Article Text

Abstract
Background: Construction workers exposed to silica-containing dust are at risk of developing silicosis even at low exposure levels. Health surveillance among these workers is commonly advised but the exact diagnostic work-up is not specified and therefore may result in unnecessary chest x ray investigations.
Aim: To develop a simple diagnostic model to estimate the probability of an individual worker having pneumoconiosis from questionnaire and spirometry results, in order to accurately rule out workers without pneumoconiosis.
Methods: The study was performed using cross-sectional data of 1291 Dutch natural stone and construction workers with potentially high quartz dust exposure. A multivariable logistic regression model was developed using chest x ray with ILO profusion category ⩾1/1 as the reference standard. The model’s calibration was evaluated with the Hosmer–Lemeshow test; the discriminative ability was determined by calculating the area under the receiver operating characteristic curve (ROC area). Internal validity of the final model was assessed by a bootstrapping procedure. For clinical application, the diagnostic model was transformed into an easy-to-use score chart.
Results: Age 40 years or older, current smoker, high-exposure job, working 15 years or longer in the construction industry, “feeling unhealthy” and FEV1 were independent predictors in the diagnostic model. The model showed good calibration (a non-significant Hosmer–Lemeshow test) and discriminative ability (ROC area 0.81, 95% CI 0.74 to 0.85). Internal validity was reasonable; the optimism corrected ROC area was 0.76. By using a cut-off point with a high negative predictive value the occupational physician can efficiently detect a large proportion of workers with a low probability of having pneumoconiosis and exclude them from unnecessary x ray investigations.
Conclusions: This diagnostic model is an efficient and effective instrument to rule out pneumoconiosis among construction workers. Its use in health surveillance among these workers can reduce the number of redundant x ray investigations.
- HRCT, high resolution computed tomography
Statistics from Altmetric.com
Silicosis is an interstitial lung disease caused by inhaled crystalline silica that is incurable and may be progressive even after exposure has ceased.1 Chronic silicosis is the most common, and typically occurs after 10 years of exposure to relatively low levels of silica. Decrements in lung function or respiratory symptoms are not likely in the early stages of simple silicosis.2 In the more advanced cases, both obstructive and restrictive lung function effects, as well as decreased diffusion capacity, are more common. The International Agency for Research on Cancer has classified silica as a Class I human lung carcinogen.3 Cancer mortality risk varies, but appears to be highest in smoking workers with silicosis.4 Chest radiography is the diagnostic investigation in which silicosis is presented with small rounded opacities in the upper and mid zones of the lung. In the construction industry, where quartz exposure arises from drilling, milling, grinding and demolition work, silicosis often goes unrecognised.5
Recent research indicates that silicosis of grade 1/0 and 1/1 will still occur under current dust standards. Even at the proposed level of 0.05 mg/m3 the incidence rate of silicosis 1/1 (small rounded opacities) or greater would be about 10%–20%. It has been calculated that a permissible exposure level of less than 0.001 mg/m3 may be required to prevent mild radiographic changes (ILO profusion of ⩽1/0) after a lifetime of silica exposure.2 Therefore, health monitoring to detect early signs of disease among workers exposed to silica-containing dust is needed.
Guidelines for silicosis surveillance have been published and in general involve questionnaires, physical examination, and additional tests like spirometry and chest x ray.6–9 The latter test is obviously more burdensome and costly to execute. The questionnaires are simple to apply and may include useful information for selection of individual workers that are at higher risk of having silicosis and therefore could be included in health surveillance programmes. Nevertheless, none of the available protocols for silicosis surveillance specifies the exact diagnostic work-up for workers suspected of having silicosis. For instance, it is widely agreed that questionnaires on occupational and medical (respiratory) history should be collected before one can continue to the next step in the diagnostic work-up. However, it remains unclear which question provides the best diagnostic information on the presence or absence of silicosis. Further, it is not clear who needs to undergo or who can be excluded from further evaluations.
