





Abstract
Cryotherapy, brachytherapy and photodynamic therapy (PDT) are three different methods proposed in the endoluminal treatment of lung cancers. The current article presents an overview of the specific indications and limits of each technique.
These three methods were first proposed with palliative intent in inoperable patients with centrally located lung cancers. Now, the best indication is a curative intent in early stage lung cancers.
Of the three, cryotherapy is the cheapest method. It induces cell necrosis in a 3-mm radius around the probe, and is suitable for treatment of superficial tumours. However, clinical trials are limited. In contrast, many clinical studies have confirmed the efficacy of PDT in treatment of superficial lung cancers. Brachytherapy can cure more aggressive tumours with deeper invasion into the bronchial wall. Unfortunately, no comparative studies have been published. Each of these methods induces a delayed tumour necrosis, and thus neither is indicated in the treatment of obstructive tumours with acute dyspnoea. In many situations, these methods should be complementary, particularly cryotherapy and brachytherapy or PDT and brachytherapy.
The combination of these endoscopic methods with chemotherapy should be widely tested to promote the adjuvant role of the endoscopic methods in the treatment of lung cancers.
SERIES “INTERVENTIONAL PULMONOLOGY”
Edited by J.P. Janssen, M. Noppen and K.F. Rabe
Number 2 in this Series

Cryotherapy, brachytherapy and photodynamic therapy (PDT) are three different endobronchial techniques with specific indications. Each of them induces a delayed response, and thus is not indicated in the treatment of obstructive tumours with acute dyspnoea. The aim of the present paper is to describe each method, its indications and limits, enabling selection of the best treatment option for each situation encountered.
CRYOTHERAPY
Compared with other methods used to treat endobronchial tumours, cryotherapy is unique. This method offers delayed tumour destruction similar to PDT at a cost cheaper than electrocautery, and with the safety of not inducing collagen damage or bronchial wall perforation. Cryotherapy is therefore used to treat infiltrative tumours, including in situ cancers. The specific action of cryotherapy on apoptosis and on poorly vascularised tumour cells allows the use of cryotherapy in combination with irradiation or chemotherapy.
Background
The analgesic and anti-inflammatory properties of cold have been known for centuries. Larrey used these properties in 1812 to achieve haemostatic and analgesic effects in surgical amputations during the Russian campaign. In 1851, Arnott 1 made reference to the role played by low temperatures in destroying tumours. In 1959, the first clinical application on brain tumours using closed-circuit probes was published 2. Later on, cryotherapy was widely used in the treatment of a variety of tumours. In 1968, Gage 3 reported the first endoscopic treatment on a bronchial tumour in the USA. Both articles 2, 3 received little attention, despite the fact that there were several publications from 1962 to 1983 4–8 dealing with the same subject. Laser therapy was preferred. Bronchial cryotherapy was renewed in France in 1986, following studies by Homasson 9. Since then, >1,500 patients have been treated in France and the UK 10–14. Based on this clinical experience, the techniques and limits of cryotherapy were defined on both bulky tumours and in early stage lesions. The combination of cryotherapy with irradiation or chemotherapy was then tested in humans and produced encouraging results 15, 16. Since 1996, interest in cryotherapy has grown in the USA with the introduction of flexible probes 17. Currently, the cytotoxic mechanisms of cryotherapy and the potential for synergistic action with chemotherapy are being investigated through in vivo studies 18.
Principles
Cryotherapy is a unique method of destruction based on the cytotoxic effects of cold on living tissue. The application of a low-temperature probe on a tissue first induces an immediate adherence between the probe and the tissue and then the appearance of intra- and extracellular ice crystals 19–23. These crystals damage intracellular organelles, especially mitochondria. The formation of pure extracellular ice crystals causes additional ion and water movements resulting in cellular dehydration. In order to obtain a maximum lethal effect, it is necessary to have large ice crystals, especially at the intra-cellular level. This effect is achieved by rapid cooling of the tissue followed by slow thawing 10. This principle is the opposite of cryopreservation. In tumour tissue, thawing occurs by vascularisation, where cold waves move radially around the point of application of the cryoprobe. At each point, cytodestruction varies according to the speed of freezing and thawing. Cytotoxicity diminishes with distance from the centre of application, as well as when near the permeable vessels 18, 19. This physical and cellular phenomenon is coupled with a vascular effect: an initial vasoconstriction occurs, which is followed by a vasodilatation. A complete vascular thrombosis appears 6–12 h later, thus completing the physical cytodestruction by induction of local infarction 19–23.
In the more peripheral area, the destruction is inhomogeneous, and the vessels that remain permeable protect some perivascular cells from destruction 21. It has been demonstrated that apoptosis is the main phenomenon in this zone 18.
The area of destruction through cryotherapy has a diameter of ∼1 cm when a 3-mm diameter probe is used 9. When in lateral contact with a bronchial wall, cytotoxicity can be considered complete to a depth of 3 mm. Nonhaemorrhagic necrosis of the tissue occurs 8–15 days following the procedure. Collagen, cartilage or poorly vascularised tissues are very cryo-resistant 11.
These data explain the essential characteristics of cryotherapy: a spherical pure cytotoxic action leading to late tissue necrosis and an important late haemostatic effect. The high cold resistance of the supporting bronchial structure explains the safety of this method. There is neither risk of bronchial perforation nor scarring with residual fibrous stenosis. The cold wave kills poorly vascularised cells and spares perivascular cells. Thus, the vascular density increases in the residual tumour. The current author also observed an enhancement of vascular endothelial growth factor expression in the residual tumour cells. These results support the principles of cryo-radiotherapy 16 and cryo-chemotherapy studies 15.
Materials and methods
Devices
Two types of probes are available: liquid nitrogen probes, which are very powerful but awkward to use, and nitrous oxide (N2O)-driven cryoprobes (figs 1⇓ and 2⇓). Cooling is due to the Joule–Thompson principle, cooling of a gas by sudden expansion from a high to a low pressure zone. Flexible cryoprobes of 2–3 mm in diameter are available and can be used through a flexible fibreoptic bronchoscope 18. Recently, reinforced cryoprobes were manufactured in order to extract pieces of tumour after the adherence phase 24. Personally, the present author prefers and recommends rigid cryoprobes used through a rigid bronchoscope. The rigid cryoprobe is more powerful than the flexible probe. A footpad or a trigger on the handle allows immediate and active thawing of the probe after cooling. This contrasts with flexible probes where thawing is passive. Thus, with flexible probes, each cycle of freezing and thawing lasts double the amount of time compared with a rigid probe cycle. The rigid probe used by the present author is 60 cm long and 3 mm in diameter. Only the 1-cm tip of the probe causes freezing of tissues; the remainder of the probe is insulated. The external temperature obtained at the tip of the probe is <-40°C and is obtained in 1–2 s 22, 23. The probe is connected to a cylinder of purified N2O at a pressure of 50 bar. The main equipment is supplied by ERBE (Tübingen, Germany), but other equipment is supplied by DATE (La Motte d’Aveillans, France) or Spembly Medical Ltd (Andover, UK).
Methods
In St. Etienne University Hospital (St. Etienne, France), the patients are admitted to hospital the day before the treatment and discharged the following day. Procedures are performed by introducing the rigid cryoprobe into a rigid bronchoscope. High oxygen concentration can be delivered without any restriction during cryotherapy. Local anaesthesia alone is used when cryotherapy is performed through a flexible bronchoscope. It is notable that cryotherapy is not a painful procedure. Once the lesion to be removed is found, the tip of the cryoprobe can be pushed into the protruding exophytic tumour or applied laterally onto infiltrative tumours and in situ carcinomas. Generally, three cycles of freezing and thawing are performed at each location. Each freezing period is short, at ∼20 s. When an impedance meter is used, the freezing phase is stopped once a plateau of impedance is obtained. After three cycles, the tip of the probe is moved to touch an adjacent part of the tumour. Although the obtained ice-ball is ∼10 mm in diameter, the adjacent impact of the probe must be ∼5 mm from the first impact to make the ice-ball overlap. It is important to cover the entire surface of the tumour (30 or more cycles are often necessary). In cases of early stage lung cancers, the limits of the lesion should be delineated by autofluorescence endoscopy. Without this technique, a margin of 5 mm around the visible limits of the tumour should be treated. In cases of tumour located on a carina, the two sides of the carina and the crest should be treated. At the end of the procedure, the tumour appears undamaged. Indeed, cryothrombosis is delayed for several hours. In the present author's opinion, it is dangerous to mechanically remove any part of the tumour at this stage. For this reason, cryotherapy is not recommended when patients present with an acute dyspnoea. Even in large tumour treatment, the duration of a cryotherapy session using rigid cryoprobe (with active “immediate” thawing) remains short, between 20 and 45 min.
Between 8 and 10 days after cryotherapy, the necrotic sloughed tissue is eliminated by expectoration or removed by forceps during a follow-up fibreoptic bronchoscopy. Generally, when cryotherapy is used alone, a second session should be planned to eliminate the residual tumour.
