





Abstract
Elevated serum levels of antigen-specific immunoglobulin (Ig)E are often associated with allergic respiratory diseases. This parallel-group, randomised, double-blind, placebo-controlled trial was designed to study the influence of omalizumab on the early nasal response to allergen challenge reflected by symptom score and inflammatory marker levels in nasal lavage fluid (NAL).
A total of 23 patients with allergic rhinitis took part in the study, 11 were given placebo and omalizumab was administered subcutaneously in 12. Omalizumab or placebo were given at 2‐ or 4‐week intervals based on a patient's body weight and IgE levels to a total dose of 0.016 mg·kg−1·IgE−1 (IU·mL−1) every 4 weeks.
Compared to placebo, 16 weeks of treatment with omalizumab significantly inhibited allergen challenge-induced nasal symptoms (median symptom score 7.0–0.5 versus 7.0–7.0) and inhibited the increase of human serum albumin (median 15.3–0.12 mg·mL−1 versus 8.2–19.7 mg·mL−1) in the NAL after allergen challenge. Treatment with omalizumab induced a significant decrease in tumour necrosis factor‐α levels in basal NAL, but no change was seen for histamine.
These results indicate that subcutaneously administered monoclonal anti-immunoglobulin‐E antibody, omalizumab, inhibits the nasal responses to allergen challenge of patients with allergic rhinitis. Omalizumab may provide a new strategy for the treatment of allergic rhinitis.
Allergic rhinitis is a common, increasingly prevalent disease 1, 2, associated with elevated serum immunoglobulin (Ig)E‐levels. Binding of inhaled allergens to IgE on the surface of basophils and mast cells, with subsequent cross-linkage of IgE and aggregation of high-affinity receptors for IgE (FcεRI), triggers the release of histamine, leukotrienes and other inflammatory mediators, followed by the onset of allergic symptoms 3. Current therapeutic strategies include corticosteroids, mast cell stabilisers, antihistamines and immunotherapy. Removal of circulating free IgE by the recombinant humanised monoclonal anti-IgE antibody, omalizumab (Xolair®), also referred to as rhuMAb‐E25, represents a new approach in the treatment of allergic rhinitis.
Omalizumab is a construct of the murine antibody MAE11 that binds to circulating IgE on the Fc site of the IgE antibody 4. It does not interact with cell-bound IgE and therefore does not provoke histamine release from IgE‐sensitised mast cells 5. It also inhibits IgE binding to mast cells 6. In vitro, omalizumab inhibits allergen-induced IgE synthesis by peripheral blood mononuclear leukocytes from atopic volunteers 4. The efficacy, safety and tolerability, as well as pharmacokinetics and pharmacodynamics of omalizumab, have been assessed in single- and multiple-dose studies 7–10. In asthmatic subjects, omalizumab attenuates both the early- (EAR) and late-phase responses to inhaled allergen 11–13. Moreover, omalizumab induced reduction of asthma exacerbations and steroid requirement in allergic asthmatics 14. In birch pollen-induced seasonal allergic rhinitis, omalizumab reduces concomitant medication and symptoms 7.
As the EAR is mediated by IgE leading to mast cell or basophil degranulation and release of inflammatory mediators, the aim of this randomised, double-blind, placebo-controlled, parallel-grouped study was to determine if omalizumab has effects on the nasal EAR in subjects suffering from allergic rhinitis. The patients were challenged nasally with the appropriate allergen. As a primary parameter, changes in the nasal symptom score were studied. Reduction of the nasal symptom score would support the clinical effectiveness of omalizumab. Additionally, inflammatory markers in nasal lavage fluid (NAL) were measured. These included histamine, the major mediator of the EAR, human serum albumin (HSA), a marker of vascular permeability, and interleukin (IL)‐1β and tumour necrosis factor (TNF)‐α, cytokines altered in the EAR after nasal allergen challenge.