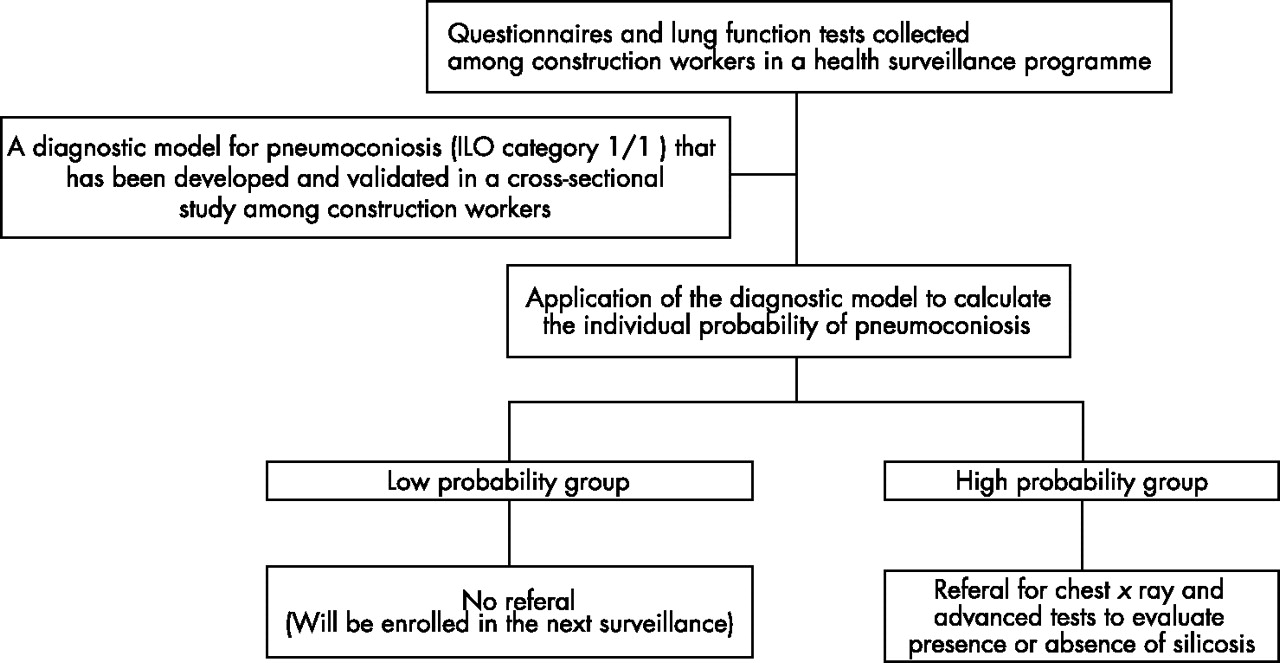
Multivariable diagnostic prediction models, which consist of simple questions or tests, are often used to rule in or out a certain target condition to avoid unnecessary burdening and costly procedures.10,11 We aimed to develop such simple diagnostic model for ruling out pneumoconiosis among construction workers at risk of having silicosis. We therefore used ILO profusion category ⩾1/1 as the reference test. Multivariable logistic regression modelling was used to quantify the independent contribution of different questions and diagnostic tests.10 Figure 1 illustrates how such model may be applied as a screening instrument in silicosis surveillance. It would enable the occupational physicians to discriminate workers with low probability of pneumoconiosis who do not need further medical investigations. This would obviously increase the efficiency of the surveillance, as it decreases the number of unnecessary chest x rays.

{kind=link}
An approach for silicosis surveillance.
METHODS AND MATERIALS
Study design and population
We used data from a cross-sectional study among Dutch natural stone and construction workers age 30 years and older.12 In 1998, 4173 workers with expected high cumulative exposure to quartz-containing dust registered in the natural stone association and nationwide construction workers database were invited to participate in the study. A questionnaire and invitation to the medical evaluation were sent to the eligible respondents’ homes (n = 1690); and 1335 (32% of those invited) were enrolled. Examinations took place in five locations distributed over the country and consisted of a questionnaire on respiratory symptoms and work history, lung function measurements and chest x ray (reference standard). All participating workers signed an informed consent for use of the test results for scientific research. The medical ethics committee of the university approved the study and all procedures were in agreement with European legal requirements with regards to privacy, data storage and use of x ray equipment.
