharge and audited the compliance rate of OCS prescription, initiation of ICS and issuance of outpatient asthma follow-up.
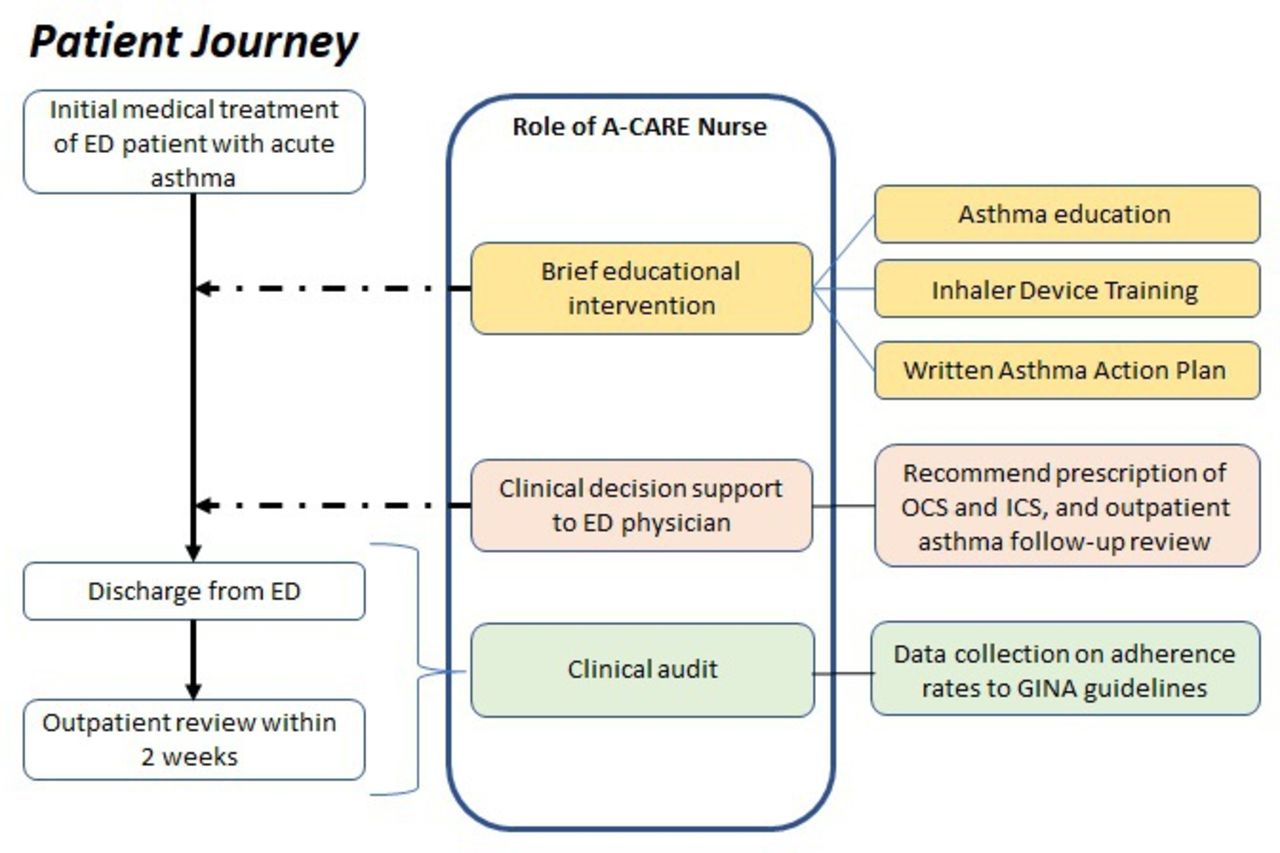
Role of Asthma-COPD Afterhours Respiratory Nurse at Emergency (A-CARE) nurse in the management of patients with acute asthma in the ED. ED, emergency department; GINA, Global Initiative for Asthma; ICS, inhaled corticosteroids; OCS, oral corticosteroids.