Indications and complications of cryotherapy
Indications
The effects of cryotherapy are delayed. This technique, therefore, is not indicated to achieve immediate debulking of an obstructive tumour. In these cases, the tumour will first be cored out mechanically with the tip of the rigid bronchoscope after coagulation (if necessary) with laser beam or electrocautery. After this first step, and in the same session, cryotherapy can be applied on the remaining infiltrative part of the tumour (fig. 3⇓).
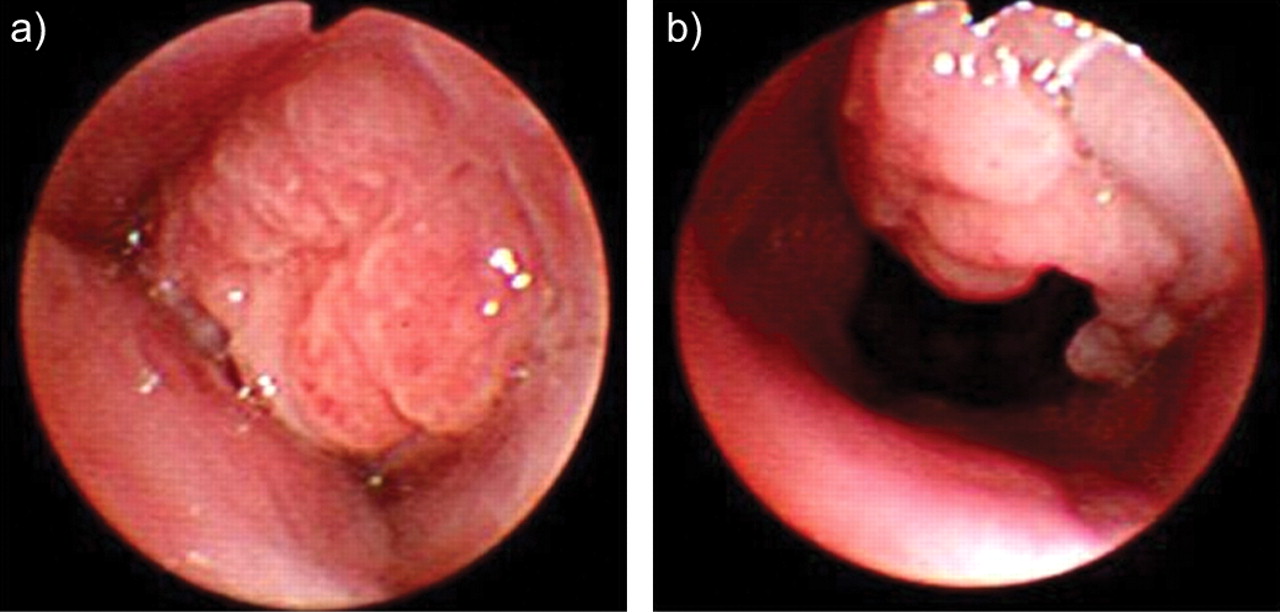
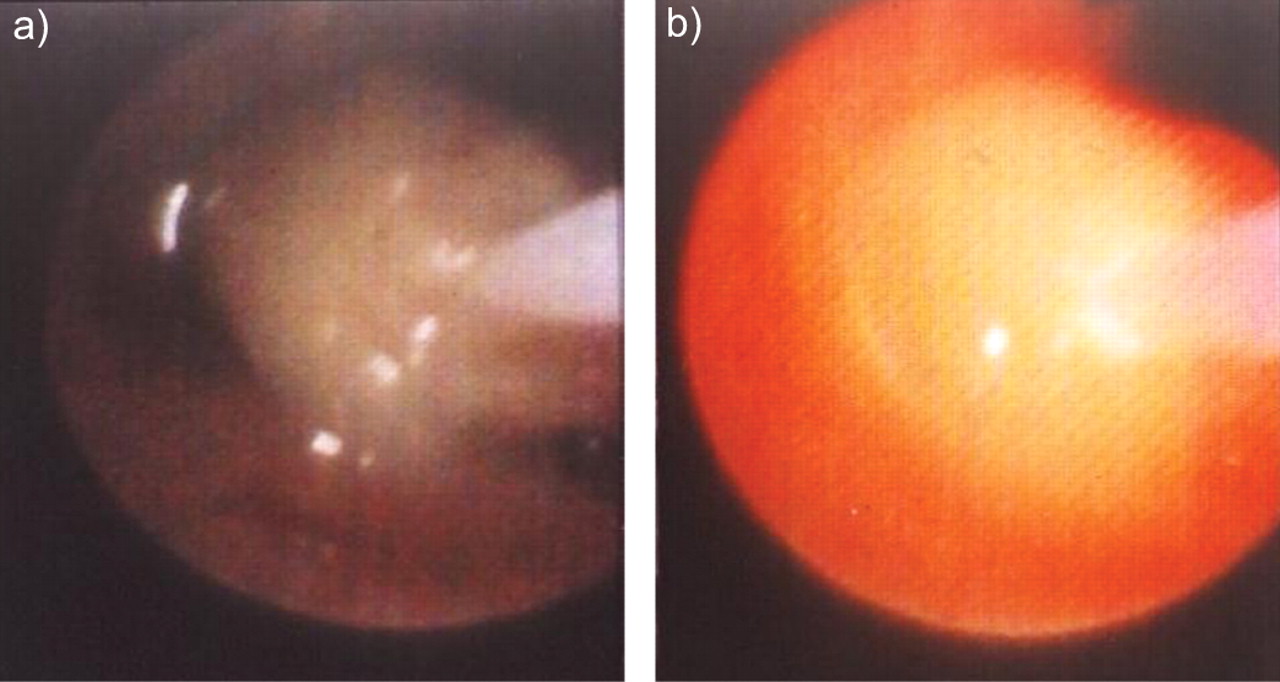
Cryotherapy is very efficient on cellular and well-vascularised tumours such as bronchial carcinomas, carcinoids (fig. 4a⇓ and b), adenoid cystic carcinomas or granulomas. In the present author’s experience, 18 cases of endoluminal typical carcinoids have been treated and cured with the combination of laser-assisted mechanical resection followed by cryotherapy. The median follow-up was 30 months. In lung cancers, the effectiveness of cryotherapy reaches ∼75%, regardless of the cellular type or the endoluminal aspect 12, 14, 19, 23. Due to the deep (3 mm) and safe cytotoxic action against tumour cells in the bronchial wall, this method can be used to safely treat in situ or micro-invasive carcinomas (fig. 2⇓). The results of a multicentre French study of 35 cases has been reported 25; an 80% complete cure with a mean follow-up of 32 months was observed. The remarkable action of cryotherapy on tumour vascularisation also explains its effectiveness on haemoptysis. The control ranged 60–86% 12, 19, 23.
The present author believes that this method of cryotherapy, as well as PDT, could now be dedicated to the treatment of stalks of resected tumours or early stage lung cancers.
Collagen tissue, poorly cellular tumours and fibrous scars are not so cryosensitive, thus cryotherapy alone is not indicated in benign strictures of the trachea or bronchi caused by fibromas, lipomas or post-intubation stenosis. Cryotherapy is not indicated in external compression of the bronchial tree. Cryotherapy is, however, useful to remove many foreign bodies from the airways (fig. 5⇓). Efficient cryo-adherence is observed with porous structures, such as pills, food, blood clots or peanuts. In contrast, cryo-adherence is less efficient with bones, metal or teeth.
Complications
Cryotherapy is a very safe method without risk of perforation or residual stenosis even after circumferential treatment. This contrasts with electrocautery which, even in soft mode, has a risk of perforation or residual stenosis. Two side-effects of cryotherapy have been observed. 1) A transient fever immediately following cryotherapy. Interestingly, this fever can be prevented by corticosteroid administration given during the procedure. The present author speculates that this fever could be associated with the cell necrosis and a release of tumour necrosis factor. 2) Airway-sloughing material elimination after cryotherapy remains a problem. A similar situation is observed with PDT. The sloughed tissue is often abundant, protruding into and even obstructing the airway lumen. It can induce cough and dyspnoea. A bronchial toilet with a flexible fibreoptic bronchoscope is recommended 8–10 days after cryotherapy.
Therapeutic associations
Cryotherapy may be of benefit in patients requiring chemotherapy or irradiation therapy, but this hypothesis needs to be proven. Preliminary reports both in animals and humans have shown that pre-treatment with cryotherapy could enhance the concentration of the chemotherapy agent into the tumour 15, 26. The benefit of combining cryotherapy with chemotherapy to enhance the induction of cell death either by necrosis or by apoptosis has also been found in a mouse model 18 (fig. 6⇓). With irradiation, a prospective pilot study has been conducted 16, suggesting that the cryotherapy irradiation combination induces a very effective endoluminal control of the tumour associated with an increased survival. This result was confirmed by another study conducted by Maiwand and Homasson 12. The same results were observed in mice (fig. 7⇓). Unfortunately, these preliminary studies have not yet been followed by larger randomised prospective protocols.