Methods
Subjects and study design
A group of 23 patients suffering from allergic rhinitis participated in the study (table 1⇓). All had at least a 2‐yr history of allergic rhinitis and a positive nasal provocation test to the indicated allergen (table 1⇓). Omalizumab or placebo were administered subcutaneously at 2‐ or 4‐week intervals. Body weight and total IgE at screening were used to determine omalizumab administration of at least 0.016 mg·kg−1·IgE−1 (IU·mL−1) every 4 weeks.
Baseline characteristics of the study subjects
The study design is outlined in table 2⇓. The study was approved by the local Ethic committee and all patients gave informed written consent.
Study design
Nasal challenge
The patients were challenged nasally before treatment and after 16 weeks of treatment with the indicated allergen (table 1⇑). Patients were asymptomatic before the antigen challenge and no antihistamine or local nasal medication was allowed up to 4 weeks prior to challenge.
Prior to the final study protocol, the challenge dose was determined by titration until the subjects developed clinical symptoms. The dose of allergen given after 16 weeks of treatment was identical to the dose given at baseline. The mean dose of allergen needed was 10,000 allergy units.
The nasal challenge was performed as previously described 15. In brief, four prechallenge nasal lavages were performed with 5 mL saline solution to wash out pre-existing mediators. After this, the patients were challenged with diluent (albumin-buffered saline; ALK‐Scherax, Hamburg, Germany) and nasal lavages were repeated 15 min later. The allergen (ALK‐Scherax) was then inserted into each nostril using a plastic hand-held nebuliser delivering 100 µL at each actuation. Another nasal lavage was performed 15 min later. The NAL were placed on ice and frozen at −70°C until analysis. Histamine, albumin, IL‐1β and TNF‐α were measured in the NAL fluid of the first prewash (pre-challenge), after diluent and after allergen challenge.
Nasal symptom score
Total symptom scores ranging 0–12 were obtained from patients following nasal allergen challenge by using four-point scales for sneezing, itching, rhinorrhea and for congestion (0: none; 1: mild; 2: moderate; 3: severe).
Histamine
For histamine analysis, the NAL was assayed by an automated fluorimetric technique capable of detecting <0.4 ng·mL−1 histamine 16.
Human serum albumin
HSA was measured by enzyme-linked immunosorbent assay (ELISA). Plates were coated with HSA (5 µg·mL−1) overnight at 4°C and then blocked with 1% bovine serum albumin for 1 h. The wells were washed with TRIS buffer and received 100 µL of samples and 100 µL of mouse monoclonal anti‐HSA antibody (1:100,000) (Pierce, Rockford, IL, USA) for 1 h. The wells were washed and 100 µL alkaline phosphatase-conjugated goat anti-mouse IgG (Dianova, Hamburg, Germany) (1:1,000) was added for 1 h. The reaction was developed by using p‐nitrophenyl phosphate (Sigma, St. Louis, MO, USA) and absorbance was read at 405 nm. The detection limit was <1 ng·mL−1.
Cytokines
Concentrations of IL‐1β and TNF‐α were detected in the NAL using ELISA according to the manufacturer's instructions (Biosource, Camarillo, CA, USA). Detection limits were <0.19 pg·mL−1 for IL‐1β and 0.09 pg·mL−1 for TNF‐α.
Statistical analysis
Comparisons were made between groups using Mann-Whitney U‐test and within groups using Wilcoxon's signed-ranked test, respectively. Between-group treatment analysis was calculated by percentage change from baseline (pre-study challenge response) after 16 weeks of treatment. A p‐value of <0.05, using two-tailed tests, was considered statistically significant.
Results
Clinical response to nasal allergen challenge
The nasal symptom score of each subject was the same before the two nasal allergen challenges. In the nasal allergen challenge conducted after 16 weeks of treatment, patients treated with omalizumab showed a significantly lower nasal symptom score after challenge (fig. 1⇓, table 3⇓, p<0.001). Furthermore, the omalizumab group symptom score was significantly lower compared to baseline (table 3⇓, p<0.01).

Percentage change from baseline of nasal symptom score after nasal allergen challenge of the omalizumab group (n=12) and placebo group (n=11) after 16 weeks of therapy. Data are present as median (25th–75th percentiles). **: p<0.01.
