Article Text

Abstract
OBJECTIVES To characterise diving exposure and pulmonary function in professional divers at the start of their formal education and during the first 3 years of their professional career.
METHODS The study included 87 men at the start of their education as professional divers. At follow up 1 and 3 years after the school 83 and 81 divers respectively were re-examined. Assessment of lung function included dynamic lung volumes and flows and transfer factor for carbon monoxide (TlCO).
RESULTS 69 Divers had preschool SCUBA diving experience and had a median number of 70 dives (range 2–3000) to a median maximal depth of 40 (range 10–73) metres. During the 15 week introductory diving course, they had 44 dives (range 38–50) in the depth range 10–50 metres. The median number of dives over the follow up period was 95 (range 0–722) to a maximal median depth of 38 (range 0–98) metres. At the start of the diving course there were no differences in forced vital capacity (FVC), forced expired volume in 1 second (FEV1), and in TlCO between the 69 pre-exposed divers and the 18 never exposed divers. The FVC was significantly larger than predicted in both groups. At follow up at 3 years there was a significant reduction in mean (SD) FEV1 of 1.8% (6.5), in forced mid-expiratory flow rate (FEF25–75%) of 6.5% (11.7) and in forced expiratory flow at 75% of FVC expired (FEF75%) of 10.4% (16.8). There was no change in FVC. The TlCO was significantly decreased by 4.6% (8.8). No significant effects were found of cumulative diving exposure, including the number of dives, on the relative changes of any of the lung function variables.
CONCLUSIONS The results indicate that divers initially belong to a selected group with large FVC. Exposure to diving may contribute to changes in pulmonary function, mostly affecting small airways conductance.
- diving
- follow up study
- pulmonary function
Statistics from Altmetric.com
Former cross sectional studies have shown that divers have larger lungs than predicted.1-3 Crosbieet al 2 described a positive correlation between increased forced vital capacity (FVC) and exposure to diving up to the age of 30 years with a following decline of FVC despite continued diving. In a later study, no difference in vital capacity was found between divers, policemen, offshore workers, and the general Scandinavian population.4 In the earlier studies,1-3 the forced expired volume in 1 second (FEV1) was not increased in proportion to the increase in vital capacity, giving a low FEV1/FVC ratio. The later study4 showed a reduction in FEV1 which correlated with the cumulative exposure to diving. This pattern of characteristics of lung function could be due to a selection of subjects with large lungs becoming divers, or an early adaptation to diving. The subsequent rates of change in FVC and FEV1could be dependent on both the initial level of lung function and the cumulative exposure to diving. Divers may also show signs of reduced transfer factor for carbon monoxide (TlCO) immediately after deep saturation dives5-7 when compared with a control group.4
An international consensus conference in 19938 concluded that there is evidence that deep diving has slight but definite long term effects on the lung, including increased total lung capacity and a reduction in small airways conductance and gas transfer capacity. However, the scientific evidence was considered limited and future research, with the highest priority to longitudinal studies, was recommended.8
The aim of this study was to characterise the pulmonary function and the effect of previous diving exposure at the start of a professional career for divers and to compare the measurements at the start and at the end of a 15 week introductory diving course with the results 1 and 3 years after the diving course and to see if changes could be related to diving activity during follow up.
Material and methods
THE COHORT
The divers were all male students at a diving school in the Oslo area. The school offers three courses annually, each lasting 15 weeks. The cohort was established in the period 1992–4, and included subjects from seven successive courses. All 95 students were asked to participate in the study. Two subjects who refused to participate, two female students, and four students who only participated in one pulmonary function testing during the diving course, were excluded. Thus the study included a total of 87 male divers who participated in two tests of pulmonary function at the start and at the end of the course (table 1). Among the 87 divers 31 (36%) were current smokers and 20 were previous smokers. Twelve had stopped smoking within 1 year before the study and thus were considered smokers in the data analysis. At the start of the study the current smokers had smoked a mean (SD) of 5.2 (4.3) pack-years. The mean (SD) number of weekly physical training hours was 4 (3.9) at the start of the study. All divers gave written informed consent. The study is part of a multicentre study of health effects of diving, approved by the regional ethics committee for medical research both in Oslo and Bergen, Norway.