Conclusion
In 2006, compared with other endobronchial treatments, the role of cryotherapy was still limited. It is the safest and cheapest method but less versatile than electrocautery. It is an excellent method with which to treat early stage lung cancers, but experience is limited and should be confirmed by prospective randomised studies. In lung cancer, results of the combination between cryotherapy and chemotherapy or irradiation are very encouraging but require large prospective human studies.
BRACHYTHERAPY
Introduction
For each specific endo- or paraluminal tumour of the tracheobronchial tree, different methods of endobronchial intervention are available. These interventions should be quick, effective, suitable for the patient and the staff, and carry a low risk of complications, especially in the mostly palliative setting. One of these methods is endoluminal brachytherapy. Brachytherapy (brachys (Greek) meaning short) refers to the placement of a radioactive source (usually iridium-192 high dose rate (HDR)) within or near to an endobronchial/parabronchial malignancy to deliver local irradiation. The radioactive source can be implanted directly into the tumour, placed in the tumour bed after surgical resection or applied via the endoluminal endoscopic route. Endoscopic brachytherapy with a HDR system has the advantage of being a minimally invasive procedure, which can be performed on an outpatient basis. Also, it is suitable for patients with a poorer performance status. Furthermore, the equipment is not very expensive. The disadvantage is the time gap between intervention and the macroscopic effects on the tumour. Acute side-effects are very rare and are related to bronchoscopy itself; late effects may be bleeding, the formation of fistulas, radiation bronchitis and consecutive airway stenosis. It may be curative in very early superficial cancers. HDR brachytherapy can also be used for nonmalignant tracheal and bronchial obstruction. Brachytherapy can be combined with all other treatment modalities used in thoracic malignancies. The effect is not limited to the tumour in the lumen and is long lasting. Due to its small radiation volume and the rapid decline of the radiation dose, it is also indicated to palliate symptoms, such as cough, haemoptysis and dyspnoea, in patients who have already received their maximal dose of external beam radiotherapy (EBRT).
Background
Amongst the currently available interventional bronchoscopic procedures, endobronchial brachytherapy is one of the oldest techniques. The first successful endobronchial implantation of radium capsules (using the ideas from gynaecological implants) was documented as early as 1922, and further reports also on interstitial therapy have followed 27, 28. In the 1960s, cobalt-60 seeds were most frequently used as the radiation source. Both radium and cobalt implants deliver the dose with a relatively low dose rate and therefore require a long treatment time, up to days, which is not suitable for application in the airways. Also, rigid bronchoscopy and general anaesthesia are necessary.
By using brachytherapy, it is possible to deliver a maximum dose to the tumour with a minimum dose to the surrounding normal tissue. However, one of the major drawbacks of this method was found to be the high level of radiation to which the medical personnel were exposed. Therefore, the development of the remote afterloading technique in 1964 was essential for the widespread application of brachytherapy 29. The introduction of the iridium-192 radioisotope with the possibility of delivery with a HDR, and the refinement of the afterloading apparatus by using automated, computer controlled steering devices, has led to significant progress 30. The small size of the iridium source with its high activity (∼10 Gy at the beginning of the treatment) and HDR allows its placement in a hollow guidance catheter, which can be easily placed endoluminally by a flexible bronchoscope. Nevertheless, it was not until the widespread use of the neodymium yttrium-aluminium-garnet (Nd-YAG) laser recanalisation of tumour stenoses that endoluminal brachytherapy was used more frequently for the palliative treatment of endobronchial and parabronchial tumours. Here, brachytherapy stabilises the recanalising effect of Nd-YAG laser therapy. It can be used, either alone or in combination with other methods, in a more curative setting, such as early stage endobronchial tumours.
Performed by an experienced endoscopist, HDR brachytherapy has the same acute side-effects as routine fibreoptic bronchoscopy and, therefore, can be easily applied in an outpatient setting. Irradiation lasts only a few minutes.
Principles
Brachytherapy is a form of radiation therapy, where the irradiation source with a high dose is either within or very close to the malignant tissue. The primary radiation produced is gamma rays. The physical characteristics of these radioactive isotopes are characterised by the inverse square law which means that the dose rate decreases as a function of the inverse square of the distance to the source centre. This makes it possible to achieve a high irradiation dose in the centre of the irradiation source with a fast decrease towards the periphery. A typical distribution of isodoses is shown in figure 8⇓. Usually the effects of irradiation are not direct killing of the cells, but single chain breaks of the DNA resulting in apoptosis and a decrease in cell proliferation. Therefore, the visible effects of brachytherapy with iridium-192 HDR are delayed, with the maximum visible and histological changes taking place ∼3 weeks after application. These effects are clearly less pronounced in normal, nonmalignant tissue 31, 32.
Materials and methods
Devices
To position the radiation source an afterloading polyethylene probe is used, which is available in different diameters, usually 2–3 mm in external diameter. A removable dummy simulates the pathway of the radiation source during the radiologically controlled placement of the probe (fig. 9⇓). A vascular guide wire is helpful for placing the catheter and a tube, such as a shortened gastric tube, is helpful in avoiding direct contact with the normal tissue 33. Centring devices, such as balloons, cages or sheaths, can be employed to maintain the radioactive source within the centre of the bronchial lumen and avoid dose inhomogeneity 34. A HDR source with high activity of iridium-192 is usually used for endoluminal brachytherapy of thoracic malignancies. Remote brachytherapy is performed in a shielded room with permanent oxygen delivery to the patient, who is monitored from outside by continuous assessment of oxygen saturation, pulse rate or electrocardiogram and direct visual control via a video camera. After removal of the dummy seed, the applicator is connected to the iridium-192 remote afterloading unit containing the irradiation source. The radiation source (diameter of ∼1 mm) is advanced to the intended position under computer control and then drawn backwards at intervals of 5 mm. It remains in each position for the time needed to apply the computed dose. By varying the source position and dwelling time, individual computer-assisted dose distribution can be achieved (fig. 10⇓). The treatment can be interrupted and restarted whenever necessary.
Energy levels, dosages and fractionation
Until the mid 1980s a low energy radioactive source for brachytherapy was used. Now sources with higher energy are available, usually iridium-192. A distinction between radiation with different energy levels can be made using the terms low dose rate (LDR), medium dose rate and HDR. LDR brachytherapy implies delivery of <2 Gy·h-1 and a total dose of 1,500–5,000 cGy, given over a period of up to 3 days 8. Intermediate dose rates range ∼2–10 Gy·h-1 35. The International Commission of Radiation Units defines HDR as the application of >20 cGy·min-1 (1 rad = 1 cGy), which means a delivery of >12 Gy·h-1, with the dose per session (fraction) varying from ∼300–1,000 cGy (calculated at 10 mm from the source axis) 36.
Iridium-192 is the most commonly used source. As the source is in position for a shorter time, there is less chance the catheter will be displaced. A shorter treatment time also improves patient tolerance and reduces treatment costs. In contrast to LDR, HDR brachytherapy is usually delivered in a series of dose fractions in order to optimise its effectiveness and minimise side-effects. A wide variety of treatment schedules have been utilised; generally patients are treated no more than every 1–2 weeks because of the discomfort and logistical difficulties associated with more frequent bronchoscopies. There is only one controlled, randomised study to evaluate the effect of dose rate, overall radiation dose, fractionation and localisation of the afterloading catheter to survival rate, local control and complications. In the study 37, two treatment regimens with a comparable total irradiation dose of 15 Gy (at 1 cm from the source axis), but different doses per fraction (four fractions of 3.8 Gy on a weekly basis versus two fractions of 7.2 Gy at a 3 week interval) were compared. There were no disadvantages for the shorter fractionation regimen, with a similar survival time (19 weeks) and local control time in both groups. The complication rate was also similar, with fatal haemorrhage occurring in ∼21% of all patients.
Methods
In general, endoluminal brachytherapy using flexible bronchoscopy and an HDR regimen can be performed on an outpatient basis, as it is no more strenuous for the patient than a diagnostic bronchoscopy. In the case of LDR brachytherapy, hospitalisation for several days is usually required.
Preparations for the procedure
Flexible bronchoscopy is performed to localise the tumour region for irradiation. The afterloading catheters have an external diameter of 2–3 mm. lf there is subtotal stenosis of the bronchi due to submucosal or exophytic tumour growth, it is sometimes necessary to perform balloon dilatation or use other recanalisation methods for better applicator placement. If there has been previous laser treatment, it is recommended to wait ≥3 days before brachytherapy treatment can be initiated, although the debate about this issue is still ongoing 38, 39. Endoluminal irradiation should be delivered with a safety margin of ≥1 cm at both ends of the visible endobronchial tumour length. The active length refers to the distance between the first and last dwelling point of the iridium source in case of HDR brachytherapy. As the distal end of the tumour cannot always been seen by the bronchoscopist, the distal end-point of the irradiation length must often be estimated from previous chest radiographs or computed tomography scans and controlled during bronchoscopy by fluoroscopy.