Nasal symptom score and increase of histamine and human serum albumin (HSA) after nasal allergen challenge at baseline and after 16 weeks of therapy
Histamine
There was no significant difference in histamine levels between the pre-challenge NAL collected at baseline or after 16 weeks of treatment in either treatment groups (table 4⇓). After 16 weeks of therapy the increase in histamine in NAL after allergen challenge was significantly lower in the omalizumab group compared to baseline (table 3⇑, p=0.015). However, no significant difference was seen compared to the placebo group (fig. 2⇓, table 3⇑).

Percentage change from baseline of histamine release after nasal allergen challenge of the omalizumab group (n=12) and placebo group (n=11) after 16 weeks of therapy. Data are present as median (25th–75th percentiles).
Inflammatory markers in nasal lavage fluid of the first prewash at baseline and after 16 weeks of therapy
Human serum albumin
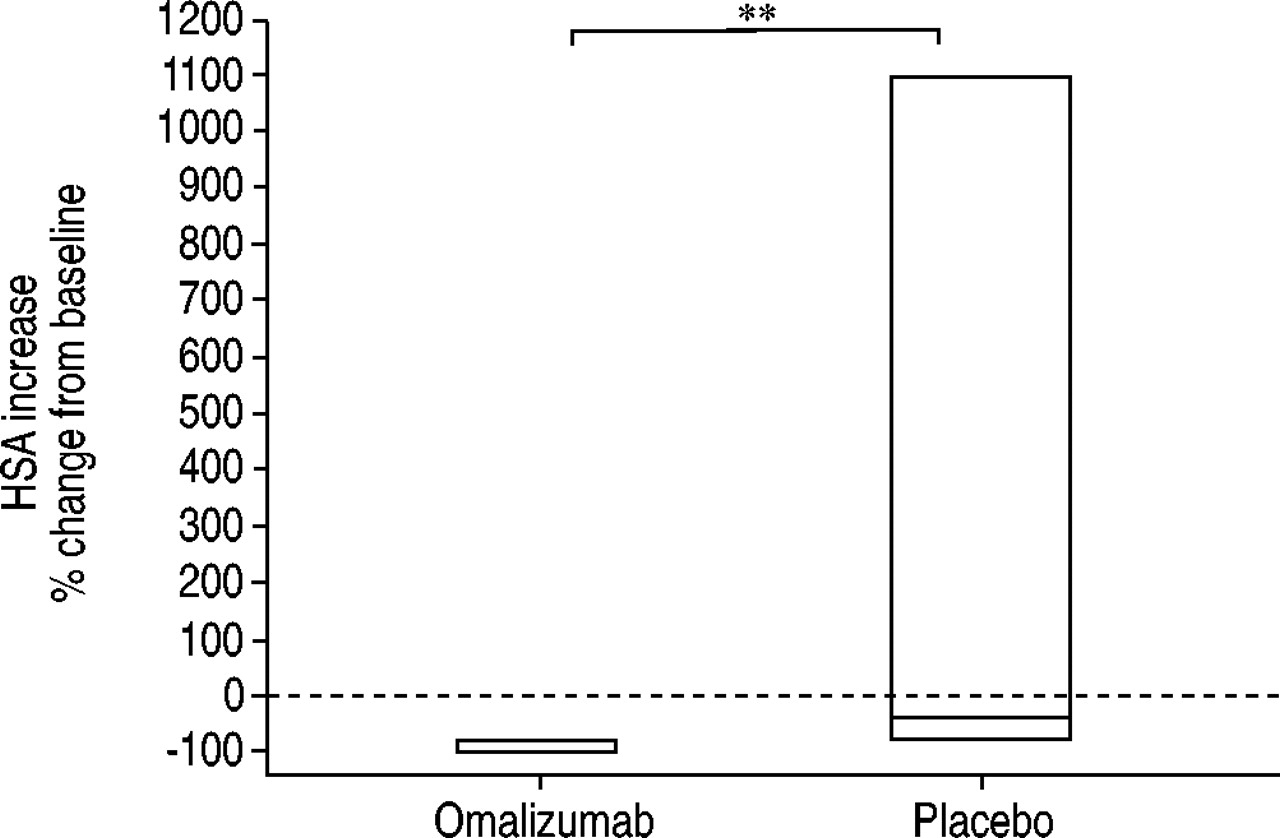
The HSA levels in pre-challenge NAL were not statistically different between treatment groups (table 4⇑). Following 16 weeks of treatment, the increase of HSA levels after allergen challenge were significantly lower in the omalizumab group compared to the placebo group (fig. 3⇓, table 3⇑, p<0.01).