Questionnaire
The prevalence of respiratory symptoms was ascertained with a self-administered questionnaire derived from the British Medical Research Council Respiratory Questionnaire.13 Respiratory symptoms were considered present if during the preceding two years the symptoms lasted for at least three months. Chronic cough was interpreted as either productive or non-productive cough. Shortness of breath was defined as ever being short of breath when walking with people of the same age at normal pace on level ground. Frequent wheezing was defined as wheezing for more than one week in the preceding two years. We added questions on whether the participants ever had, or have been told that they had, certain respiratory diseases (such as emphysema, pleuritis or tuberculosis), as well as questions on smoking and occupational history. A self-rated health question, “How would you assess your recent health condition?”, with the answer choices of “healthy” and “unhealthy”, was also included.
Silica exposure assessment
A cumulative exposure index was available for every worker.12 This exposure proxy was a semi-quantitative measure of the cumulative exposure to silica, which was calculated by multiplying the duration of exposure by an expert exposure index. Three industrial hygienists, with experience in exposure assessment among construction workers, classified 36 different jobs on a 10-point scale for quartz exposure. The median score of the three experts, weighted for all consecutive and multiple jobs, was used to rank the different past and present occupations of the construction under study. The duration of exposure was calculated by summing up the years worked in jobs with potential mineral dust exposure in the construction industry.
Lung function measurements
Lung function was measured with a pneumotachometer (Masterscreen Pneumo, Jaeger Benelux, Breda, the Netherlands) on the same day as the chest radiographs. The pneumotachometer measures the forced expiratory flow. Trained technicians performed the lung function measurements.14
Lung function data were compared with the European Respiratory Society reference values. To compare the actual to the reference lung function levels, we used the standardised residuals (standardised residual = (observed − predicted)/ residual standard deviation). This dimensionless index indicates how far the observed value is removed from the predicted value, and, therefore, how likely it is that the observed lung function occurs in the reference population.15
Diagnostic outcome (reference standard)
Chest x ray indicative for pneumoconiosis (ILO profusion category ⩾1/1) was used as the reference standard. The chest radiograph has long been the cornerstone in the diagnosis of silicosis, and the ILO guidelines state that the classification system is to be used for epidemiological survey and routine surveillance of dust-exposed workers.16
Posterior-anterior chest x rays from all individuals were taken in a mobile x ray unit and read independently by three National Institute of Occupational Safety and Health (NIOSH, Morgantown, USA) “B” readers, according to the ILO guidelines for classification of pneumoconiosis.16 Profusion score and the predominant shape of the opacities were recorded. Median results of the readings were used.
Data analysis
We first assessed the univariable association between each predictor and the presence of the outcome with binary logistic regression analysis. We also examined whether continuous variables (age, lung function, and cumulative exposure index and total working years) could be transformed into simple categorisations. Cut-off values for categories were chosen based on restricted cubic spline functions, provided in S-Plus version 2000 (Mathsoft, Inc, Seattle, WA, USA), at the point where the function showed a change in risk of the outcome.17 Model χ2 of the models with the continuous and categorised variables were compared to see whether the categorisations were reasonable. To evaluate the association between job titles and the diagnostic outcome, we first assigned one job title for each worker. Workers who had more than one job title (n = 256) were assigned to a job title with the highest expert exposure index.12 As this resulted in 36 job titles, we further clustered the job titles based on the expert exposure index. We finally evaluated the univariable association between the clustered job titles and outcome; those with similar regression coefficients were finally grouped into two groups (high vs low exposed) for convenience in practice.