Placement of the applicator
The irradiation length is marked by external tags controlled by fluoroscopy. A guide wire is placed through the working channel of the bronchoscope, which is then removed. Manipulation of the guide wire and then of the applicator through a partially obstructed lumen requires skill, particularly within the upper lobe bronchi. However, with this technique areas can be reached that cannot easily be reached by other recanalising methods. For a better fit of the afterloading probe, a shortened gastric tube with an external diameter of 5 mm is usually inserted over the guide wire by the Seldinger technique. The gastric tube should be placed inside the tumour bulk. The irradiation applicator is then placed into the tube and taped to the tip of the nose to prevent it from being dislocated. This should be carried out under visual fluoroscopic control.
After placement of the afterloading probe, a dummy seed is inserted, and a set of orthogonal chest radiographs is obtained to document the correct placement of the catheter within the tumour bulk and to determine the necessary irradiation length, as indicated by the external tags (fig. 9⇓). The treatment dose is prescribed by the radiation oncologist, usually specified at a depth taken 1 cm from the middle of source axis 40. One of the technical challenges is the obvious difference in luminal diameters of different segments of the tracheobronchial tree. It is uncommon to adjust for these differences, but Saito et al. 41 attempted to answer this problem by setting distinct diameters at different segments of the tracheobronchial tree and adjusting the dose evaluation point to the lumen diameter at the lesion site.
After removal of the dummy seed, the applicator connected to the iridium irradiation source (diameter ∼1 mm) is advanced to the intended position under computer control, then drawn backwards at intervals of 5 mm. The source remains in each position for the time needed to apply the computed dose. By varying the source position and dwell time, an individual computer-assisted dose distribution can be generated (fig. 10⇓).
Follow-up
The maximal effect of a brachytherapy session is seen after ∼3 weeks. Therefore, a follow-up bronchoscopy is usually performed 3–6 weeks after the end of the planned treatment series.
Indications and complications of brachytherapy
Indications
The effects of brachytherapy are delayed. First effects can be seen after ∼1 week, and the maximum effect is only achieved after ∼3 weeks. However, brachytherapy probably has a longer-lasting effect and has greater tissue penetration than other tumour lysis techniques. It also destroys tumour outside of the bronchial wall and behind cartilage. HDR brachytherapy has the advantage of delivering a high dose of radiation over a short period of time to the tumour area without significantly affecting the adjacent lung parenchyma.
This technique is not indicated to achieve immediate debulking of an obstructive tumour. Therefore, in central tumours with imminent tracheal or bronchial occlusion, methods which rapidly destroy the tumour or stenting have to be applied. Thereafter, brachytherapy can be performed to achieve a longer-lasting effect on the tumour both inside and also outside the bronchial wall. Contraindications to endobronchial brachytherapy include the presence or the imminent danger of fistulas between bronchi and other structures.
Palliative setting
In most cases, brachytherapy is applied in a palliative setting. This is the case in metastatic diseases of patients with poor performance status. HDR endobronchial brachytherapy is then considered a palliative technique for alleviating dyspnoea resulting from major airway obstruction by primary and secondary malignant tumours. It is also indicated to palliate symptoms, such as cough, haemoptysis and dyspnoea, in patients who have received their maximal dose of EBRT.
Curative indications
Brachytherapy can be applied after surgery if there are microscopically positive resection margins.
Brachytherapy can also be used as an endobronchial boost to EBRT 41–45. HDR brachytherapy has been primarily used for previously untreated patients in conjunction with EBRT, often to quickly relieve obstruction and to reduce the volume of irradiated normal lung tissue. Brachytherapy can help to reduce the permanent fibrosis of normal lung tissue due to large external irradiation fields, particularly when atelectasis due to obstruction of a main or lobar bronchus is obscuring the true tumour margins. It has been calculated that this procedure can reduce the irradiation of normal tissues by an average of 32% 46. Apart from treatment for local stenosis, brachytherapy has the potential to increase local control and survival time when used in combination with external irradiation. Although none of the studies published so far could demonstrate a clear advantage in terms of survival in nonselected patients treated with this combined modality, there are indications that at least local control is better in patients with additional endoluminal brachytherapy 47.
In very early superficial cancers, brachytherapy may be curative. Surgical resection is widely accepted as the treatment of choice in early stage nonsmall cell lung cancer (NSCLC). However, when occult carcinoma in situ or small invasive endobronchial lesions are discovered incidentally by bronchoscopy, mostly due to symptoms like cough or haemoptysis, HDR brachytherapy, either alone or as a boost to EBRT 41, offers a treatment option with good results, low morbidity, low cost and little inconvenience for the patient. Especially in carcinoma in situ or limited invasive tumours without nodal involvement, HDR brachytherapy could represent the definite treatment due to the deeper and unrestricted penetration. As with other treatment modalities, data published on intraluminal brachytherapy in early stage NSCLC are limited 41, 47–51.
Nonmalignant indications
HDR brachytherapy can also be used for nonmalignant tracheal and bronchial obstruction. Typical applications are the treatment of recurrent granulation tissue formation in and around a stent or of granulation tissue at the bronchial anastomosis after lung transplantation 52, 53.
Effectiveness
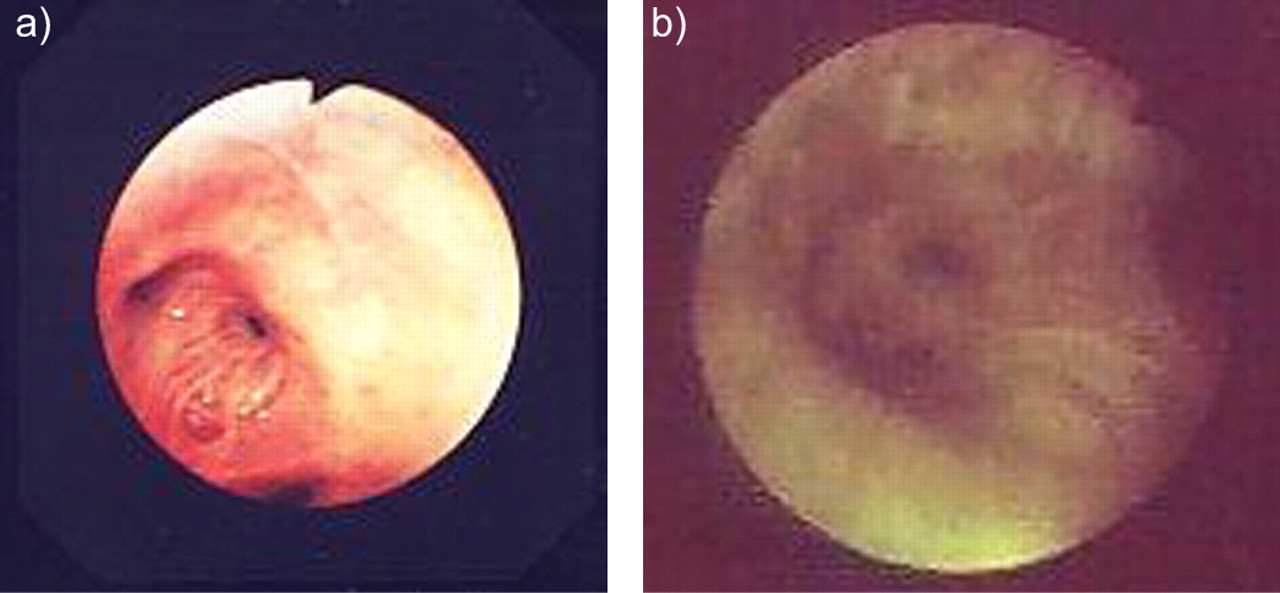
In palliative indications, overall improvement and disappearance of symptoms has been shown in 65–95% of all patients. Haemoptysis can be treated with a high rate of success; this is also true for the reopening of obstructed bronchi. Improvement of cough, shortness of breath and pain was observed to a lesser degree. Palliation can be maintained in a high proportion of patients 35, 39, 43, 45, 54, 55. This can also be verified by bronchoscopy (fig. 11a⇓ and b) or lung function testing 56–58. There are even hints for survival advantage in selected cases 42, 59.
Complications
Acute side-effects of the placement procedure include severe coughing and increased bronchial secretion. They are not more frequent than those occurring during routine diagnostic flexible bronchoscopy. The placement of the afterloading catheter and the following remote irradiation procedure in the HDR setting are usually well tolerated. However, patients with poor performance status and severe respiratory failure are at higher risk due to the prolonged procedure.
Temporary pleuritic pain or even pneumothoraces have been described when the guide wire or the applicator were placed too vigorously. However, the present author has never observed such serious side-effects during >2,000 placements of afterloading probes.