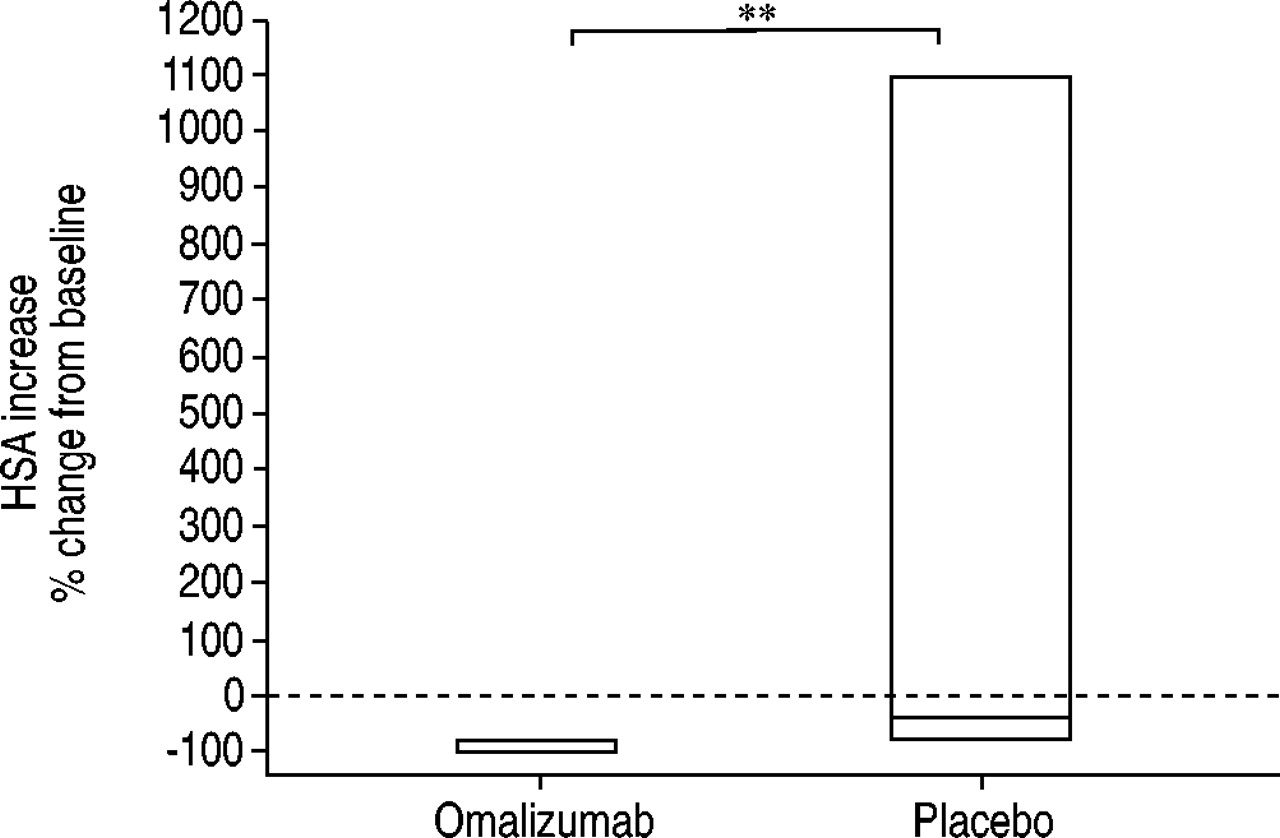
Percentage change from baseline of human serum albumin (HSA) release after nasal allergen challenge of the omalizumab group (n=12) and placebo group (n=11) after 16 weeks of therapy. Data are present as median (25th–75th percentiles). **: p<0.01.
