





Abstract
In asthmatic subjects an imbalance between elastase and α1‐antitrypsin (α1‐PI) exists. This study aims to evaluate whether ageing per se affects the levels of elastase.
Both young and elderly asthmatics with comparable severity and duration of disease, as well as young and elderly healthy subjects, underwent an induced sputum procedure to measure levels of elastase and α1‐PI.
The percentage of sputum neutrophils and eosinophils was higher in young and elderly asthmatics than in young and elderly controls. The levels of both total and active elastase were significantly higher in young and elderly asthmatics than in young and elderly controls, and directly correlated with the percentage of neutrophils. In addition, in both young and elderly asthmatics the levels of total and active elastase were negatively correlated with forced expiratory volume in one second values, but positively correlated with the duration of the disease.
This study indicates that ageing per se does not necessarily lead to a progressive elastase/α1‐antitrypsin imbalance in asthma, and suggests that an important variable in the development of airway remodelling in both young and elderly asthmatics is represented by the duration of the disease.
This study was supported by a CNR-INSERM scientific cooperation grant and by the INOC.
Bronchial asthma is commonly considered a disease of theyoung; however, epidemiological evidence indicates that asthma is not rare in elderly subjects 1. One of the most important characteristics of ageing lung is the loss of elastin fibres and of elastic recoil 2, 3. Increased elastin degradation has been demonstrated in the airways of young mild-to-moderate and severe asthmatics 4, 5, suggesting that the elastolytic activity in the bronchial mucosa is enhanced, possibly because of an imbalance between elastase and α1‐antitrypsin (α1‐PI); in addition, the increased levels of active elastase correlate with the degree of airway obstruction 6, suggesting a relationship between this biochemical imbalance and the development of long-term airway modifications, which may account for the increased rate of decline in forced expiratory volume in one second (FEV1) and for the loss of airway reversibility of bronchial obstruction 7–9. It is now well known that in bronchial asthma these changes are the result of a chronic inflammatory process; conversely, ageing is accompanied by a subclinical lower respiratory tract inflammation, as demonstrated in asymptomatic, clinically normal volunteers of advanced age 10, 11. Therefore, ageing and asthma share, to some extent, some inflammatory and elastolytic processes; however, it is unclear whether these phenomena interact in elderly asthmatics.
To better understand whether ageing is associated with a specific inflammatory profile and an altered homeostasis of elastin in the airways, an evaluation of inflammatory cells, elastase and α1‐PI levels was undertaken in induced sputum of young and elderly asthmatics matched for duration of the disease, degree of baseline FEV1 and response to salbutamol. Two groups of young and elderly healthy subjects that matched asthmatics in terms of age acted as internal controls.
Methods
Subjects
Eleven young control subjects (median age 27, 25th to 75th percentiles 27–32 yrs), 10 elderly control subjects (67.5, 61–71 yrs), 22 young asthmatics (32.5, 24–45 yrs) and 10 elderly asthmatic patients (72, 67–75 yrs) were studied. Asthma was diagnosed on the basis of criteria as described previously 12. To avoid any potential inclusion of subjects with concomitant chronic obstructive pulmonary disease, only those who showed an improvement of FEV1 of >12% from baseline or an absolute value of 200 mL following inhalation of 200 µg of salbutamol were included in the study. For the same purposes, smoking habit was carefully evaluated, and no current or previous smokers were recruited. According to a previous study 13, asthmatics were matched for the duration of the disease, the degree of airway obstruction as assessed by FEV1, and the degree of reversibility of airway obstruction (table 1⇓).
Demographic characteristics of patients
Patients were excluded from the study if they had undergone a severe exacerbation of asthma requiring hospitalisation during the month preceding the study. Inhaled corticosteroids or oral corticosteroids had been withdrawn for at least 2 months prior to the commencement of the study, while the use of nedocromil sodium or cromoglycate had been stopped for at least 2 weeks, and theophylline in the previous 48 h. The study was approved by the appropriate Ethics Committee and the patients gave informed consent.
Induced sputum production and processing
Induced sputum production and processing were carried out according to a previously published method 6. The safety of sputum induction was carefully assessed during this study in elderly asthmatics. After processing, the homogenised sputum was centrifuged at 800×g for 10 min to separate the supernatants from the cell pellet. The supernatants were frozen at −20°C for subsequent biochemical analysis. The cell pellet was resuspended in saline solution and the cell viability was assessed by Trypan blue exclusion. Cytocentrifuged cells were then stained by Diff Quick® (Merz-Dade, Dudingen, Switzerland) for differential cell counts. The slides were blindly read by counting ≥400 cells per slides by two independent investigators. The number of the squamous cells was subtracted from the total cell counts and the differential cell counts were expressed as corrected percentage.