Age, height, and weight in 87 male divers (students) participating in the study including nine divers with decompression sickness or unconsciousness during follow up
At the start of school 69 of the 87 students had SCUBA diving experience. There were no differences in smoking habits, height, weight and age between pre-exposed and never exposed divers (table 1). Eighty three divers participated in the follow up study 1 year after attending the school, and 81 in the follow up after 3 years. Those who were classified as smokers in the first study were also classified as smokers in the 1 and 3 year follow up study. Six divers were lost to follow up, among them three had moved to foreign countries. During the 3 year follow up the group of divers had a mean (SD) increase in weight from 80.0 (10.4) kg to 82.6 (9.7) kg.
DIVING EXPOSURE
Previous diving exposure was registered by a questionnaire. Sixty nine subjects had a median number of 70 (range 2–3000) dives and had reached a mean (SD) maximum depth of 41 (14) metres before school (figure 1 A and B).

(A) Number of dives among 87 men before a 15 week introductory course at a school for occupational divers. (B) Maximal depths (m) obtained by 87 men before a 15 week introductory course at a school for occupational divers.
During the course diving was performed to depths of a maximum of 50 metres of sea water. The divers used air as breathing gas. Most of the diving took place during the last 11 weeks. All divers wore umbilical-type air supplied demand equipment, a Kirby Morgan band mask 18B or a Kirby Morgan superlite helmet 17B and neoprene wet or dry suits. The mean (SD) time spent in the water during the diving course was 40 (5) hours and the mean number of dives was 44 (6).
Registration of diving activity during the follow up period of 3 years was not completed by all divers due to lack of registration in log books or bad memory. Diving activity was reported by 77 among 83 divers during the first year of follow up. At last follow up 67 among 81 divers reported diving activity during the preceding 2 years (fig 2 A).

(A) Number of dives among 83 divers the first year of follow up (shaded bar) and 79 subjects during second and third year of follow up (filled bar). (B) Maximal depths (m) obtained by 83 divers the first year of follow up (shaded bar) and 79 subjects during second and third year of follow up (filled bar).
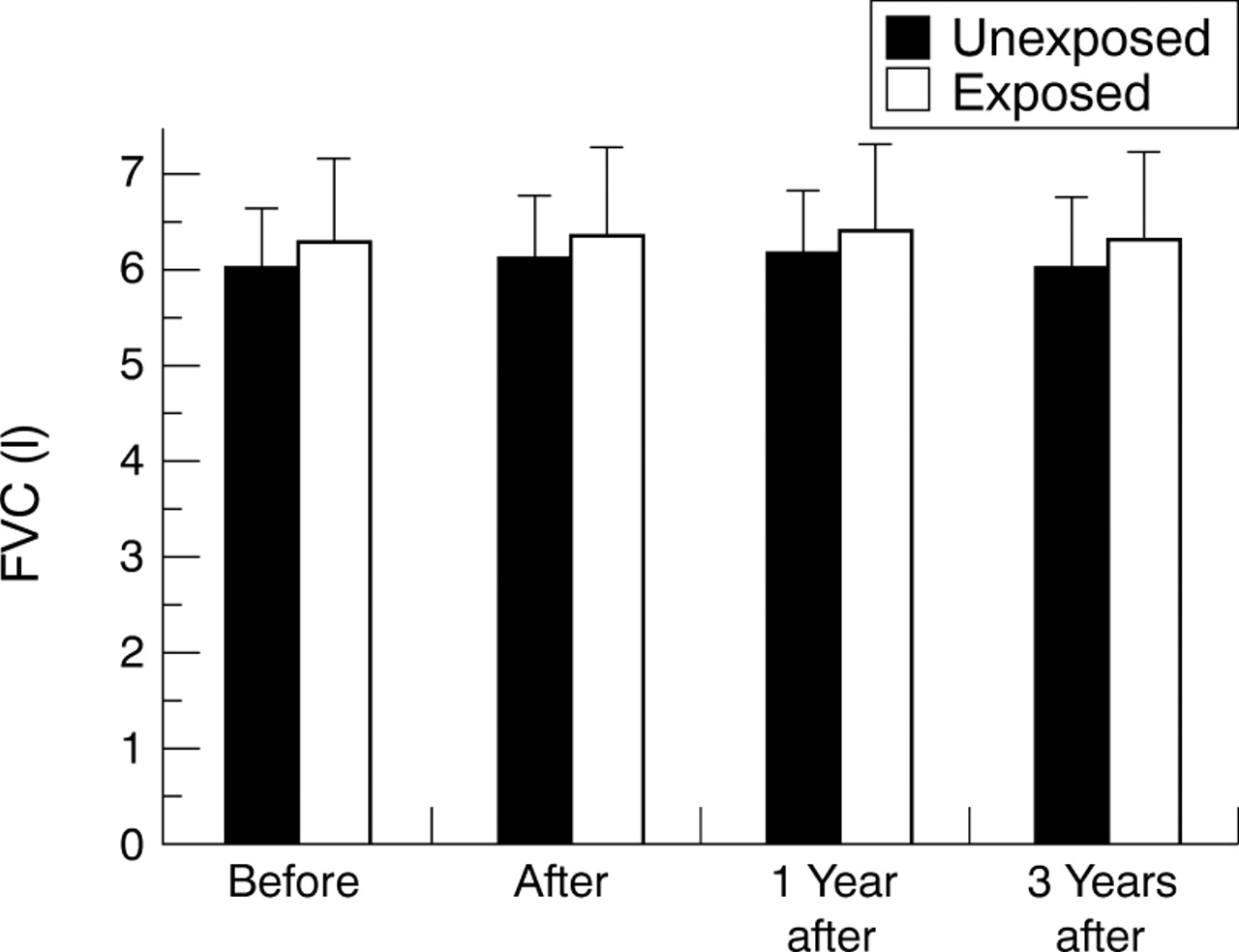
FVC (mean (SD)) at the start and end of school, and at 1 and 3 years of follow up among the two groups of divers who were unexposed (n=16) and exposed (n=65) at the start of school.

FEF25–75% (mean (SD)) at the start and end of school, and at 1 and 3 years of follow up among the two groups of divers who were unexposed (n=16) and exposed (n=65) at the start of school.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