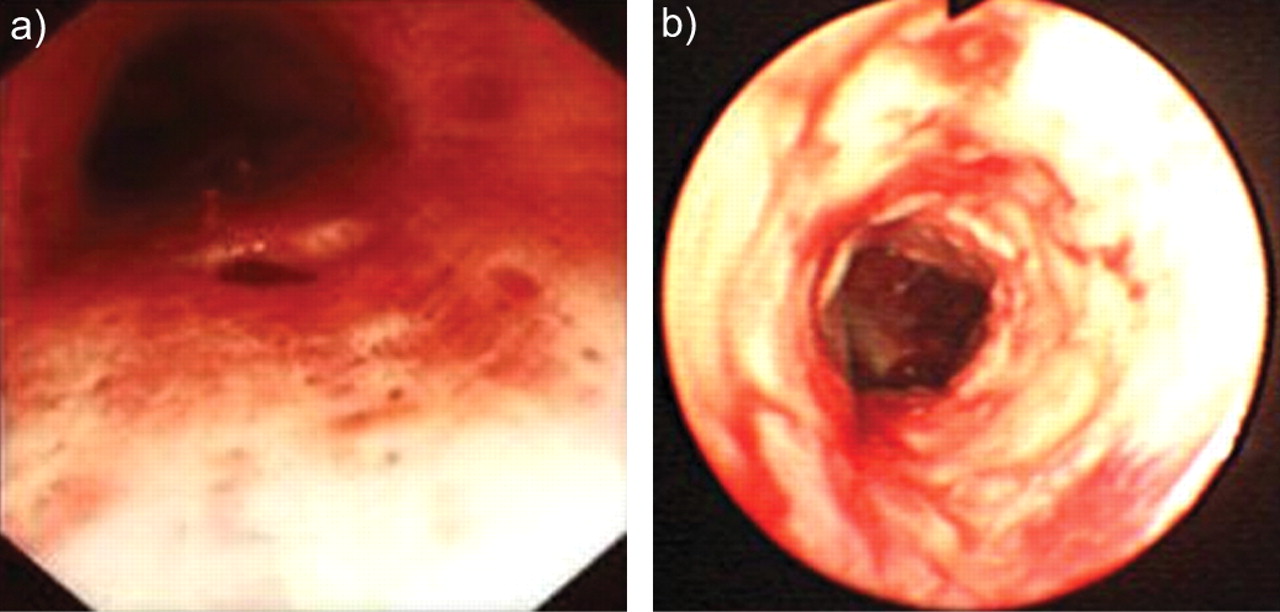
As with EBRT 59, radiation bronchitis and stenosis may occur days or weeks after therapy and can manifest with cough or wheezing (fig. 12⇓). Histological changes consist of mild mucosal inflammation to severe bronchial fibrosis. Risk factors include large cell carcinoma histology, use of brachytherapy for curative intent, prior laser resection and concurrent external beam radiation 35. Overall bronchial stenosis has been shown to occur in ∼10% of patients after HDR EBRT for lung cancer 60. Therapy of these post-radiation effects consists of conventional treatment, such as inhaled steroids and antibiotics, or, for stenosis, balloon dilatation, laser resection and stenting.
The most important potential side-effects of brachytherapy are fatal haemoptysis and fistula formation. Such adverse outcomes are reported in 0–32% of patients, with an overall prevalence of ∼10% 56. For the interpretation of these figures, it should be kept in mind that most of the studies published are not randomised and are not even prospective. The studies use different selection criteria concerning pre-treatment, catheter placement, dosages, fractionation, localisation and histology. The occurrence of fatal haemoptysis is usually considered as a complication of treatment and not related to the disease itself. However, the data on the natural course of lung cancer is sparse and it is often difficult to differentiate between treatment complications and tumour progression. One can argue that the incidence of fatal haemoptysis is related, for example, to tumour invasion into pulmonary vessels or related to the administered irradiation dose and fractionation regimen or even to the longer survival of the patients who receive brachytherapy. Squamous histology and tumour localisation in the mainstem bronchi predispose to fatal haemorrhage 61, 62. This localisation represents a further negative selection towards more frequent haemorrhages. It is possible that the combination of external and endoluminal irradiation increases the frequency of haemorrhages. However, one randomised trial could not demonstrate a statistically significant difference in comparison to external radiotherapy alone 27. One of the relevant factors for haemoptysis is the localisation of the radiation, especially the direct contact between the endobronchial brachytherapy applicator and the tracheobronchial walls at the vicinity of the great vessels 63. Furthermore, an increase of the dose per fraction over 10 Gy at a distance of 10 mm from the source axis increases the risk of bleeding dramatically 64.
In general, the incidence of fatal haemorrhage is high and all efforts to minimise potential side-effects of endobronchial brachytherapy should be strengthened. However, with usual dosages and fractionation, fatal haemorrhage seems to be correlated more with the natural course of a longer survival than with endoluminal brachytherapy itself.
Overall, endobronchial brachytherapy is easy to perform in an outpatient setting with little discomfort to the patient and can be considered a well-tolerated treatment option, especially in patients with reduced performance status.
Combination with other endobronchial methods and chemotherapy
Adding brachytherapy to Nd-YAG laser therapy improves the local control 65. Furthermore, the combination of laser therapy and brachytherapy in early lung cancer seems to offer a significant survival advantage over either therapy alone 66. This is also reported for the combination of HDR brachytherapy after 6 weeks with PDT 67. The combination with systemic chemotherapy is feasible and seems to provide radiosensitisation 68.
Conclusion
Bronchoscopic brachytherapy in its HDR form is an easy-to-perform outpatient treatment for endoluminal and paraluminal tumours. It is effective in palliating symptoms such as dyspnoea, haemoptysis, intractable cough, atelectasis and post-obstructive pneumonia. Brachytherapy can be combined with all other modalities of tumour therapy, e.g. external beam radiation, Nd-YAG laser therapy, PDT or chemotherapy and may improve the degree and duration of palliation. Small tumours can be cured by brachytherapy. Unfortunately, as with other endobronchial treatment modalities, experience is limited and further randomised studies are needed. Brachytherapy is a permanent interdisciplinary challenge with the need of a close contact between radiation oncologists and chest physicians. Further investigations are necessary to determine optimal dose fractionation and the ideal adjunctive use of the technique.
PHOTODYNAMIC THERAPY
Background
The healing power of sunlight and the therapeutic effects of light-activated chemical compounds have been recognised throughout history and by ancient civilisations 69. However, the scientific basis of light treatment (phototherapy) is rooted in the 20th century. In the early 20th century, Finsen 70, a Danish physician, noted that tuberculous lesions occurred more frequently during the winter season. This prompted him to study the effects of light in a number of conditions, notably smallpox and the cutaneous form of tuberculosis, lupus vulgaris, which at the time occurred commonly in Scandinavia. Finsen 70 harnessed light in the ultraviolet spectrum from sunlight and from electric arc lamps and thus laid down the foundation of phototherapy; in 1903 he was awarded the Nobel Prize in Physiology and Medicine for his work. There followed the establishment of departments of light therapy, known as Finsen Therapy, in many city hospitals throughout the world, most notably in Copenhagen (Denmark) where The Medical Light Institute was named after him.
Parallel with the development of Finsen's phototherapy, other scientists were focusing their attention on the biological effects of light-activated chemical compounds (photochemotherapy) on living tissue. In this area, Raab 71 and von Tappeiner and co-workers 72–74 were examining the effect of chemical compounds on infusoria. They made a number of observations, of which two were seminal in the development of PDT. They noted that the chemical compound acridine could affect the biological behaviour of paramecia and that the organism was killed when the preparation was exposed to daylight. They also discovered that air (oxygen) was necessary for the death of paramecia in the acridine plus light setting. These authors referred to the phenomenon as “Photodynamisch Wirkung” (photodynamic reaction/effect). During the 1960s and 1970s, experimental and clinical PDT evolved from these and subsequent observations, with the first recorded case of clinical PDT reported by Lipson et al. 75 in 1966. The case was a large recurrent ulcerating breast tumour treated by injection of haematoporphyrin derivative (HPD) followed by exposure to a filtered xenon arc lamp.
In the 1970s, a number of investigators were working on the photodynamic effects of different chemicals and their corresponding activating light. HPD and light in the red spectrum appeared as the most suitable combination to yield photodynamic action in the animal model and clinical situation 76, 77. Dougherty et al. 78 showed that systemic administration of HPD followed by exposure to red light from a xenon arc lamp could eradicate transplanted murine mammary tumour without much change to normal tissue surrounding the tumour. This same group started clinical trials in 1976 at Roswell Park Memorial Institute (Buffalo, NY, USA), which showed the effectiveness of PDT in a variety of malignant growths 76, 78, 79.
Bronchoscopic PDT began in 1982 at Tokyo Medical University (Tokyo, Japan), when Hayata et al. 80 treated a patient who had an operable early lung cancer but refused surgical intervention. The treatment was carried out with complete eradication of the tumour. After nearly 4 yrs the patient died from noncancer-related causes 81.
At that time, many of the PDT clinical trials were focused on cutaneous and subcutaneous cancer. Nevertheless, by virtue of its high incidence, advanced stage of disease at presentation and highly unresectable rate, lung cancer became one of the first cancers to be targeted for PDT trials 82–85.
This brief history demonstrates how clinical PDT evolved through phototherapy and photochemotherapy (table 1⇓).