Data collection and analysis
The A-CARE nurse collected prospective data on the adherence rates to the GINA guidelines along with asthma-related history from ED patients who were referred for asthma counselling. Deidentified data were collated in a password-encrypted Microsoft Excel database and shared with the QI team for analysis. A two monthly run chart, using the IHI methodology,22 was chosen to demonstrate the effect of QI interventions on the above endpoints.
In order to measure the referral rate to the A-CARE nurse in PDSA cycle 2, a key process step in our QI intervention, the QI team performed a clinical audit of deidentified aggregated data on the electronic medical records of all patients presenting to our ED with a primary diagnosis of asthma from September 2018 to January 2019. Comparisons between groups of patients seen by the A-CARE nurse and those who were not seen by A-CARE nurse were performed using the χ2 test. This study follows the Standards for Quality Improvement Reporting Excellence V.2.0 publication guidelines for reporting.23
A-CARE PDSA cycle 1: roll-out of A-CARE with reminders at ED department meetings
Prior to the implementation of A-CARE, asthma counselling services were only available during office hours. It was therefore necessary to inform the ED healthcare providers about the new after-hours service and its intended goals. From a content standpoint, key messages that were delivered to ED healthcare providers were to refer all patients with a diagnosis of asthma, chronic obstructive pulmonary disease (COPD) or asthma-COPD overlap to the asthma nurses on duty, receive the clinical decision support recommendations of the A-CARE nurse and adhere to clinical practice guidelines for asthma discharge management in the ED. The ED was also regularly updated about the adherence rate to prescriptions of oral and inhaled steroids and outpatient follow-up reviews through their senior management. In PDSA cycle 1 (September 2017 to April 2018), we implemented our change idea of delivering updates to ED physicians on A-CARE. These updates took the format of face-to-face briefings held during the monthly ED department meetings that were led by the ED physicians in our QI team with support from the respiratory physicians and asthma nurses of the QI team. Deliberate care was taken to convey the message to the ED audience that the A-CARE nurse was at their service to help them provide holistic asthma care in a busy environment as opposed to being an inspector for quality control. Updates were also sent via email for ED staff who were not able to attend the monthly ED department meetings.
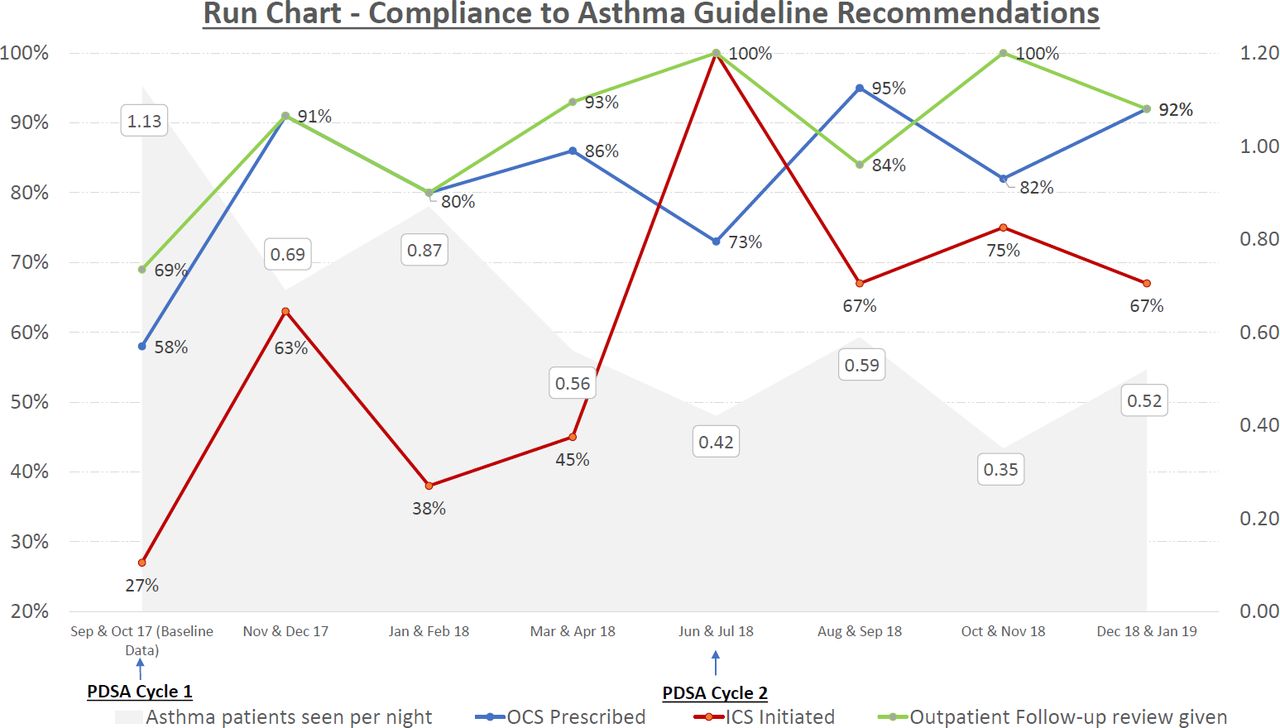
We performed an interim review and found that patients referred to the A-CARE nurse had higher rates of adherence to clinical practice guidelines. However, we observed that referral rates to the A-CARE nurse remained low despite repeated reminders and updates. It was found that on average, less than one patient with asthma was referred to the A-CARE nurse per night on duty (figure 3). During the planning phase, we were initially expecting difficulties in the uptake of clinical decision support recommendations by ED physicians who might view the recommendations as interfering with their clinical judgement. Feedback from our A-CARE nurse, however, informed us that her recommendations were generally welcomed and implemented as evidenced by higher rates of adherence to prescriptions of oral and inhaled steroids and outpatient follow-up review. Further feedback from our ED physicians in the QI team revealed that few junior front-line ED physicians regularly attended ED department meetings and therefore lacked awareness. We therefore decided to adapt our change idea for PDSA cycle 2 to focus on delivering the content to junior ED physicians.