We then fitted a multivariable logistic regression model including all potential predictors from the questionnaire and spirometry, based on a univariable p value of <0.50. Secondly, we used a backward stepwise procedure (using p<0.15 for inclusion) to select a final model with the strongest predictors for absence (or presence) of pneumoconiosis.17 Extra analysis was performed to compare the diagnostic performance between the final model with all continuous variables preserved in their original form, and with these variables in dichotomised form.
The diagnostic accuracy of the final model was quantified using calibration and discrimination measures. Calibration, the agreement between the predicted probabilities and the observed frequencies of having abnormal chest x ray indicative for pneumoconiosis, was assessed graphically and tested with the Hosmer–Lemeshow test (where p⩾0.10 reflects good agreement). The discriminative ability was determined with the area under the receiver operating characteristic (ROC) curve. The area under the ROC curve (ROC area) shows the relation between false positive rate (1-specificity) and true positive rate (sensitivity). The ROC area can range from 0.5 (no discrimination) to 1.0 (perfect discrimination). The ROC area reflects the probability that for all possible pairs of workers, in which one worker has pneumoconiosis and one has not, the model indeed assigned a higher probability of having pneumoconiosis to the worker with pneumoconiosis.18
We used bootstrapping to assess the internal validity and the amount of overfitting of the model. This bootstrapping procedure gives a correction factor for both the model’s ROC area and for the regression coefficients of the predictors in the final model.19 The regression coefficients of the predictors in the final model were multiplied by this correction factor to prevent the model from yielding optimistic predictions when applied in future (new) workers.
To facilitate application of the final model in practice, the corrected regression coefficients of the predictors in the final diagnostic model were converted to easy-to-use numbers. To derive these numbers, the corrected coefficients were divided by the smallest one, and rounded to the nearest half integer. The discriminative accuracy of this scoring rule was again assessed. Finally, the sums of the scores were related to their corresponding probabilities of having (a chest x ray indicative for) pneumoconiosis. Finally, a cut-off point of the sum scores was introduced to divide the worker population into group with low versus high probability of having (chest x ray indicative for) pneumoconiosis.
Of 1335 available individual data, 44 workers with a missing outcome (chest x ray result) or with a completely missing questionnaire were excluded, leaving n = 1291. Of these, 58 participants (4.5%) had 77 missing values. Although participants with missing values showed similar characteristics as those who had complete values, deletion of subjects with a missing value (so called “complete case analysis”) may still lead to biased result and certainly a loss of power.20 Therefore, we imputed the missing values by using the linear regression method (with addition of an error term) in SPSS 11.5 for Windows (Statistical Products and Service Solution, Inc, Chicago, IL, USA). The imputation was based on the correlation between each variable with missing values and all other variables as estimated from the 1233 (95.5%) complete dataset; yielding 1291 complete data for further analyses.
RESULTS
Population characteristics
ILO profusion categories ⩾0/1, ⩾1/0, and ⩾1/1 were found in 426 (33.0%), 131 (10.1%), and 37 (2.9%) workers, respectively. Of 426 x rays with profusion category ⩾0/1, we found 38 (8.9%) with primary and 45 (10.6%) with secondary rounded opacities. Table 1 shows that workers with ILO profusion category ⩾1/1 were older, worked longer in the construction industry, had higher cumulative exposure index, and had worse lung function. This group also showed higher percentages of current smoker and workers who felt unhealthy.
General characteristics and univariable association with the outcome
The restricted cubic spline functions clearly showed an increase in risk of having x ray indicative for pneumoconiosis at age of 40 years or older, working in the construction industry 15 years or longer, a cumulative exposure index of 10 or higher, and a standardised residual FEV1 ⩽−1.0. The model χ2 of the continuous versus dichotomised variables for age, working years, cumulative exposure index, and standardised residual FEV1 were 12.6 versus 10.2, 14.1 versus 9.5, 13.2 versus 10.1, and 7.8 versus 8.2, respectively. Working 15 years or longer in the construction industry significantly increased the probability of pneumoconiosis by almost four times (OR 3.7), and workers over 40 years or having a decreased lung function had triple the probability of pneumoconiosis (see table 1).