Definition and mechanism of action of PDT in cancer
PDT is a treatment method which relies upon the excitation of a chemical photosensitiser (the drug) by an appropriate light whose wavelength matches the absorption band of the drug. Oxygen is essential in PDT, since the photodynamic reaction, leading to cell necrosis, depends on the release of singlet oxygen and the generation of other oxygen-dependent cytotoxic agents. The mechanism involved in cancer destruction and tumour necrosis in PDT has been the subject of continuing research for over 30 yrs. The observations by Von Tappeiner and colleagues 72–74 in the early 20th century were the initial basic steps that led to the description of photodynamic effect showing the destructive power of the photodynamic phenomenon. However, whilst the mechanism of death in a simple organism, such as infusozia, depends on direct cytotoxity of a light-activated chemical, in a complex multisystem species, as is the case for mammalians, such tissue destruction would be expected to rely on a number of additional factors. In the human species, the mechanism of PDT action, and cell death resulting from it, appears to be mediated through the following. 1) Generation of singlet oxygen and other toxic reactive oxygen species resulting from light and the photochemical interaction with oxygen. 2) Direct damage of subcellular and biomolecular structures of the cell. 3) Indirect ischaemic effects and injuries resulting from vascular shut down of affected tissue. 4) Indirect effects of the light-activated chemical and promotion of inflammatory and immune response. 5) Apoptosis.
It therefore appears that the mechanisms of photodynamic reaction are both direct, through disturbed cellular metabolism, and indirect, mediated by vascular and extracellular fluid, which constitutes the cell environment’s “milieu interior”.
Method
Bronchoscopic PDT for lung cancer is carried out as a two-stage procedure, namely, photosensitisation and illumination.
Photosensitisation stage
This stage is achieved by an intravenous administration of a suitable photosensitiser (the drug) to the patient. The first photosensitiser used for bronchoscopic PDT was derived from the porphyrin family. HPD was used systemically by intravenous injection at variable dose rates (2–4 mg·kg-1 body weight) 85. After manipulation and purification, HPD was commercialised for clinical use under the labels Photofrin® (Axcan Pharma Inc., Houdan, France) and Photosan® (Seehof Laboratorium Forschungs- und Entwicklungsgesellschaft mbH, Wesselburenerkoog, Germany), to name but a few. Photofrin® (Porfimer Sodium) is licensed for use in advanced-stage lung cancer by the Food and Drug Administration and European Union Licensing Authorities. At the present time, Photofrin® is the most commonly used photosensitiser for bronchoscopic PDT and has a long-standing safety record 69, 85–87. The recommended dose of Photofrin® is 2 mg·kg-1 body weight. At this dose, the drug is safe, reliable and nontoxic. However, it is not highly selective and indiscriminate illumination could result in collateral damage to normal adjacent areas with oedema and inflammation of the bronchial walls.
Chlorin family
Porphyrin-based photosensitisers were the first-generation sensitisers used for bronchoscopic PDT. Many other sensitisers have since been prepared and tested in the laboratory setting; although most have not reached clinical trial, a few have. Amongst the latter is meta-tetra(hydroxyphenyl)chlorin (Foscan®; Scotia Pharmaceuticals, Stirling, UK), which is not commonly used for bronchoscopic PDT. One group has employed Foscan® in a series of patients with apparent success and no major drawbacks 88. However, detailed information on its use for bronchoscopic PDT has not been published.
Illumination
Illumination consists of bronchoscopic exposure of the pre-sensitised tumour to a light of a specific matching wavelength. The overall effect is necrosis of the tumour. There are essentially two methods of illumination: interstitial and surface illumination. In the former, the light exposure is from within the tumour mass; in the latter, the exposure is over the surface of the tumour (fig. 13a⇓ and b).
Light sources
Photodynamic reaction is dependant on activation of the photosensitiser by a light of appropriate wavelength. The key to photodynamic reaction is the match between a specific wavelength of light and the absorption band of the chemical photosensitiser. The latter locks with the light and starts a chain reaction, which results in necrosis and cell death. The light which activates a porphyrin-based photosensitiser is within the red region of the spectrum (630 nm). A number of light sources have been used to deliver this red light to the tumour, including argon/dye lasers, metal vapour lasers and, more recently, diode lasers 89. For other photosensitisers, there are also diode lasers generating light of appropriate matching wavelength.
Light delivery system
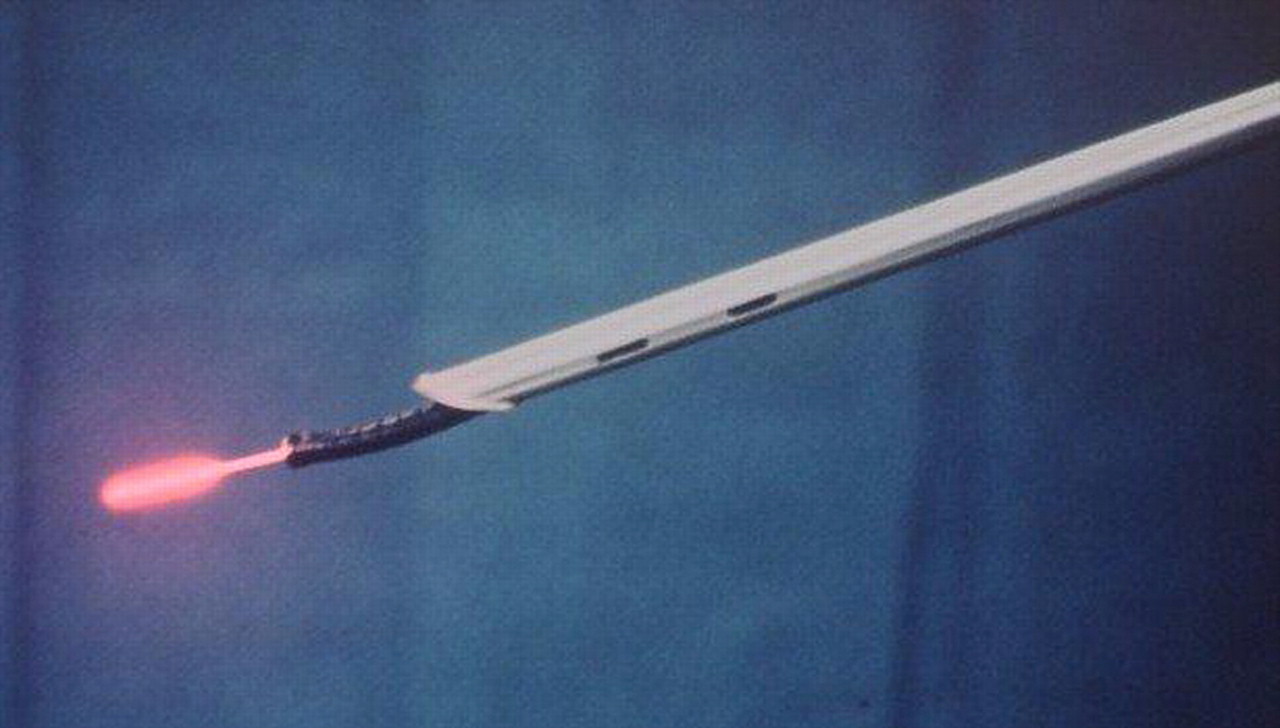
The light generated and emitted by a laser is delivered to the endobronchial tumour by optical fibres with either a cylindrical diffusing tip or a micro-lens. Cylindrical diffusers distribute light circumferentially and may be used for interstitial treatment when the diffuser is placed within the tumour mass. The micro-lens emits forward-firing light and is employed for surface application to treat superficial growth (fig. 14a⇓ and b). In either case, the delivery fibre is introduced via the biopsy channel of the fibreoptic bronchoscope, which provides access to the tumour (fig. 15⇓). The light dose at its point of delivery is calculated to be 200 J·cm-1 of lesion or the equivalent length of the delivery device 89. This is usually made up of 400 mW×500 s (1 J = power (mW)×time (s)).
Anaesthetic and instrumentation
The route of access for illumination of pre-sensitised endobronchial cancer is the biopsy channel of a flexible fibreoptic bronchoscope (FFB), which accommodates the light delivery optical fibre. Such bronchoscopic illumination can be achieved by one of the following two methods. Method 1 uses FFB under topical anaesthetic and sedation with the patient breathing normally. This is similar to diagnostic bronchoscopy as practiced by bronchoscopists. Method 2 uses general anaesthesia and controlled positive pressure ventilation by a jet ventilator or by hand-controlled injector. In this method, the open-ended rigid bronchoscope is first placed in the trachea for ventilation. The FFB is then introduced through the bronchscope for precise visualisation of the lesion and illumination (fig. 15⇓).
Each method has advantages and disadvantages (table 2⇓). The use of general anaesthetic necessitates the presence of an anaesthetist and more elaborate equipment, but provides a comfortable environment for the patient and facilitates the operative procedure. General anaesthesia and use of the rigid instrument allows the operator more time, better access to lesions and less risk of displacement of the delivery fibre in patients with bulky tumours and/or multiple lesions. However, a unifocal superficial lesion of limited extent can easily be treated using FFB under topical anaesthesia. In the present author’s experience, the use of the combined rigid and flexible instruments under general anaesthesia is best for patients with obstructive exophytic tumour of the major airway (trachea main stem bronchi), and should be recommended for such cases. For other cases the choice depends on the experience of the operator and patient choice.