{kind=link}
{kind=link}
{kind=link}
Run chart showing compliance to asthma guideline recommendations (in coloured lines) and patients with asthma seen by Asthma-COPD Afterhours Respiratory Nurse at Emergency (A-CARE) nurse per night (in grey). ICS, inhaled corticosteroids; OCS, oral corticosteroids; PDSA, Plan-Do-Study-Act.
A-CARE PDSA cycle 2: A-CARE nurse-led case-finding strategy and dedicated CME sessions for junior ED physicians
In PDSA cycle 2 (June 2018 to January 2019), the QI team implemented the change idea of a case-finding strategy whereby the A-CARE nurse would perform regular screening of ED patient lists for patients with asthma so that there was less reliance on getting a referral from an ED physician. In addition, the respiratory physician members of the QI team supported and conducted dedicated CME activities for junior ED doctors in the months of July 2018 and October 2018 to raise awareness of the A-CARE QI project. We received informal feedback from junior ED physicians that they often did not attend the ED department meetings because these meetings were usually held for senior ED physician and nursing leaders to discuss administrative matters. It was therefore hoped that dedicated sessions for junior ED physicians would help improve attendance rates. These CME activities took the format of didactic lectures on acute asthma management in the ED with emphasis on the GINA clinical practice guidelines pertaining to discharge management in the ED. Before and after lecture multiple-choice question quizzes were administered to facilitate retention of information. They were scheduled to coincide with the periods of following junior ED physician staff turnover.
Further sustained improvement in terms of compliance to clinical practice guidelines was observed in patients who were referred to the A-CARE nurse. Unfortunately, we observed that the referral rate to the A-CARE per night fell further (figure 3) and we implemented an independent clinical audit from September 2018 to January 2019 in order to measure the proportion of patients with asthma who were not referred to A-CARE. Through this clinical audit, we found that only 13.7% of all ED patients with a diagnosis of asthma were referred to the asthma nurse (table 1). The QI team sought feedback from informal channels through our ED physician team members and found that the overall interest and engagement of the ED healthcare staff had waned with time. Existing ED healthcare providers expressed frustration when they were unsuccessful in making a referral because the A-CARE nurse was not on duty every night. Our ED physician team member was also on maternity leave during this period and we lost a valuable ‘ED asthma champion’ in the interim. While it was hoped that we would be able to reach out to junior ED physicians through dedicated CME sessions, we observed that the attendance rate was modest at best. Most junior physicians perform rotations of 3–6 months in the ED and most junior ED physicians who were present in PDSA cycle 1 were no longer present in the ED at the time of PDSA cycle 2. This was also an important non-modifiable barrier towards behaviour change in the ED.