Biochemical analysis of sputum
Total elastase was measured by enzyme immunoassay specific for human polymorphonuclear elastase (Ecoline; Merck, Darmstadt, Germany) using the package insert 6, 14. In addition, to assess the effect of metalloelastases from bacterial or macrophages sources on the assay system, the inhibitory profile of active elastase was determined by 30 min of preincubation of the sample with 0.4 mM methoxysuccinyl-Ala-Ala-Pro-Val-chloromethyl ketone (Sigma Chemical Co., St Louis, MO, USA) and 50 mM ethylenediamine tetraacetic acid (EDTA) 6. The lower detection limit of the assay was 20 µg·L−1. Neutrophil elastase activity was measured according to the technique of Fujita as described previously 9, 15 using the specific substrate methoxy-succinyl-Ala-Ala-Pro-Val-p nitroanilide (Sigma). The lower detection limit of the assay was 0.04 µg·mL−1. α1‐PI in sputum was detected by a nephelometric assay (Beckman array protein system; Beckman Instruments, Fullerton, CA, USA) using specific monoclonal antibodies 16. The lower detection limits of the assays were 2.8 µg·mL−1.
Statistical analysis
Results are expressed as median and 25th to 75th percentiles. Mann-Whitney U‐test was used to assess differences between groups. Spearman rank correlation was calculated to evaluate the correlation between outcomes. p‐values ≤0.05 were considered significant.
Results
Demographic characteristics of the patients
FEV1 values were higher in young than in elderly control subjects (p<0.003), whereas in asthmatics FEV1 values were similar in young and elderly subjects. Median FEV1 values in young asthmatic patients were 84% of predicted values (73–98%) (table 1⇑) and in elderly asthmatic patients 73.5% (52–91%). In both young and elderly subjects FEV1 was inversely correlated with the duration of the disease (p<0.04 and p<0.02, respectively, Spearman rank correlation).
Total and differential cell counts in sputum
The percentage of squamous cells was not significantly different in sputum samples obtained from elderly and young control and asthmatic subjects (table 2⇓). The corrected median total cell counts were similar in the four groups. The median viability of sputum cells was similar in the four study groups (table 2⇓). The differential counts of sputum cells were similar in young and elderly control subjects (table 2⇓), except for neutrophils, whose percentage was higher in the elderly than in the young (p<0.02), and macrophages whose percentage was higher in the young than in the elderly (p<0.02). Conversely, the differential counts of sputum cells were not statistically different between young and elderly asthmatics. The percentage of neutrophils and eosinophils was significantly higher in young asthmatics than in young controls (p<0.003 and p<0.0001, respectively) as well as in elderly asthmatics than in elderly controls (p<0.05 and p<0.0003, respectively; table 2⇓). Finally, in both young and elderly asthmatics the percentage of neutrophils was directly correlated with the duration of the disease (p<0.002 and p<0.03, respectively).