Cytokines
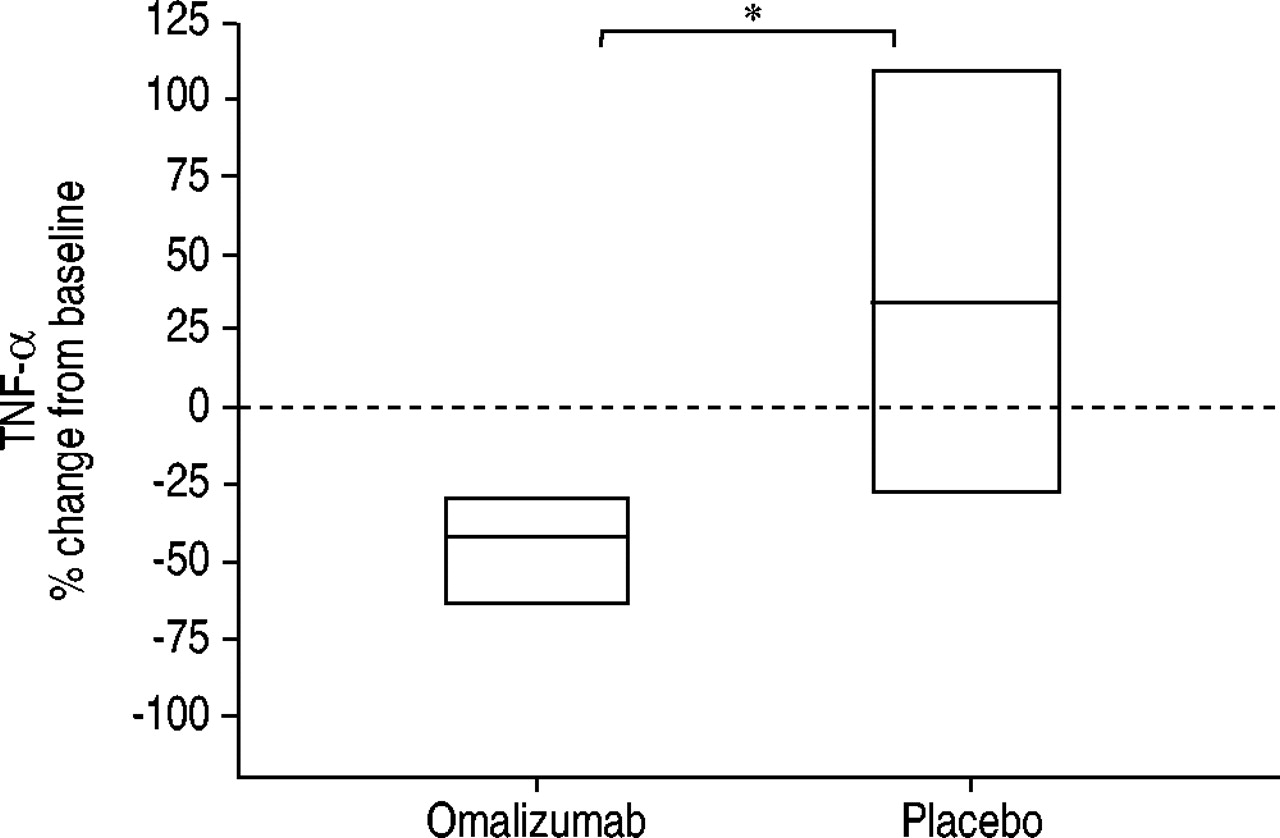
After 16 weeks trial treatment, the pre-challenge NAL showed a significant decrease of TNF‐α in the omalizumab group compared to the placebo group (fig. 4⇓, table 4⇑, p=0.015). There was no detectable statistically significant difference in pre-challenge IL‐1β levels between both groups (fig. 5⇓, table 4⇑). Following diluent or allergen challenge, TNF‐α and IL‐1β values were not detectable.