Review of the literature concerned with bronchoscopic PDT 85 seems to indicate the following. 1) Many authors whose series consist predominantly of patients with advanced stage disease and endoluminal obstruction of major airways have employed general anaesthetic and its associated instrumentation. 2) Authors treating early superficial lesions have used topical anaesthetic and FFB.
Bronchoscopic PDT in practice
Patients selected for bronchoscopic PDT will have had standard lung cancer work up, including diagnostic bronchoscopy and confirmation by histo/cytology of the malignant tumour. Prior to photosensitisation, a further bronchoscopic examination is carried out using white light and fluorescence bronchoscopy (if available) in order to delineate the tumour and its extent (fig. 16a⇓ and b). It is important that the bronchial tree is examined in its entirety in order to map out synchronous lesions in adjacent or more distant sites from the main focus. After administration of the photosensitising drug, time is allowed for its absorption and its preferential retention in the tumour. The duration of this latent period depends, to a large extent, on the composition of the photosensitiser. For Photofrin®, this is 24–72 h. Following this period, bronchoscopic illumination is carried out. This consists of exposure of the pre-sensitised tumour (or all tumour sites) to laser light, as previously described.
Post-PDT management
Clearance of the airways, debridement
Immediately after illumination, attention should be paid to clearance of the airways and removal of debris (fig. 17⇓) from the treated area and beyond with the use of biopsy forceps, followed by aspiration and lavage with normal saline solution. In patients with exophytic endoluminal obstructive tumours requiring interstitial treatment, it is necessary to carry out this procedure not only immediately after illumination, but also a few days later. At this time, some necrosis of the tumour occurs, as well as discharge of infected secretions collected beyond the bronchial obstruction. Clearance of the airways in patients with bulky obstructive tumours is most effectively carried out with the use of the rigid bronchoscope and its accessories.
Re-illumination
It is important to consider re-illumination after post-PDT debridement when it is deemed necessary, i.e. when there are residual tumour islands. It should be emphasised that such illumination needs to be within the prescribed time (within 6–7 days of the intravenous injection of Photofrin®) so that tumour tissue concentration of the photosensitiser (drug) is either at therapeutic level.
Prevention of bronchopulmonary infection
This is particularly relevant to patients with significant lobar or segmental tumour obstruction. In such patients, post-PDT necrosis creates a good culture medium for organisms in the airway, notably beyond the obstructive lesion. Physiotherapy, breathing exercise and, at times, a course of antibiotics may be required.
Indications and patient selection for bronchoscopic PDT
It is generally agreed that surgical resection is the treatment of choice for lung cancer when the tumour is oncologically and technically resectable, and provided that the patient is fit for and consents to the operation. Considering this, it is also acknowledged that only a small proportion of patients, amounting to ≤15–20% of the lung cancer population, could qualify for resectional surgery. It therefore follows that 80–85% of lung cancer patients are classified as inoperable, either by the nature of their advanced stage disease, because of poor general condition or from choice. This is a huge population, amounting to >25,000 individuals per annum in the UK alone. In 50–60% of this population, the tumour is central, projecting into the bronchial lumen, is visible bronchoscopically and is diagnosable by bronchial biopsy. For the purposes of interventional bronchoscopy (including bronchoscopic PDT), the present author classifies these tumours as type I lung cancer, as opposed to type II cancer, which are peripheral tumours not directly diagnosable bronchoscopically.
The prerequisite for bronchoscopic PDT is the presence of a malignant endobronchial lesion confirmed by cytohistology. By implication, only patients with central (type I) lung cancer will qualify for PDT. Theoretically PDT is indicated in every patient with type I lung cancer if their general condition allows bronchoscopic operation. In practice, at the present time, selection for bronchoscopic PDT is made from subjects unsuitable for surgery (inoperable/unresectable patients) according to the extent and stage of their disease. These inoperable patients are divided into two groups. 1) Those with advanced stage disease (stages III and IV) 90 at presentation (group/subtype A). These patients are inoperable because they are oncologically unresectable. 2) Those with early stage disease (group/subtype E) with oncologically and technically resectable cancer but who are, for a variety of reasons, unsuitable for surgical resection.
PDT is indicated in both groups but with different objectives. For group A patients, the aim is palliation of symptoms, whereas for group E patients, the aim is survival benefit and curative intent.
Group A patients
The majority of patients in group A have an obstructive endobronchial lesion and are usually symptomatic with dyspnoea, cough and haemoptysis; the relief of obstruction will alleviate the symptoms (fig. 18⇓). The initial trial of bronchoscopic PDT in the 1980s was directed towards symptomatic patients with endoluminal exophytic tumours causing major obstruction 83. In the light of subsequent and more recent experience, PDT indications in this group have become more stringent. The present selection criteria consist of the following: 1) patients with inoperable/unresectable tumour with existing or impending related symptoms; 2) patients with good performance status (Karnofsky performance status index >50% or World Health Organization (WHO) scale ≤ 3); and 3) patients without extrathoracic metastatic disease.
Previous surgical operation, chemo-/radiotherapy or other endoluminal therapy do not constitute exclusion criteria. All histological types respond to PDT, including small cell cancer, provided that the lesion can be accessed bronchoscopically for illumination.
Group E patients
In the context of bronchoscopic PDT, the term early cancer is used to describe cases in which the tumour is limited in its extent to the bronchial tree and is confined in depth to the inner bronchial wall. It is important to emphasise that standard investigatory methods may not be capable of providing a precise diagnosis of early stage cancer according to the above definition. A carcinoma in situ involving superficial layers of bronchial epithelia can be radiologically occult and bronchoscopically invisible when examined using white light. It is also relevant to emphasise that a case with superficial synchronous (multifocal) endobronchial lesions should, for the purpose of bronchoscopic PDT, be considered as an early cancer even though, based on standard tumour node metastasis classification 90, it cannot be classed as stage I.
Two recently developed methods assist the bronchoscopic diagnosis of early cancer. Fluorescence bronchoscopy uses a blue light with greater discriminative power of differential fluorescence imaging than its white light counterpart. This more accurately displays mucosal abnormalities than white light bronchoscopy 91, 92 and is of use both for pre-PDT diagnosis of early endobronchial cancer and for monitoring response to treatment. The second development is endobronchial ultrasonography. This enables the imaging and estimation of the depth of bronchial wall involvement by the tumour 93–95.
At the time of writing, there is some consensus of opinion in respect of bronchoscopic PDT indications in early stage lung cancer. These are patients: 1) whose general condition puts them in such a high-risk category as to prohibit them being offered resectional surgery; 2) who have inadequate predicted post-operative (post-resection) pulmonary function (such patients may well recover from the operation but post-operatively they may become a respiratory cripple with unacceptably poor quality of life); 3) who have multifocal endobronchial early cancer whose surgical resection is either technically impossible or would entail too extensive a loss of pulmonary parenchyma; 4) who present with early stage metachronous cancer following previous extensive surgical resection; and 5) who decline surgical resection but consent to PDT.
Some patients with early lung cancer present with cough, blood-stained sputum and dyspnoea. The latter is not usually related to endobronchial tumours, but is associated with co-existing conditions such as chronic obstructive pulmonary disease.
Results/outcome
Bronchoscopic PDT results are evaluated using the following parameters: 1) mortality and morbidity; 2) local pathological response to treatment; and 3) patient satisfaction and clinical effect.
Mortality and morbidity
Over the years, experience has shown that bronchoscopic PDT is a safe treatment method. Technically the procedure can be mastered by the majority of bronchoscopists. There is no death associated with the procedure per se and the 30-day mortality rate (empirically set for surgical operations) is <1% (table 3⇓). A recent review article 85 concerning 25 publications from the world literature and comprising 1,153 patients undergoing nearly 2,000 bronchoscopic PDT procedures for cancer confirms this.
Important adverse reactions of bronchoscopic PDT are presented in table 3⇓. The morbidity of bronchoscopic PDT relates greatly to skin burn, i.e. photosensitive reaction of the skin exposed to sunlight. This was reported to be 20% for bronchoscopic PDT with Photofrin® in a multicentre trial. Skin burn can be an important drawback and a prohibitive factor for clinical PDT, particularly in those cancer patients with limited life expectancy. Nevertheless, it should be emphasised that this is an avoidable complication whose incidence can be reduced considerably by thorough counselling and regular reminders to the patient to avoid exposure to sunlight. At the Yorkshire Laser Centre (YLC; Goole, UK), with a total of nearly 500 PDTs using a systemically administered photosensitiser, the incidence of skin burn in different series has consistently been 3.5–5.3% of patients. Furthermore, in the last 50 patients, no cases of skin burn have been recorded.
Other complications of bronchoscopic PDT reported in the literature are listed in table 3⇓.
