Article Text

Abstract
OBJECTIVES To investigate the occurrence of work related respiratory symptoms and to assess the effect of atopy in a group of trainee bakers.
METHODS A prospective study of work related respiratory symptoms among 125 trainee bakers who were investigated with a questionnaire plus skin prick test with wheat flour and α-amylase allergens at baseline and then after 6, 18, and 30 months.
RESULTS At the baseline examination, four students (3.2%) complained of respiratory symptoms (cough and rhinitis) when working with flours and four were skin positive to wheat flour or α-amylase. The incidence of work related respiratory symptoms was 3.4% at 6 months, and the cumulative incidence was 4.8% and 9.0% at 18 and 30 months, respectively. The incidence of skin sensitisation to occupational allergens was 4.6% at 6 months and the cumulative incidence was 4.6% at 18 months and 10.1% at 30 months. The generalised estimating equation approach to longitudinal data showed that work related respiratory symptoms in the study population was significantly associated with a personal history of allergic disease (odds ratio (OR) 5.8, 95% confidence interval (95% CI) 1.8 to 18.2) and skin sensitisation to wheat flour or α-amylase (OR 4.3, 95% CI 1.2 to 14.9). Atopy based on prick test was not related to the occurrence of work related respiratory symptoms over time (OR 1.1, 95% CI 0.3 to 3.8).
CONCLUSIONS Personal history of allergic disease is a predisposing factor for the development of symptoms caused by exposure to wheat flour and may be a criterion of unsuitability for starting a career as a baker. Atopy based on the skin prick test is useful for identifying subjects with allergic disease, but should not be used to exclude non-symptomatic atopic people from bakery work.
- follow up study
- wheat flour
- α-amylase sensitisation
- work related respiratory symptoms
Statistics from Altmetric.com
Pre-employment medical examination is considered to be an important practice in recently introduced Italian legislation on safety and health at the workplace, and pre-employment medical screening is also common practice in other countries of the European Union.1 The aim of this practice should be to reduce adverse health effects during working life, without discrimination or damaging workers. It is thus essential that the content of such medical assessments is both accurate and reliable.
Several authors have noted a close association between allergic respiratory symptoms and atopy based on skin prick tests among workers affected by occupational asthma due to high molecular weight substances.2-7 Nevertheless, there is still great debate about the wisdom and practicability of excluding atopic people from work at risk of sensitisation, because of the large number of atopic people who would be considered unsuitable to work and because this type of screening programme may distract attention from improving the work environment.3-10 Prospective studies of newly exposed young workers are essential for a clearer understanding of the fate of atopic people who are exposed to occupational allergens, but unfortunately, such data are still scarce and the results obtained so far are not consistent.11-14
The aim of this paper is to present the results of a follow up prospective study of work related respiratory symptoms, skin sensitisation to occupational allergens, and atopy among trainee bakers at a vocational school.
Materials and methods
SUBJECTS AND MEDICAL INVESTIGATIONS
In a previous paper we presented the results of a cross sectional study among trainee bakers in northern Italy.15 The present study reports the results of a prospective evaluation of a subsample of the same subjects. The training of bakers consists of a 2 year course of baking and pastry making, including a period working in bakeries. An additional year of training in pastry making is optional. The subjects participating in this follow up study were all students who had started their first or second years in November 1992 or November 1993.
In the previous study,15 144 trainee bakers and a group of 81 trainee graphic artists (used as controls), were evaluated for smoking habit, atopy based on skin prick test, IgE concentrations, skin test and RAST/EAST to wheat flour and α-amylase, personal history of allergic disease, and of upper respiratory airway infections. Work related respiratory symptoms were defined as attacks of rhinitis, coughing, wheezing, and dyspnoea when working with flours.
In the present study, a subsample of 125 trainee bakers were retested at 6, 18, and 30 months after the baseline examination, with a questionnaire, to update eventual symptoms, plus skin prick test for wheat flour and α-amylase. From the first investigation, 19 subjects were lost to follow up because they had left the school or moved elsewhere. Of these, only one subject was skin sensitised to wheat flour and complained of rhinitis when working with flours. Of the 125 subjects who participated in the follow up, 42 were followed up for 6 months, 36 for 18 months, and 47 for 30 months. Sixty subjects were tested twice, and 45 and 20 attended three and four examinations, respectively (table 1). The subjects with an incomplete follow up (those attending only two or three check ups) had either been absent from school on the days of the follow up or had finished their training.