Clinical characteristics of all asthma visits to the ED, September 18 to January 19 (n=637)
Results
Baseline clinical characteristics
Two hundred and forty-seven patients with a diagnosis of asthma were seen by the A-CARE nurse from September 2017 to January 2019. Ninety-seven patients (39.3%) were seen by the A-CARE nurse on more than one patient visit for a total of 273 patient encounters with the A-CARE nurse. Approximately one-third of patients reported that they were current smokers, did not have any routine follow-up for asthma or non-compliant to their inhalers (table 2). 82.1% did not receive any prior asthma counselling. Approximately one-third of patients were not receiving any form of controller therapy and 39.3% had two or more ED attendances in the past year for asthma.
Clinical characteristics of 247 patients with asthma reviewed by A-CARE, September 17 to January 19
Overall QI outcomes
The baseline rates for adherence to OCS prescription, ICS initiation and issuance of outpatient follow-up review were determined in the months of September 2017 and October 2017 and they were found to be 58%, 27% and 69%, respectively. Following implementation of PDSA cycles 1 and 2, the target of attaining at least 80% compliance to OCS prescription and issuance of outpatient follow-up review was achieved in patients seen by the A-CARE nurse, but not for ICS prescription (figure 3). The median adherence rate at the conclusion of the project in January 2019 was 86%, 67% and 92% for OCS prescription, ICS initiation and issuance of outpatient follow-up review, respectively. The referral rate to the A-CARE nurse however remained low over two PDSA cycles with a referral rate of 0.52 patient per night in December 2018 and January 2019.
A clinical audit comparing outcomes of all patients presenting to the ED for asthma (with and without asthma counselling by the daytime asthma nurse or A-CARE nurse) was subsequently performed in PDSA cycle 2. The electronic medical records of all patients who were seen in our ED with a primary diagnosis of asthma from September 2018 to January 2019 were analysed (table 1). A total of 637 ED visits for asthma were recorded and 337 (52.9%) of ED disposition decisions occurred after-hours from 18:00 to 08:00 hours. Asthma counselling was delivered for 87 (13.7%) ED visits. Three hundred and thirty-three (52.3%) of ED visits did not require hospitalisation and were discharged from the ED. ED physicians were given reminders by the A-CARE nurse to refer discharged patients back to their usual asthma care provider (general practitioner or respiratory specialist) for outpatient follow-up. If patients did not have any usual asthma care provider, ED physicians were advised to refer them to our respiratory specialist clinic. We tracked the attendance rate of 81 patients who were referred to our respiratory specialist clinics. In the latter group, statistically higher rates of follow-up attendance rates were observed in patients who received asthma counselling compared with those who did not (41.7% vs 15.9%, p=0.0388).
Discussion
This study has demonstrated improvements in the quality of asthma care in the ED with the introduction of an after-hours asthma nurse service. A sustained level of adherence to OCS prescription and issuance of outpatient follow-up review of at least 80% was achieved in patients who were reviewed by the A-CARE nurse. In addition, among the patients who were referred to our respiratory clinics, higher attendance rates were achieved in patients who received asthma counselling compared with patients who were not. An improvement in ICS initiation (from 27% to 67%) was demonstrated although the target level of 80% was not met.
A significant proportion of ED visits for asthma can be prevented.24 In addition to disease severity, various potentially modifiable factors have been described, including inadequate supply of inhaled medications,1 25 lack of asthma education,26 lack of a written asthma action plan,27 lack of follow-up asthma care,20 poor inhaler technique and active smoking status.28 As reported in our study and internationally around the world, many patients lack formal asthma education.29 Therefore, specialist nurses are uniquely suited to close the gap by providing education on self-management and inhaler device training.30–32 The ED is often a challenging environment for the delivery of asthma counselling services due to overcrowding, background noise and ongoing symptoms of an asthma exacerbation, thus posing difficulties for patients with asthma to retain and process information from asthma counselling.