Cell analysis of sputum samples
Total and active elastase
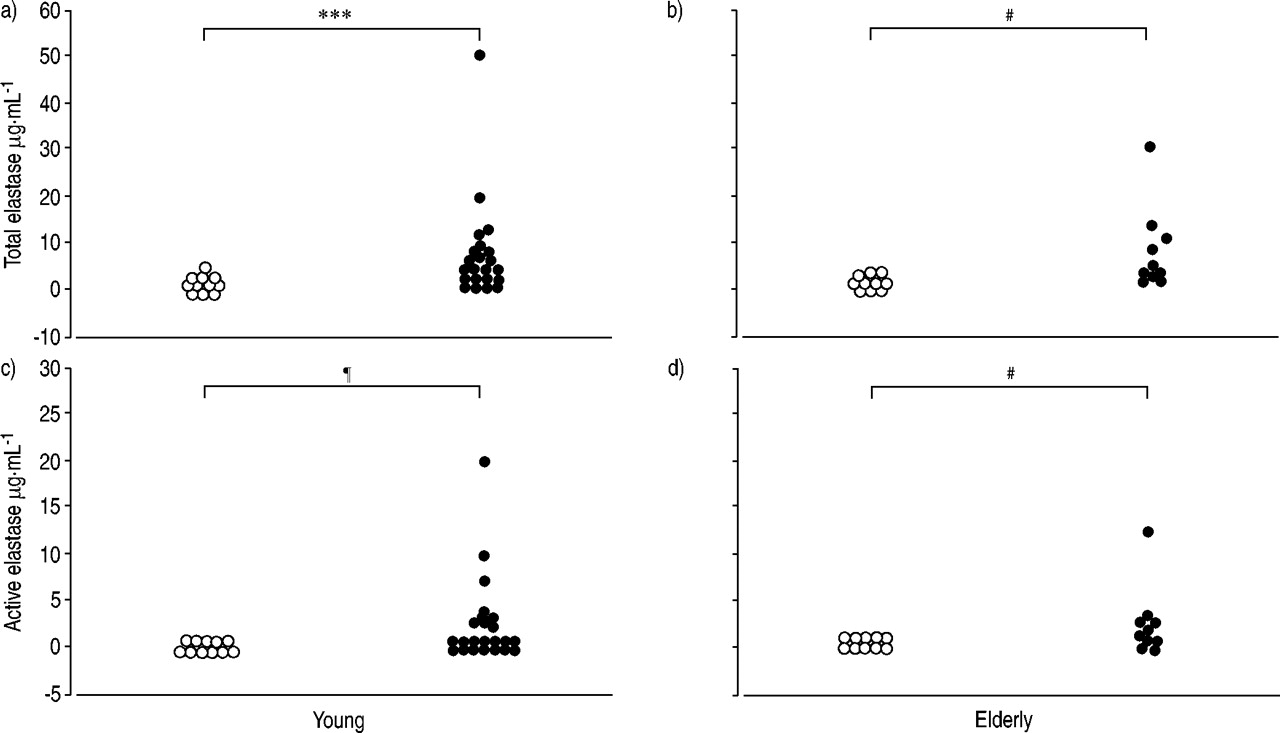
Total elastase levels were significantly higher in young asthmatics (4.75 (2.6–8.6) µg·mL−1) than in healthy controls (1.21 (0.9–1.4) µg·mL−1, p<0.001). Similar results were obtained in elderly asthmatics (4.9 (3.2–10.9) µg·mL−1) when compared with the control group (1.7 (1.3–2.8) µg·mL−1, p<0.003). Active elastase levels were 0.96 (0–3.1) µg·mL−1 in young asthmatics and 1.5 (0.4–2.9) µg·mL−1 in elderly asthmatics, whereas no levels were detected in the healthy control groups. Both total and active elastase levels did not differ between the young and elderly asthmatic groups. Similar comparison within the healthy control groups did not yield any significant difference (fig. 1⇓). When total and active elastase levels were plotted against the percentage of neutrophils, significant correlations were found (young asthmatics: total elastase p<0.05, active elastase p<0.009; elderly asthmatics: total elastase p<0.02, active elastase p<0.02; fig. 2⇓).

Levels of total elastase and active elastase in sputum obtained from both young (a and c) and elderly (b and d) control (○) andasthmatic (•) subjects. Statistical analysis was performed using the Mann-Whitney U‐test. ***: p<0.001; #: p<0.003; ¶: p<0.002.