Model development
The initial multivariable model included seven questionnaire predictors (univariable p values ⩽0.50; table 1). Of these, only five—that is, age 40 years or older, current smoker, high exposed job title, working 15 years or longer in the construction industry, and “feeling unhealthy” —appeared independently (p<0.15) related to the presence or absence of pneumoconiosis (table 2, first column). Table 2 also shows that the cumulative exposure index did not give additional value to the diagnostic information provided by the five questionnaire items; the odds ratio of the cumulative exposure index was far from significant and the ROC area of both models were the same (second column). Addition of the lung function to the reduced questionnaire model (third column) slightly increased the ROC area (delta ROC area of 0.02) and significantly increased the model χ2 of the questionnaire model (deviance = 7.8, df = 1, p = 0.005). The calibration plot of the reduced questionnaire + lung function model showed good calibration, confirmed by a non-significant Hosmer–Lemeshow test (p = 0.20). Therefore, the questionnaire + lung function model was chosen as the final model. The bootstrapping procedure yielded a correction factor of 0.82 for the regression coefficients of the final model, which indicated a reasonable internal validity. The corrected AUC was 0.76 (instead of 0.81).
The strength of the predictors for chest x ray indicative for pneumoconiosis (ILO profusion category ⩾1/1)
There was no significant difference in the diagnostic performance between the model with all continuous variables preserved in their original form and the model with dichotomised variables. The model with continuous variables showed model χ2 of 44.0 with 6 degrees of freedom, ROC area of 0.809, and Hosmer–Lemeshow test p = 0.514, whereas model with dichotomised variables showed model χ2 of 44.9 with 6 degrees of freedom, ROC area of 0.805, and Hosmer–Lemeshow test p = 0.465.
Score chart
After multiplication by the correction (shrinkage) factor obtained from the bootstrapping procedure, the corrected regression coefficients of the independent predictors of the final model were converted into a simple-to-use score system or score chart (table 3). The predictive accuracy of this scoring system was good; p value of the Hosmer–Lemeshow test was 0.39 and the ROC area was 0.787 (95% CI 0.729 to 0.845). Using the adjusted regression coefficients from table 2 (see formula in table 2 footnotes), we calculated the predicted probabilities of pneumoconiosis corresponding to the different sum scores (table 3, lower part). As an example how to use this chart, a 45-year-old non-smoking concrete driller who worked in the construction industry for 10 years, felt healthy, but had a standardised residual FEV1 of −1 would have a sum score of 3.75 (1+0+1.5+0+0+1.25). This corresponded to a probability of pneumoconiosis of 2%.
Diagnostic model for chest x ray indicative for pneumoconiosis and the corresponding predicted probability
Table 4 displays the diagnostic accuracy parameter plus the corresponding proportions of the detected pneumoconiosis cases and unnecessary referrals for each sum score threshold. For example, using the sum score threshold of 3.75 or higher as cut-off point for referral for chest x ray, one refers 567 (43.9%) workers. As the aim of our model was to rule out pneumoconiosis, the negative predictive value was 99.4% (720/724) and the likelihood ratio of a negative test (LR-) was 0.2 ((4/37)/(720/1254)). For comparison, not using the model and referring all workers for chest x ray would in fact result in 1254 unnecessary negative x rays (as only 37 had a positive x ray).
The diagnostic accuracy across different cut-off points for referral for chest x ray investigation
DISCUSSION
Our study shows that the diagnostic model for pneumoconiosis ILO profusion category ⩾1/1 effectively rules out pneumoconiosis and reduces a substantial number of unnecessary referrals for chest x ray investigations.