While it may not be optimal to deliver asthma education to a patient with an active exacerbation in the ED, it may be the only opportunity to do so for some patients. Our study found that the majority (74.9%) of patients seen by our A-CARE nurse after-hours lacked prior asthma counselling. We observed that half of asthma visits occurred after-hours in our ED. These patients would have otherwise lacked access to asthma counselling if asthma counselling services were unavailable after-hours. The lack of self-management education and non-issuance of a written asthma action plan has been shown to increase the likelihood of repeat ED attendance.27 This is an important gap in asthma care that continues to drive unplanned acute healthcare usage. In addition, approximately one-third of patients reported either a history of treatment non-compliance or active smoking status. These patients represent a ‘captive audience’ who could potentially benefit from even brief counselling on the importance of taking regular controller treatment and self-management strategies together with written information.33 In terms of measurable outcomes, asthma education has been shown to be cost-effective34 and ED-directed educational interventions have been shown to improve primary care follow-up for adults seen in the ED for asthma.34,35
Opportunities to optimise asthma medical therapy were also found in a significant proportion of ED patients seen by our A-CARE nurse. We found that approximately one-third of patients were not on any regular controller inhalers and one-third did not have any prior regular asthma follow-up. This represents a critical gap in asthma care to be urgently addressed via better implementation of quality asthma care. Failure to provide ICS controller medication and follow-up assessment have been consistently cited as avoidable factors in national audits of patients with fatal or near-fatal asthma in Singapore36 and internationally,37 38 and our study has shown that it is possible to address them with extended availability of specialist asthma nurse counselling after-hours.
Limitations
This study however has several potential limitations. First and most importantly, only 16% of all after-hours ED visits for asthma were referred to our A-CARE nurse. This was partially because the pilot A-CARE service was available for only 3 days per week instead of a daily service. Some degree of buy-in from ED physicians was lost when they tried to mistakenly make referrals on nights when A-CARE was not available. More importantly, the A-CARE referral rate from ED physicians was suboptimal. Although efforts were made to improve the referral rate to A-CARE, the nightly referral rate remained low and this significantly limited the impact of A-CARE. Although we attempted to address this via a case-finding approach in PDSA cycle 2, this strategy had to be abandoned subsequently from September 2018 onwards due to increased institutional restrictions on accessibility of electronic medical records. Second, our study was also limited by our method of data collection, which was dependent on referral rates to our A-CARE nurse and the subjective entry of the diagnosis of asthma by ED physicians. Third, our study relied on retrospective data collection from a single centre with limited sample size and the findings may not be generalisable to other EDs at large.
Lessons learnt: the unique challenges of implementing QI in the ED
It has been said that changing the behaviour of physicians is as difficult as that of patients, and merely informing physicians of the benefits and standards of care alone is unlikely to reach sustained adherence.39 This is particularly true in the ED setting, where organisational and cultural factors feature prominently in hindering QI.40 Despite various attempts to improve the quality of asthma care in EDs around the world,41 enduring challenges are likely to remain due to the high-paced and unpredictable nature of the emergency care. ED physicians are frequently under the competing pressures of heavy workloads and overcrowding,42 frequent interruptions at work,43 and the need to multitask,44 and many experience occupational stress and burnout.45 In addition, the exigencies of attending to the medical emergencies may contribute to reduced emphasis and prioritisation of resources on good holistic asthma care.
In our ED, junior ED physicians are often ultimately responsible for making the referral to the A-CARE nurse, issuing medication prescriptions and arranging for outpatient follow-up after discharge from the ED. Although A-CARE received broad support from senior ED physician leaders in our hospital, we were unsuccessful in engaging junior ED physicians and this was perhaps the most important factor underlying the low referral rate to the A-CARE nurse.