Study design and distribution of trainee bakers during the follow up
STATISTICAL METHODS
Data analysis was performed with the statistical software Stata 5.0 (Stata Corporation, 1997). Continuous variables were summarised as means (SDs). Nominal variables were expressed as numbers and percentages. Cumulative incidence at 18 and 30 months was calculated with life tables according to the procedure described by Bothamet al. 13 Incidences over the three periods, 0–6 months, 6–18 months, and 18–30 months, were obtained from the subsamples followed up over those periods. The relation of the outcome to explanatory variables was assessed by applying the generalised estimating equation to longitudinal data to account for correlation between repeated responses for each subject.16 Odds ratios (ORs) were used to measure the effect of covariates on binary responses with multivariate marginal logistic regression models. Ninety five per cent confidence intervals (95% CIs) for ORs were derived from robust variance estimates.16
Results
The mean (SD) age of the students seen at follow up was 15.5 (1.6) years; 57% were males, 24% were smokers and 13% complained of allergic symptoms.
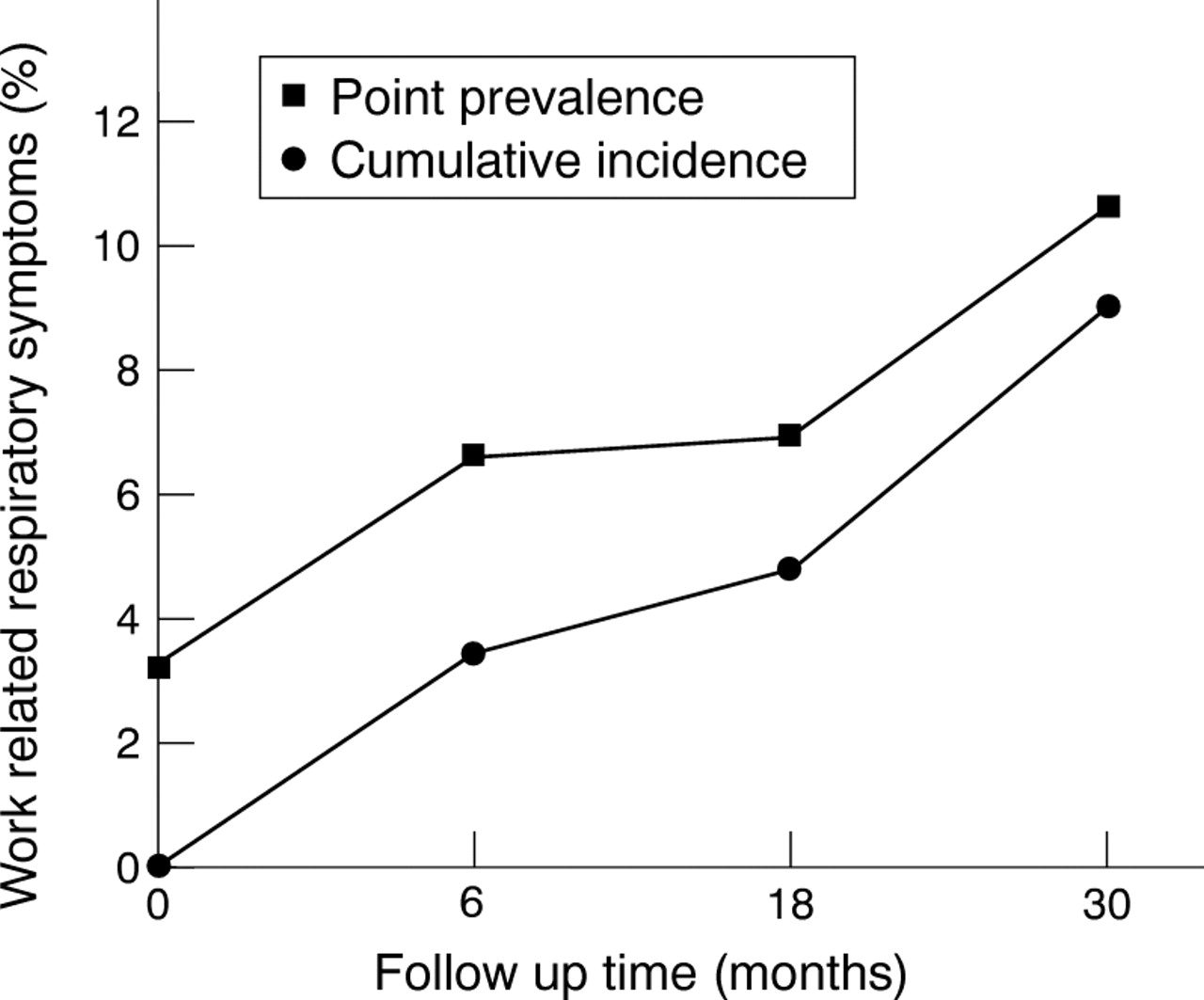
At the baseline examination, four of these 125 students (3.2%) had complained of cough and rhinitis related to work and four others (3.2%) were skin positive to wheat flour or α-amylase. At the end of the present study, there were 10 students with work related respiratory symptoms and 10 skin positive to wheat flour. Of those skin positive to wheat flour, three were also sensitised to α-amylase. Three of the new cases of work related respiratory symptoms were found at the 6 month follow up (incidence 3.4%). Cumulative incidence at 18 and 30 months was 4.8 and 9.0%, respectively (fig 1). Four of the new cases with skin sensitisation to occupational allergens were found at the 6 month follow up (incidence 4.6%). Cumulative incidence at 18 and 30 months was 4.6 and 10.1%, respectively (fig2).

Point prevalence and cumulative incidence of new cases of work related respiratory symptoms during the follow up among trainee bakers.

{kind=link}
{kind=link}
Point prevalence and cumulative incidence of new cases of skin sensitisation to wheat or α-amylase during the follow up among trainee bakers.