Percentage change from baseline in tumour necrosis factor (TNF)‐α in pre-challenge nasal lavage fluid of the omalizumab group (n=12) and placebo group (n=11) after 16 weeks of therapy. Data are present as median (25th–75th percentiles). *: p<0.05.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Percentage change from baseline in interleukin (IL)‐1β in pre-challenge nasal lavage fluid of the omalizumab group (n=12) and placebo group (n=11) after 16 weeks of therapy. Data are present as median (25th–75th percentiles).
Discussion
This study demonstrates that treatment with omalizumab, a humanised monoclonal antibody directed against IgE, reduces nasal EAR in subjects with allergic rhinitis.
Omalizumab treatment significantly reduces the nasal symptom score after allergen challenge. This demonstrates the effectiveness of omalizumab and these findings agree with recently published data describing a reduction of concomitant medication and symptoms in birch pollen-induced seasonal allergic rhinitis on treatment with omalizumab 7.
A statistically significant decrease of albumin after allergen challenge was observed in the NAL of omalizumab-treated subjects. Therefore, the effect of omalizumab could be caused, in part, by inhibition of vascular permeability reflected by albumin levels. Increased vascular permeability after allergen challenge is caused by mediators like histamine, kinins, leukotrienes or cytokines 17.
Histamine, stored in mast cells and basophils is the major mediator of acute allergic rhinitis, causing itching, sneezing, congestion and rhinorrhea by increasing vascular permeability, vasodilatation and glandular secretion 17. Within minutes of allergen exposure, histamine can be measured in nasal lavages 15. Infusion of omalizumab decreased basophil IgE and FcεRI surface density, and Ag‐induced basophil histamine release in vitro 18. Therefore, an omalizumab-induced inhibition of histamine release after allergen challenge was expected. However, no significant difference in histamine release after allergen challenge was found in patients treated with omalizumab versus those receiving placebo. This might be because omlizumab has no effect on histamine release in this model or because of the extensive variation in response to the different allergens used. This indicates that a larger number of subjects should be studied to determine whether the treatment effects are significant or not.
The nose also contains different inflammatory cells that may contribute cytokines to the allergic response 16. IL‐1β and TNF‐α levels have been measured 2 h after allergen challenge in nasal lavage, and their increase corresponded to the rise in neutrophil and eosinophil cell infiltration 19. In addition, mast cell activation in vitro leads to the release of pro-inflammatory cytokines, including TNF‐α and IL‐1β 19–21. IL‐1β is also produced by monocytes and macrophages after antigen stimulation, and is an important signal for the activation of resting T‐cells 22. Furthermore, TNF‐α and IL‐1β are involved in the regulation of allergic inflammatory processes, since both lead to a significant increase in adhesion receptor expression in vitro 20, 23. Omalizumab also induced a significant decrease in TNF‐α levels in the pre-challenge NAL, indicating an anti-inflammatory effect. No change was seen in the placebo group. Post-challenge, however, no detectable amounts of IL‐1β or TNF‐α were found. This could be explained by the additional hypersecretion factor and/or the short time between allergen stimulation and lavage sampling.
The results described here do allow a deeper insight into the mode of action of omalizumab. The binding of omalizumab to circulating IgE leads consequently to a downregulation of TNF‐α, and probably to a decrease in the liberation of stored and newly synthesised mediators from target cells (mast cells, basophils and eosinophils). The reduction in TNF‐α suggests possible downregulation on a fundamental level, since TNF‐α amplifies both immunologic and cellular mechanisms of inflammation.
In conclusion, these findings suggest that the use of the humanised monoclonal anti-immunoglobulin E antibody omalizumab, administered subcutaneously, inhibits the nasal responses to allergen challenge in subjects with allergic rhinitis. Therefore, omalizumab may provide a new strategy for the treatment of allergic rhinitis.
Acknowledgments
This study was supported by Novartis Pharma GmbH, Nurenberg, Germany.
- Received December 4, 2001.
- Accepted September 8, 2003.
- © ERS Journals Ltd
References