The main motivation for (multivariable) diagnostic research is to determine whether simple diagnostic tests already predict the presence or absence of the target disease without having to perform the more invasive and costly reference test, with acceptable misclassifications. The motive of diagnostic research is simply to decrease patient burden and healthcare expenses and by no means to explain causality.10,11 In our study, we focused on optimal prediction of the absence of pneumoconiosis in order to decrease unnecessary x ray referrals.
Diagnostic studies are inherently cross-sectional, and the test results under study are commonly not causal factors (that is, not part of the causal pathway). In fact, most test results are actually the consequence of disease presence. This explains the inclusion of the variables “feeling unhealthy” and “current smoker” in our final diagnostic model. These associations thus do not necessarily express a causal relation between smoking and pneumoconiosis. We only used the information carried by the smoking habit to estimate the probability of having a positive x ray. The odds ratio of 2.4 for current smoker only means that current smokers, compared to non-smokers, have 2.4 times higher probability of having a positive x ray, without any reference to causality. The odds ratio for “feeling unhealthy” should also be interpreted as: workers who feel unhealthy have 2.8 times higher probability of having a positive x ray than workers who feel healthy. Furthermore, “feeling unhealthy” as a global assessment of an individual’s health perspective, although not disease specific, has also been proven to be an independent and strong predictor of mortality in community studies.21
The selected predictors in our diagnostic model, including age and declining lung function, have been mentioned in previous studies.5,22–25 Here again, age is not a causal factor, but rather captures information about duration of exposure and potential progression of disease and thus has independently contributed to the prediction of pneumoconiosis.
Some intuitive predictors such as work duration and job with high exposure to silica containing dust were selected in our model as well. The cumulative exposure index indeed showed a significant univariable association with a chest x ray result that was indicative for pneumoconiosis. However, adding this variable to the multivariable model that already included work duration and job title did not improve the predictive accuracy of the model. Apparently, its information (that was reflected in the univariable analysis) was already provided by work duration and job title. Several exposure studies indeed demonstrated that the number of years of working in the construction industry could be used as a surrogate measure for cumulative exposure to silica.4,26 The high exposure job consisted of job titles with high quartz exposure level and, therefore, could be considered a proxy for exposure as well.9
We chose ILO profusion category ⩾1/1, as an abnormal chest x ray indicative for pneumoconiosis, as our reference standard. Choosing profusion category ⩾1/0 would lead to defining a category in which the absence of small opacities was seriously considered. This would result in significantly more misclassification. Plain chest radiographs may be insensitive to early changes of the lung parenchyma. High resolution computed tomography (HRCT) is superior to chest x ray in identifying early parenchymal lesions.27 Nevertheless, codifying abnormalities according to ILO classification by conventional radiographic assessment remains the first diagnostic step in epidemiological studies and in health surveillance programmes of dust-exposed workers.16 Besides, the increased radiation dose, as well as the added expense and time involved, do not justify the use of HRCT for surveillance.
Silicosis occurrence is not surprising among workers exposed to silica-containing dusts in various industries and occupations. Patients may be free of symptoms with abnormalities identified by chest x ray during medical screening. However, regarding the low prevalence, it is not efficient to perform a chest x ray as a routine test in the population at risk because this will yield many avoidable negative outcomes.
Our diagnostic prediction model can be applied by the occupational physician to decide whether a worker should have a chest x ray investigation or not. For groups of workers with low probability, there will be no further action. They will be enrolled in the next surveillance round. For groups of workers with a high probability, they should be referred for chest x ray and possibly advanced medical tests (that is, diffusion capacity and HRCT) to confirm the presence or absence of pneumoconiosis or silicosis.