Six of the 10 students with work related respiratory symptoms during follow up complained of allergic disease and in four of them the pre-existing symptom was asthma. In four cases, symptoms were continuously present at the different follow up periods, but the remission of respiratory symptoms in two cases might be due to drug treatment for their pre-existing allergic disease. Seven symptomatic students showed a positive skin test to wheat or α-amylase at least once during the follow up and six were atopic by prick test.
The generalised estimating equation applied to longitudinal data showed that work related respiratory symptoms in the study population were significantly associated with a personal history of allergic disease (OR 5.8, 95% CI 1.8 to 18.2) and skin sensitisation to wheat flour or α-amylase (OR 4.3, 95% CI 1.2 to 14.9, table 2). Increased ORs were also found for drug treatment for respiratory disease and exposure to wheat flour outside school, but the association with work related respiratory symptoms was not significant. Atopy based on prick test was not related to the occurrence of work related respiratory symptoms over time (OR 1.1, 95% CI 0.3 to 3.8). Similarly, family atopy, atopy based on serum IgE concentrations and positive RAST for wheat flour were not associated with work related respiratory symptoms.
Association between respiratory symptoms related to work and various independent variables in the study population of trainee bakers
Current smokers showed an increased, although not significant, risk of work related respiratory symptoms (OR 2.0, 95% CI 0.7 to 5.7) and skin sensitisation to wheat flour or α-amylase (OR 1.7, 95% CI 0.5 to 6.4).
Discussion
The most widely used methods for the medical screening and surveillance of occupational allergic respiratory diseases are itemised questionnaires, spirometry and immunological tests to identify atopy. Several studies have sought to assess the importance of atopy as a marker of susceptibility to occupational allergic respiratory disease, but a fundamental problem is the lack of agreed criteria to define atopy. Two broad definitions of atopy are principally used, based on a personal history of allergy and on positive skin prick test to common environmental allergens.10 11 Whichever of these definitions is adopted, there seems to be an association between atopic diathesis and allergic respiratory disease among animal handlers, bakers, and workers exposed to latex.2 3 17-19 The significance of the finding is debatable, however, because the design of the various studies is cross sectional and in most cases includes subjects who have been working for some time.