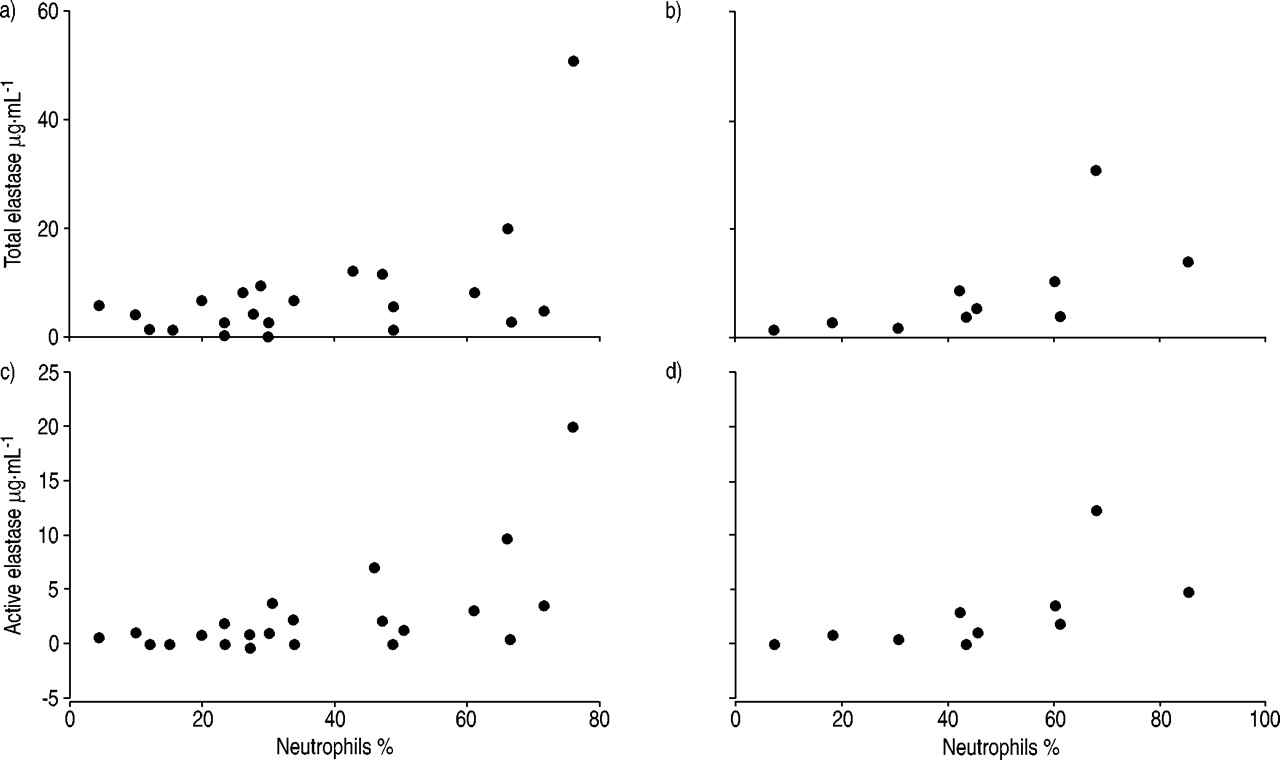
Correlation between levels of total elastase and active elastase and percentage of neutrophils in sputum obtained from young (a and c) and elderly (b and d) asthmatic patients. Statistical analysis was performed using Spearman's rank correlation test: a) rho=0.4, p<0.05; b) rho=0.8, p<0.02; c) rho=0.6, p<0.009; d) rho=0.8, p<0.02.
Interestingly, total and active elastase levels also correlated with the degree of baseline airway narrowing (expressed as FEV1 % pred), not only in young asthmatics (total elastase p<0.02, active elastase p<0.003), but also in elderly asthmatics (total elastase: p<0.03, active elastase: p<0.05; fig. 3⇓). As shown in figure 4⇓, similar results were obtained when the duration of disease was analysed (young asthmatics: total elastase p<0.004, active elastase p<0.003; elderly asthmatics: total elastase p<0.006, active elastase p<0.004). Since, in each group, one subject showed total and active elastase levels apparently out of range, the analysis was performed again by taking out the data from those individuals. When FEV1 represented the outcome of the regression, the results of the analysis did not change for young asthmatics (total elastase p<0.01, active elastase p<0.003), whereas, for elderly asthmatics, the relationship became weaker (total elastase p<0.06, active elastase p<0.18). This leads to the possibility that in elderly asthmatics airflow limitation is a more complex phenomenon, in which elastase plays a secondary role. Conversely, the exclusion of the “outliers” did not change the significant relationship between the levels of elastase (active and total) and the duration of asthma, further supporting the role of length of exposition to remodelling changes (for young asthmatics: total elastase p<0.007, active elastase p<0.005; for elderly asthmatics: total elastase p<0.01, active elastase p<0.009).

Correlation between levels of total elastase and active elastase in sputum and forced expiratory volume in one second (FEV1) per cent values in young (a and c) and elderly (b and d) asthmatic patients. Statistical analysis was performed using Spearman's rank correlation test: a) rho=−0.6, p<0.02; b) rho=−0.7, p<0.03; c) rho=−0.7, p<0.003; d) rho=−0.7, p<0.05.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Correlation between levels of total elastase and active elastase in sputum and duration of the disease in young (a and c) and elderly asthmatic patients (b and d). Statistical analysis was performed using Spearman's rank correlation test: a) rho=0.6, p<0.004; b) rho=0.9, p<0.006; c) rho=0.7, p<0.003; d) rho=0.9, p<0.004.