TlCO (mean (SD)) at the start and end of school, and at 1 and 3 years of follow up among the two groups of divers who were unexposed (n=16) and exposed (n=65) at the start of school.
The median number of dives performed during the 3 year follow up was 95 (range 0–722).
The mean (SD) depth of the deepest dive performed during the first year of follow up was 40 (16) metres and during the second and third postcourse years it was 38 (20) metres. Reports of diving activity after 1 year of follow up showed that 10 had dived to a depth of ⩾50 metres. During the second and third year of follow up 18 divers reported that they had been ⩾50 metres (fig 2B).
DIVING RELATED DISEASE AND ACCIDENTS
No diver had been treated for decompression sickness (DCS) before attending the school, but one subject reported an episode of symptoms consistent with skin bends. No accidents or DCS were recorded during the time at school. Based on the divers' written statements, 10 episodes of decompression sickness (DCS) occurred in seven different divers in the follow up period of 3 years. There were four episodes of neurological DCS, including one which affected the inner ear. Three were treated by recompression in a hyperbaric chamber. Of six reported episodes among four divers of non-neurological DCS, two episodes were treated in chambers. One subject had experienced three episodes of DCS in the knee during the second and third year of follow up treated by recompression procedures in water. Two divers had been brought unconscious onshore and were treated in hospital and in chambers. The lung function of the nine divers that had endured DCS or had been unconscious in the sea during the 3 year follow up were compared with the other divers (table 1, table 2, table 3).
Diving exposure among divers who subsequently had accidents (n=9) and active divers without any accidents (n=72)
Results of selected lung function variables before exposure at school among 18 never exposed divers, 69 previously exposed divers and the nine divers who subsequently had accidents
Four episodes of middle ear barotrauma during follow up were reported among three different divers.
PULMONARY FUNCTION TESTS
The pulmonary functions of divers were compared with predicted values from a reference population consisting of a healthy never smoking segment of a randomly selected population on the south western coast of Norway.9 10 Linear models overestimate FVC and FEV1 in young age groups. Thus we have used the second order polynomial model of Gulsvik et al 9 when we study the divers at baseline. This model shows the evolution of FVC and FEV1 with age. The FVC and FEV1 increase with age up to a peak at the age of 25–30 years, after which they decrease.