The results of retrospective cohort studies are also controversial. With pre-employment data at a plant producing enzymes, Johnsenet al showed that occupational exposure and atopy were significant determinants of clinical enzyme allergy.20 They reported a 3 year cumulative incidence of 8% for clinical enzyme allergy. In a retrospective cohort study with pre-employment screening data, Kruize et alfound that atopic predisposition at the time of engagement was not a significant risk factor for laboratory animal allergy, even though its reported incidence was 19.2%.21
Very few prospective studies have been conducted with apprentices just starting exposure to high molecular weight agents. In a follow up study on the incidence of allergy to laboratory animals and the influence of atopy and pre-existing sensitisation, Botham et al found that both atopic diathesis and pre-sensitisation to laboratory animals increased the likelihood of a person developing laboratory animal allergy.13 Neither factor, however, was an accurate predictor of disease. More recently, Fuorteset al did not find atopy to be a risk factor for complaining of work related respiratory symptoms among laboratory animal workers.14 In this study, the prevalence of work related respiratory symptoms at the first 6 month follow up was about 5% and the incidence of work related asthma was 2.5% at 6 months and 4.5% at 24 months.
Prospective studies have not been carried out among bakers, and there are few studies about the personal and health characteristics of newly exposed workers.22 25 Among subjects newly exposed to flour, Cullinan et al found that work related respiratory symptoms were not related to atopy and that there was only a weak association between symptoms and specific sensitisation.24
In a recent cross sectional study, Gautrin et al have found that when first exposed to high molecular weight allergens, apprentices have a low but substantial frequency of specific sensitisation to work related allergens.25 The proportion of skin sensitisation to flour documented by these researchers was similar in groups of trainee pastry makers and dental hygienists (5%). They suggest that the presence of skin reactivity to flour before the beginning of significant exposure can be explained by an increased propensity for polysensitised people to develop sensitisation mediated by IgE. Moreover, among the pastry makers, specific sensitisation to flour was associated with symptoms.
In the present investigation, the risk for work related respiratory symptoms over time was significantly related to personal history of allergic disease and skin sensitisation to wheat flour, but not to atopy based on a skin prick test. These results support the suggestion that atopy based on a skin prick test is insufficient to predict the fate of workers exposed to wheat flour. Thus, screening out atopic non-symptomatic workers from certain occupations seems unacceptable, because of its low predictive value for occupational allergic diseases and in view of relocation difficulties and the adverse implications of unemployment.3 8 10 13 26 27 It is quite possible that baseline polysensitisation and cross reactivity increase the propensity for developing sensitisation to specific occupational allergens mediated by IgE. For this reason, atopic people must be advised about their increased chance of developing work related respiratory symptoms, but if they are free of symptoms, they should not necessarily be prevented from doing work involving exposure to high molecular weight allergens.
On the other hand, there is strong evidence in favour of rejecting people who complain of allergic disease, most of whom are atopic by skin prick test. In this follow up study, six of the 10 subjects with work related respiratory symptoms also complained of allergic disease and most of them were asthmatic. These symptomatic subjects may be considered to be at major risk and defined during pre-employment evaluation as unsuitable to work as bakers. People affected with asthma may need to be more selective in the careers they choose, taking care to avoid occupations that may provoke attacks. Moreover, jobs may be lost more easily or acquired less readily because of absence or diminished work performance due to illness.26-28
In conclusion, the present follow up study indicates that atopy based on a skin prick test is useful for identifying subjects with allergic disease, but should not be used to exclude non-symptomatic atopic people from work as bakers. The finding that a personal history of allergic disease is the main predisposing factor for the development of symptoms among trainee bakers is further evidence in favour of excluding young atopic people with symptoms from starting a job involving exposure to high molecular weight agents. On the other hand, avoiding the kind of exposure that can aggravate allergic disease is a sensible option which is part of preventive strategies for allergic disease in general. Moreover, if pre-employment screening is done early on in working life, the social cost will be more acceptable, because at this stage the young workers can more easily change their career.