In young and elderly controls, the levels of α1‐PI were often undetectable. In contrast, the levels of α1‐PI were not different in sputum obtained from young and elderly asthmatic subjects (9 (8–18) versus 8.45 (5–13) µg·mL−1, respectively).
Finally, the ratio of total elastase over α1‐PI was pooled against FEV1 and duration of the disease. The results of this analysis basically confirm the above-described relationships. Indeed, the regression analysis showed that the ratio of total elastase over α1‐PI significantly correlated with FEV1 (for young asthmatics p<0.02; for elderly asthmatics p<0.04), and with duration of disease (for young asthmatics p<0.0001; for elderly asthmatics p<0.02).
Discussion
The authors have previously demonstrated that elastase levels are significantly increased in asthmatic subjects, suggesting that this phenomenon could contribute to the occurrence of remodelling changes in the extracellular matrix of the lung. However, since the study population consisted of young asthmatics, the question of whether ageing processes could influence the balance between elastase and α1‐PI was addressed. Herein, the authors have shown that the levels of elastase do not differbetween young and elderly asthmatic subjects, and are often undetectable in elderly, as well as in young, healthy subjects. Moreover, elastase levels were found to positively correlate with the duration of asthma and negatively with FEV1 values, both in young and in elderly asthmatic subjects.
An imbalance between proteinases and their inhibitors has been reported in individuals with airway inflammation 15, supporting the concept that this mechanism is a feature of chronic bronchitis. A wealth of evidence has accumulated to date to confirm that this phenomenon also occurs in the airways of asthmatics; indeed, an abnormal elastic fibre network, in which connective fibres often appear fragmented, has been demonstrated in this disease 4, 5. It is reasonable to expect that the alteration of the elastic fibre network has important pathophysiological consequences in asthma. Airflow limitation that occurs in asthma can be described as acomplex phenomenon that derives from several factors, oneof which is represented by the elastolytic activity. The increased elastolytic activity in the airways of asthmatics could play an important role in the pathogenesis of airway remodelling and in the development of some functional abnormalities, such as the exaggerated airway narrowing 17. This is further supported by several studies in moderate and severe asthmatics, which show that loss of elastic recoil 18, the increased collapsability of the central airways in long-lasting asthma 19, the lack of distensibility of airways 20 and hyperinflation 21 variably occur. In a recent study, Gelb and Zamel 21 have demonstrated the unsuspected loss of lung elastic recoil in severe asthmatics, which develops via unknown mechanism(s). Therefore, it is not unlikely that elastase may induce changes of the elastic fibre network of the lung of asthmatic subjects, thus affecting lung function, as shown by the present study.
However, the relationship between airflow obstruction and structural alterations of the airways cannot be solely attributed to changes in the elastic component. Furthermore, it is unknown to what extent the pathological abnormalities of the large and small airways account for airway narrowing. In this respect, structural changes of both the large and small airways have been described by Carroll et al. 22 in cases of fatal asthma. The increased thickness of airway wall area resulted from hypertrophy of all components of the airways (smooth muscle, submucosal areas, mucus glands), most likely as a response of different tissue to airway wall inflammation. These abnormalities could affect the lung function for geometric reasons, in that, excessive narrowing occurs for a given degree of muscle shortening 23; in addition, the possibility exists that the increased amount of smooth muscle causes greater shortening 24. This phenomenon could be further enhanced by the interaction between airway smooth muscle and mast cells. Interestingly, a recent study 25 has demonstrated increased mast cell infiltration within the airway smooth muscle, suggesting a key role of these cells in the development of airflow obstruction, and in the modulation of asthma severity 26. Finally, the possibility that increased production of mucus leads to excess lumen plugging cannot be excluded. Therefore, different structural abnormalities of the airways can be selectively associated with the asthmatic phenotype, and interact to induce airway obstruction. The relationship between such structural abnormalities and the severity of asthma, and the selective contribution of small versus large airway changes to airflow obstruction need further elucidation.
To address the effect of age on the balance between elastase and α1‐PI, two groups of asthmatic subjects of different ageswere compared. Both groups were characterised by a comparable, though variable, duration of disease (from 7–16 yrs in young asthmatics and from 8–16 in elderly asthmatics), and a similar degree of functional impairment. The induced sputum technique was chosen due to its relatively low invasiveness; indeed, the procedure was well tolerated by elderly subjects and in no case was the procedure interrupted because of induction of an asthmatic reaction.