The pulmonary function testing was performed with the Jaeger MasterLab (Erich Jaeger GmbH&CoKG, Wuerzburg, Germany). The same technician performed all tests. The divers were tested before and after the diving course and 1 and 3 years after the course. At each event lung function was measured at least 2 days after the last dive had been performed, because changes in pulmonary function has been shown shortly after open sea bounce dives.11 The subjects were given standardised instructions on the forced maximal expiratory manoeuvre, and transfer test with a demonstration of the procedures. The tests were performed with the subjects sitting in a chair breathing through a mouthpiece with a nose clip. The spirometer was calibrated by means of a 2 litre syringe twice daily and test gas calibrations were also performed twice daily with the instruments automatic calibration programme. The best results according to ATS criteria of at least three flow volume manoeuvres performed were used in the analysis.12 The peak expiratory flow rate (PEF), FVC, FEV1, forced mid-expiratory flow rate (FEF25–75%), and forced expired flow rates at 25%, 50%, and 75% of FVC expired (FEF25%, FEF50%, FEF75%) were measured. The TlCO was measured by the single breath holding method.13 Two measurements of TlCO were taken on each occasion. The average of the two measurements was used in the analysis. Effective alveolar volume (VA) was measured simultaneously by helium dilution, and the transfer per unit effective alveolar volume (KCO) was calculated.
STATISTICS
Student's two group test, two sided was used when comparing the never exposed and pre-exposed groups of divers. Student'st test was used in the data analysis to compare the groups of divers and their predicted values. A pairedt test was used to study the group of divers at different times of follow up, with the Bonferroni method when multiple comparisons were made. Multiple linear regression analysis was used to study the effect of smoking habits and diving exposure (number of dives) on the relative change between the first and last lung function measurement. All tests were two sided and the data were expressed as means (SD). A significance level of 5% was chosen.14 SPSS for Windows (SPSS 1989–92) was used in the data analysis.
Results
There was no significant difference in initial lung function variables between the 18 never exposed divers and the 69 pre-exposed divers (table 3). The lung functions of the nine divers who had accidents were not different from those of the other divers. Nor did we find any differences in preschool FVC, FEV1, and TlCO between the 69 pre-exposed and the 18 never exposed divers when the results were expressed in percentage of predicted values. In both groups the initial FVC, FEV1, and TlCO values were significantly greater than the predicted values. For the pre-exposed divers we found no effect on FVC or any of the other lung function variables of any of the exposure variables on previous diving.
During the diving course there was a significant increase in VA of 2.6% (SD 5.4%, p<0.001) among the 87 divers, no significant change in TlCO, and a significant fall in KCO of 3.2% (SD 7.1, p<0.001). At baseline, the 43 smokers showed a significantly lower value of TlCO compared with non-smokers, 13.2 (SD 2.3) and 14.7 (SD 1.9) mmol/min/kPa (p=0.001) respectively. No effect of smoking on changes was found on dynamic lung volumes or gas diffusion after the 15 week follow up period.
Tables 4, 5, and 6 and figures 3-5 show the results during follow up. Table 6 shows the results in the regression model. A significant reduction in FEV1 and maximal expiratory flow rates (FEF25–75%, FEF50%, FEF75%) was found when the results at 3 years follow up were compared with the results before school, after school, and at the 1 year follow up. A significantly increased VA and a significant reduction in TlCO and KCO were also noted. However, no significant effect of cumulative diving exposure, including the number of dives, on the relative changes of any of the lung function variables was found.
Selected lung function values in the 81 divers attending the 3 year examination
Selected lung function values among the 16 never exposed and 65 previously exposed divers studied at 3 years follow up
Regression coefficients for number of dives and cigarette smoking on relative change of selected lung function variables of first and last measurement
The divers who were accident prone (n=9) seemed to perform deeper dives and increased the number of dives during follow up compared with the divers who had no accidents during the 3 year follow up (table 2). We found no difference between the nine accident prone divers and the others when relative changes in lung function during the 3 year follow up were compared.
Discussion
This study indicates that divers have larger lungs (FVC) than predicted when they start their diving career and FVC may increase slightly due to adaptation to diving. The results may also indicate a tendency towards small airways dysfunction during the 3 year follow up period. The FEV1 , FEF25–75%, and FEF75% were significantly reduced and VAincreased.
A larger than predicted vital capacity was found among the diving students at baseline. In the subgroup of students with previous recreational diving experience, but also among the subgroup without previous diving experience, the vital capacity was significantly different from the predicted value.9 There was, however, no significant difference between the subgroup with previous diving experience compared with the group without. The diving school has a selective intake of students based on a medical examination, and only physically fit students are accepted.
After the first year of follow up the FVC and VA were increased compared with precourse values. During this period the diving activity was most intense. The FVC between the first and third year of follow up decreased, and this could be due to less diving activity over the 2 later years of follow up. This supports the possibility of adaptation to diving. An increased FVC among divers has been reported previously by others.1-3 This has formerly been suggested as being caused either by positive selection of students1or as a result of increasing exposure to diving.3Increased breathing resistance due to increased gas density,15 swim training,16 and breathing equipment, could contribute to an increase in vital capacity, which could be attributed to the exercising of inspiratory muscles.