We attempted to raise awareness on the A-CARE QI project via traditional platforms such as the ED department meetings or via mass emails. While this ‘top-down’ approach was successful in reaching out to senior and permanent ED physicians, organisational constraints meant that the message was ultimately delivered to few junior ED physicians. Front-line junior ED physicians gave informal feedback that they were often unable to attend the face-to-face briefing sessions as they were either on active clinical duty or that they preferred to rest at home before or after their ED shift. Some junior physicians also missed the briefings as they were only performing a short rotation through the ED as part of their training. At an individual level, it was challenging to keep junior ED physicians continually engaged. Some junior physicians were rotating through the ED as part of their specialist training programme and had a low level of interest towards what was viewed as primary care for asthma rather than holistic ED asthma care. There was also a low level of buy-in from junior ED physicians, some of whom expressed having ‘ED protocol burnout’ and who saw A-CARE as yet another administrative task that added to workload without providing tangible improvements.
Future steps ahead
Drawing on the lessons learnt from PDSA cycles 1 and 2, we have plans to broaden stakeholder involvement in subsequent PDSA cycles to empower ED nursing staff to initiate referrals to A-CARE in accordance with a nurse-led written ED asthma protocol. This is in line with efforts to implement more nurse-led interventions in our ED, such as early administration of bronchodilators for patients who are asthmatic at triage and nurse-initiated analgesia for patients with pain. Key process steps in healthcare delivery in the ED are often ‘bottlenecked’ at the level of busy ED physician and delegation of tasks to senior ED nurses would help improve the timeliness of the various process steps. We hope to overcome the limitation of low A-CARE referral rates from ED physicians by doing so. Additionally, as ED nurses comprise largely of permanent staff, it is anticipated that QI interventions targeting ED nurses would overcome the effects of regular junior ED physician turnover and raise sustainability. Finally, the QI team aims to identify and engage experienced ED nurses for training in asthma counselling so that daily round-the-clock asthma counselling services can be upscaled in the future.
Conclusions
A significant proportion of patients present to the ED after-hours for acute asthma and many patients were found to lack regular controller therapy, follow-up for asthma, or were non-adherent to their inhalers or currently still smoking. Opportunities to optimise the management of patients with asthma in the ED therefore exist which could be addressed by high-quality asthma care. Additionally, several gaps in the ED care pathway for asthma were found. A pilot after-hours asthma nurse service was thus implemented as a QI project and achieved the target of 80% adherence rates to the prescription of OCS and issuance of outpatient follow-up for patients discharged from the ED but fell short of target for prescription of ICS. Although sustained improvements in the adherence rates to GINA guidelines were achieved in patients reviewed by A-CARE, they were limited in overall impact due to suboptimal referral rate. We plan to improve the quality of asthma care by implementing further PDSA cycles to increase the referral rates to A-CARE.
Acknowledgments
The authors acknowledge the efforts of the team of asthma nurses and the quality improvement coaches of the Department of Process Transformation and Improvement of Singapore General Hospital for their contributions to this project.
References
Footnotes
Contributors MSK designed the study. JYLL, AKWC, SYC, JJC, KBKT and MSK conducted the study and operationalised A-CARE. JYLL performed data collection which was analysed by SYC, AKWC, JJC, KBKT and MSK. The manuscript was drafted by JYLL, SYC and MSK. AKWC, JJC, KBKT, BA and DT gave critical revision of the manuscript. All authors read and approved the final manuscript, and take responsibility for the integrity of the data.
Funding The A-CARE programme was supported by a grant from AstraZeneca Singapore to the Singapore General Hospital.
Disclaimer AstraZeneca Singapore had no role in study design, data collection and analysis.
Competing interests AKWC has received speaking fees and honorarium from AstraZeneca and GlaxoSmithKline, all paid to his hospital, Singapore General Hospital. DT and BA are employees of AstraZeneca Singapore. MSK has received speaker fees and fees for serving on the advisory boards of GlaxoSmithKline, AstraZeneca and Sanofi, all paid to her hospital, Singapore General Hospital. The other authors do not have competing interests to declare.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Ethics approval Waiver of ethical approval was granted by our Institutional Review Board. The work was deemed a service improvement project and not a research study on human subjects.
Provenance and peer review Not commissioned; internally peer reviewed.
Data availability statement All data relevant to the study are included in the article.