Ageing is associated with structural and functional alterations of the lungs 2, 3, 27. Lung function deteriorates with age and is associated with reduction in elastic recoil pressure 2. The rearrangement of the elastic fibre network in the lungs of elderly asthmatics may contribute to reduce the mechanical interdependence between the airway and the parenchymal structures, thus leading to excessive airway narrowing. In this scenario, the structural alterations in lung elasticity associated with ageing could result in enhanced bronchoconstriction during an attack of asthma. This is confirmed by recent observations showing that, despite the same degree of baseline pulmonary function and airway hyperresponsiveness, elderly asthmatics have higher bronchial reactivity than young asthmatics, as expressed by changes in forced vital capacity 28. A low-grade inflammation has also been demonstrated in the airways of many asymptomatic, clinically normal elderly individuals 11. Since the neutrophil represents the major source of elastase in human lung 29, the question is raised whether the cellular abnormalities of the airways related to ageing processes, although not clinically evident, could interfere with the elastolytic activity. In this context, the neutrophil elastase‐α1‐proteinase inhibitor complex in bronchoalveolar lavage fluid was markedly elevated in asymptomatic smokers 30; in this population, an accelerated decline in FEV1 was detected in those subjects who showed higher levels of the elastase‐α1‐proteinase inhibitor complex, favouring the hypothesis that neutrophil elastase in the lung is related to the onset and/or progression of chronic bronchial diseases.
The main result of this study lies in the fact that the levels of both total and active elastase in the elderly asthmatic subjects do not differ from those that were found in young asthmatics, questioning the role that ageing can play as a factor amplifying neutrophil activation. Thus, these results imply that age per se does not affect the production of elastase. Conversely, ageing appears to influence the cellularity of the induced sputum of elderly healthy subjects. Indeed, in elderly subjects the percentage of neutrophils was higher than that of young subjects. The low levels of elastase in subjects with a high percentage of neutrophils could be explained with the lack, in healthy subjects, of an activation step in the production of elastase. An increase in α1‐PI levels was also detected in sputum samples obtained from young and elderly asthmatic patients compared with control subjects, which may depend on a compensatory response to the high levels of active elastase, although the former were not able to counterbalance the increased levels of elastase; in fact, in both young and elderly asthmatics high amounts of active elastase still persisted.
Interestingly, the duration of asthma significantly affects the levels of elastase. In the current study in young and elderly asthmatics, this parameter correlated with the levels of elastase. Hence, it is likely that the duration of the disease is the factor that exerts a major influence on lung function impairment. As discussed below, the loss of airflow obstruction reversibility and the decline of lung function can be explained with permanent and progressive remodelling changes with age; this would also explain why the functional impairment in asthma is a function of the duration of the disease. These results confirm previous findings obtained by the present group 31 and are in keeping with a recent study that shows that, in elderly asthmatics, subjects with asthma of long duration had a significantly lower FEV1 than those with asthma of a short duration, as well as a greater degree of lung function decline 32. In addition, the same study showed that most subjects with asthma of a long duration failed to achieve normal airflow after bronchodilator administration, which indicates that airflow limitation associated with long-term asthma may become irreversible, and suggests that long-standing asthma is characterised by an increased extent ofairway remodelling. This concept is also supported by histopathological studies that demonstrate an increase in airway wall area, including smooth muscle 22 and airway narrowing with increasing duration of severe asthma 33. Therefore, the duration of the disease appears to be the time variable affecting the baseline airway calibre, independently of the age of the patient. The significant correlation between the levels of elastase and the duration of asthma supports this hypothesis and provides novel information on the pathogenic mechanisms involved in remodelling of the extracellular matrix in asthmatic subjects.
Finally, the relationship between elastase and the degree of airway obstruction needs to be explained. Both in young and in elderly asthmatic subjects, the levels of elastase inversely correlated with FEV1 values, thus suggesting that, independently of age, elastase/α1‐PI imbalance may play an important role in the development of airway obstruction. Taken together, these findings strongly support the concept that, in the asthmatic condition, the alteration of the mechanisms involved in the degradation of elastin does not appear to be enhanced by the process of ageing.
To conclude, this study shows that the imbalance between elastase and its main inhibitor α1‐antitrypsin, as well as the degree of airway inflammation, is similar in young and elderly asthmatic subjects, and that the duration of the disease is one of the major factors implicated in the development of airway remodelling in asthmatics.
- Received December 4, 2002.
- Accepted July 13, 2003.
- © ERS Journals Ltd
References