The observed changes in FVC were, however, small and have probably no clinical nor physiological significance.
There was a significant increase in VA over the 3 year observation period. This observation could reflect the normal evolution of VA with age, or it could reflect a hyperinflation due to narrowing of small airways. The normal change in VA over 3 years in this age range is not known. There is a transient increase in static lung volumes immediately after deep saturation dives,17 but in a cross sectional study of experienced saturation divers4 there was no difference in static lung volumes or VA when compared with a control group.
A change of FEV1 would not be expected among men in their early 20s during a 3 year follow up.9 18 A decline in FEV1 measured by longitudinal studies is less than suggested by cross sectional studies and starts in the mid-30s among men.18 However, the reduction in FEV1 and flow rates at low lung volumes has not shown any relation to exposure to diving. Thus we might have seen the natural history of lung function over time in this highly selected group of divers. We found FEV1 100% of predicted values in both groups of divers at the start of the course. However, FEV1 was significantly reduced at the 3 year follow up.
The divers also showed a loss in FEF25–75% ,FEF50%, and FEF75% 3 years after the diving course. A reduction in maximum expiratory flows at low lung volumes has been a consistent finding in all previous studies of divers' lung function.1-3 19 The change in flows could be an indication of small airways dysfunction, but interpretation of the index is critically dependent on the concurrent absolute lung volume. In previous cross sectional studies of divers a reduction in FEF75% in divers was found when compared with other groups with the same vital capacity1-3 and same static lung volumes.4
During diving the airways could become narrowed by the external physical pressure of the distended alveoli. Subsequent chronic inflammation may appear, with thickening of the walls of the bronchioles or loss of lung elasticity, leading to dynamic compression of the airways during forced expiration.3 In a postmortem study, Calder et al 20 have shown distension of the alveoli among eight divers in whom the ratio of FEV1 to FVC was known to be reduced.
Our findings of reduced gas transfer capacity accords with other published values that show a reduction among saturation divers after one dive of long duration where the gas transfer capacity was decreased, at least temporarily.5-7 17 In a previous study of young occupational divers performing bounce dives to shallow depths, we found that one single dive to 10 or 50 metres caused a transient reduction in gas transfer capacity,11 which nearly returned to normal within 1 week after the dive, but without knowledge of the time course in between. Other studies indicate that these changes become normal within 24 hours.21 In epidemiological studies of divers' lung function the time of the assessment of pulmonary function should be at least 2 days after the last dive performed, preferably more.21
The findings in the study could result from bias or systematic error. Apart from selection of divers at the start of the study, the prospective design with comparison at frequent intervals within each young diver, gives good control over the sources of bias. Also the fact that few subjects were lost to follow up minimises the possibility of errors. However, a random misclassification could be introduced as the exposure data registered in log books varied among the divers. All divers were asked to bring their log books at each follow up. Most occupational dives were logged whereas some of the recreational dives were not. However, each diver was asked to memorise his history, and to give the best information possible on depth and number of dives. In general, all dives are characterised by pressure, time, and gas mixture as the basic physical variables. Cumulative exposure to diving will therefore be strongly related to the number of dives and depths. Other derived estimates of specific exposure like hyperoxia will also be related to these basic variables. The number of dives and depths should therefore be an adequate estimate of non-specific cumulative exposure to diving.
We found no association between change in lung function and diving exposure during follow up. Former studies, reporting an association between diving exposure and change in lung function, have mostly been cross sectional studies mainly among older divers1-4 22at ages 30–35 years with 6–9 years of diving experience. The present study reports small changes in lung function within a group of young divers with a limited number of dives. A longitudinal study with only 3 years of follow up would require more subjects in the study to draw any conclusions.23 However the pattern of changes occurring among the divers is the same as others have found,1-7 and the cohort will be subjected to further follow up according to the recommendations given at the international consensus conference in 1993.8
In conclusion, the results indicate that divers initially belong to a selected group with larger lung volumes than predicted. There may be an adaptation to diving with a further small increase in lung volumes. Any association between diving and airways obstruction needs further follow up.
Acknowledgments
This study was supported financially by Statoil's Fund for Research in Occupational Medicine, Oslo, Norway and The Research Council of Norway. We thank the Norwegian Commercial Diving School and Dr Helge Kjuus for excellent assistance and support.