The diagnostic model showed good diagnostic accuracy (calibration, discrimination, and internal validity). However, to use it as a screening tool, one should carefully choose the cut-off point above which workers should be referred for chest x ray. Screening must lead to a high level of case detection (high sensitivity), and at the same time a reasonably low level of unnecessary x ray referrals. So, the choice of a cut-off point must be based on an acceptable proportion of missed cases and of unnecessary referrals. As shown in table 4, a higher cut-off leads to a lower sensitivity but at the gain of investigating fewer workers. Policy makers should, therefore, balance the number of missed cases with the cost reduction gained by minimising the number of referrals for advanced diagnostic tests. For example, not referring workers with sum scores lower than 4.75 will save the expense of unnecessary chest x rays in up to 80% of the subjects. This cut-off point also has a high negative predictive value of 98.4%, which means that more than 98% of those who are not referred would indeed have a negative chest x ray (if tested). However, 16 of all 37 cases will be missed. Given the slowly progressive nature of the disease and the fact that surveillance is repeatedly conducted overtime, we could expect that the missed cases would be captured in the next surveillance. However, if the aim is to detect as many cases as possible, this cut-off value will not be the first choice. One then might use a lower cut-off point to reduce the number of missed cases. For instance, a sum scores of 3.0 or higher yields 100% sensitivity, which means that all cases will be captured, but at the expense of referring half of all workers. A cut-off point in between the earlier discussed options is 3.75, with 89.2% sensitivity, 99.4% negative predictive value, and not referring 56.1% of all workers. In doing so, the use of this diagnostic model as an initial screening instrument will surely increase the efficiency of health surveillance in construction workers.
The small number of cases relative to the high number of potential predictors studied is the limitation of our analysis. For diagnostic studies, no exact formula for sample size calculation exists. However, the general rule is that per candidate predictor variable there should be at least 10 events (1 to 10 rule).28 We had nine candidate predictors with 37 cases (ratio 1:4). When limited positive cases are available to develop a model, statistical methods such as the bootstrapping procedure should be used to check whether a developed model is reasonably valid or needs to be adjusted. This procedure has been shown to be superior to split-sample or cross-validation methods.28 It turned out that the model had a reasonable internal validity (we obtained a correction factor of 0.82; the closer the correction factor is to 1, the less optimism). Nevertheless, an external validation in a new population is required to confirm the performance of the model and its transportability into all construction workers. Another important point from the modelling aspect is the dichotomisation of various continuous variables. Dichotomisation increases the potential for misclassification and we may lose important information conveyed by a variable.17 Nevertheless we dichotomised those variables for reason of simplicity in practice. The cut-off values were chosen based on restricted cubic spline function, at the point where the function showed an observable change in risk of the outcome.17 Additional analysis showed that the model χ2 of both forms were comparable and there was no significant difference in the diagnostic performance between the model with all continuous variables preserved in their original form and the model with dichotomised variables.
In conclusion, we derived a diagnostic model for pneumoconiosis that can be applied in health surveillance on a large scale in natural stone and construction workers. The model comprises simple questionnaire items and routine lung function, which are widely available in occupational health settings. With our approach, the efficiency of health surveillance can be increased considerably by decreasing a large number of unnecessary referrals for chest x ray investigations. However, external validation of the model is recommended before it can be used with confidence in all construction workers.
Main messages
-
A diagnostic model for pneumoconiosis ILO profusion category ⩾1/1 was developed and shown to be an efficient and effective instrument to rule out pneumoconiosis among construction and natural stone workers.
-
Its use in respiratory health surveillance among these workers could minimise the number of redundant x ray investigations by excluding workers with a low probability of having pneumoconiosis.
-
For screening purposes a balance between cost reduction gained by reducing the number of investigations and the acceptable misclassification rate should be considered in the determination of the cut-off point.
Policy implications
-
By using diagnostic modelling, pneumoconiosis could be quantified more accurately than can be expected from the traditional surveillance approach.
-
For health surveillance policies in silica-exposed workers the application of diagnostic models can reduce unnecessary x ray investigations by estimating the individual probability of having pneumoconiosis.
Acknowledgments
We acknowledge ARBOUW, the Dutch National Institute for Safety and Health in the Construction industry, for funding and supporting this study. We thank Peter S Thorne for reviewing the manuscript.
REFERENCES
Footnotes
-
Published Online First 4 April 2007
-
Competing interests: None declared.