Local pathological response to treatment
By convention, local response to treatment is described as complete response/remission (CR) when a treated area becomes macroscopically and microscopically (by cyto/histology) clear from tumour. Partial response/remission (PR) occurs when macroscopic extent of the tumour is reduced by ≥50% after treatment, but cyto/histology demonstrates presence of malignancy. No response occurs when there is little (<50%) or no change in the macroscopic extent of the tumour and the histology remains unaffected.
It is important to note that CR and PR are not precise measurements but are nevertheless a useful concept both in terms of monitoring of treatment and also in relation to decision-making for further management of the patient. It is also necessary to point out that response to treatment, be it CR or PR, becomes meaningful when it is further quantified by duration of response and related symptomatic relief.
Patient satisfaction
The level of patient satisfaction reflects the overall quality of care as well as subjective evaluation of the treatment; it is therefore important that these should be recorded.
Clinical effects and survival
Patients with advanced stage disease
In patients with advanced disease and significant endoluminal bronchial obstruction, PDT is capable of relieving the obstruction and the related symptoms. Parallel with relief of obstruction, there is an improvement in pulmonary function and radiological clearance 87 (fig. 18⇓). Pathologically, there is a PR in all and CR in some, irrespective of the histology 85–87. Generally, survival is related to the stage of the disease. In addition, two subsets of patients have been shown to have survival benefit. First, those with a good performance status (<2 WHO scale or >50 Karnofsky index) and, secondly, patients without extrathoracic metastases 87, 96; histology per se does not appear to influence survival. Whilst an overall majority of cases referred for and submitted to bronchoscopic PDT have NSCLC, patients with small cell cancer also benefit from the procedure provided that there is endoluminal tumour and the aforementioned criteria are fulfilled. In some such cases, bronchoscopic PDT has been carried out concomitant to chemotherapy 81, 87, 95 or following chemo-/radiotherapy. In fact, many patients with advanced stage type I NSCLC are referred for PDT due to recurrence of tumour after chemo-/radiotherapy. In one series of 100 patients with advanced, inoperable cancer 87, 85% had chemo-/radiotherapy prior to referral for PDT. It is interesting that in some cases amongst these, the endobronchial component of the tumour was found to have been nonresponsive to chemo-/radiotherapy and endoluminal volume remained unaltered at post-therapy bronchoscopic examination. These observations show that resistance or lack of response to chemo-/radiotherapy does not imply lack of response to PDT. They also suggest that there is no incompatibility between PDT and chemo-/radiotherapy.
Patients with early stage cancer
Many patients with early lung cancer are asymptomatic and assessment of results in this subgroup is based on pathological response and survival. In general, CR is achieved in all patients, albeit for a variable length of time. It should be noted that monitoring response to treatment in early stage bronchial cancer may prove difficult without the added assistance of fluorescence bronchoscopy. This is because localisation of the treated area for sampling may prove impossible with the use of white light bronchoscopy alone. Also, without fluorescence endoscopy, newly developed early cancer could either escape detection or be assumed to be at the previously treated area. Bronchoscopic PDT can achieve long survival amounting to cure of disease in patients, with early superficial lung cancer confined to the bronchial wall. The Tokyo Medical University has the largest experience of bronchoscopic PDT in early lung cancer and has shown a nearly 60% overall 5-yr survival and >90% cancer-specific survival in such patients 81, 97. The present author’s group at the YLC, with a smaller series, has also shown comparable results 96. A review of 12 articles from world literature involving 650 patients undergoing bronchoscopic PDT for early cancer 85 shows that long survival of >5 yrs is achieved in >50% of cases. The inconsistency of long-term response is, according to the author’s belief, related to difficulty in defining the “earliness” of the tumour.
Conclusions
There is sufficient evidence to state that bronchoscopic PDT is a safe and effective method of therapy for central type (type I) lung cancer using sensitisers that are currently tried and licensed; Photofrin® (Porfimer Sodium) is the commonest in use. Photosensitivity skin reaction (skin burn) should not be a prohibitive factor; its incidence and severity can be reduced to a minimal proportion with effective counselling.
The pre-requisite for bronchoscopic PDT is identifiable cancer in the bronchial tree and confirmation of its malignancy by cyto/histology.
Bronchoscopic PDT is indicated in two groups of patients with central type (type I) cancer. 1) Patients with advanced disease or with existing and/or impending symptoms. The aim in this group is palliation of symptoms and PDT is shown to achieve this goal. Patients with no extrathoracic metastases and those with good performance status will have survival benefit. Such cases should be offered other bronchoscopic treatment such as Nd-YAG laser. 2) Patients with early stage cancer. In these, the aim is curative intent and PDT is shown to provide long survival and is potentially capable of disease cure.
Final conclusion
As underlined in this article, cryotherapy, brachytherapy and photodynamic therapy represent three different techniques to treat endoluminal tumours. None of them are perfect and each has specific indications. Unfortunately, no comparative studies have been published. Tables 4⇓ and 5⇓ attempt to summarise the indications and results of each method compared with others. In many situations, these methods should be complementary, particularly cryotherapy and brachytherapy, and photodynamic therapy and brachytherapy. The combination of these endoscopic methods with chemotherapy should be widely tested to promote the adjuvant role of the endoscopic methods in the treatment of lung cancers.
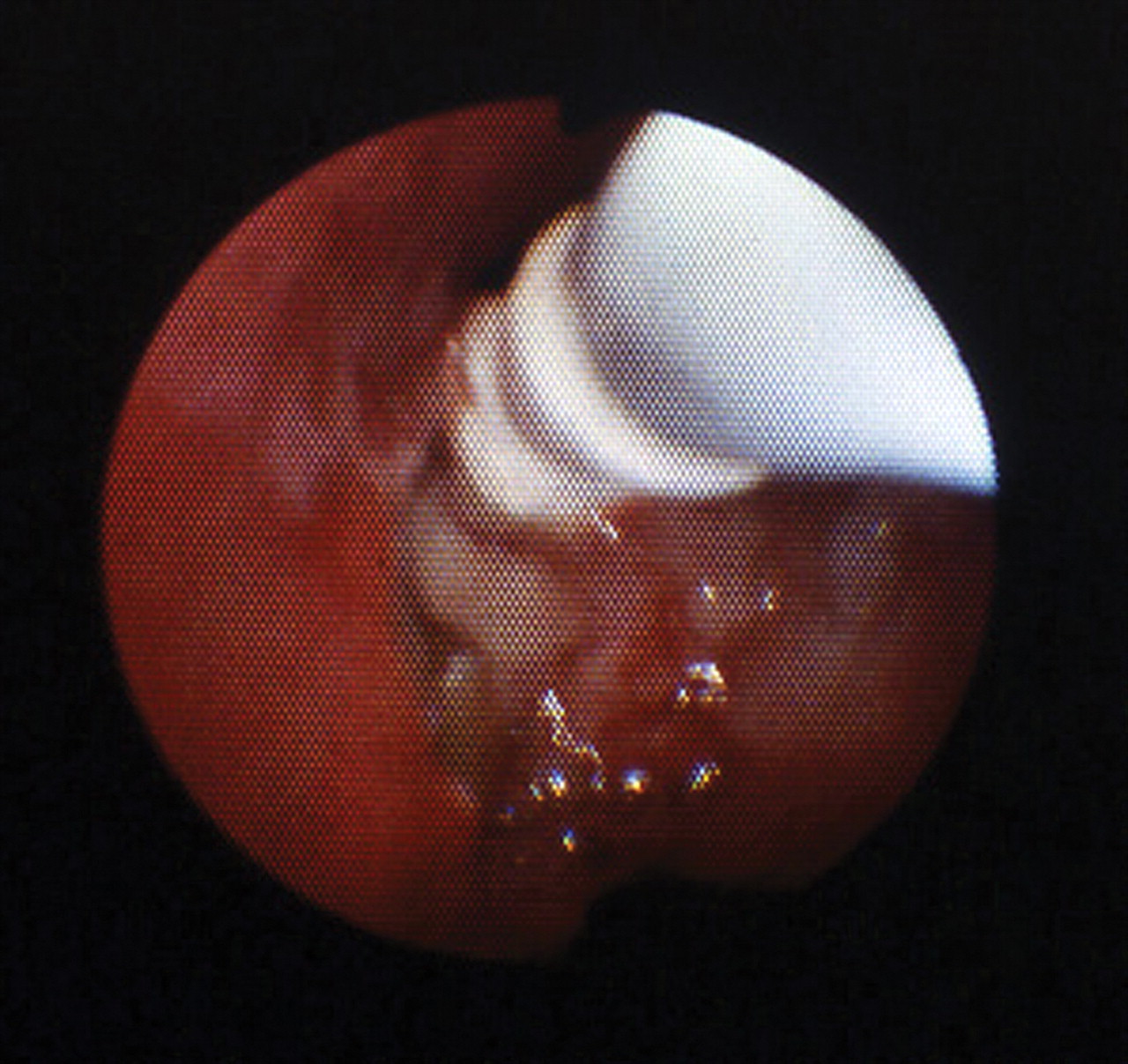
Flexible cryoprobe used to treat a tumoral obstruction in the right upper lobe.
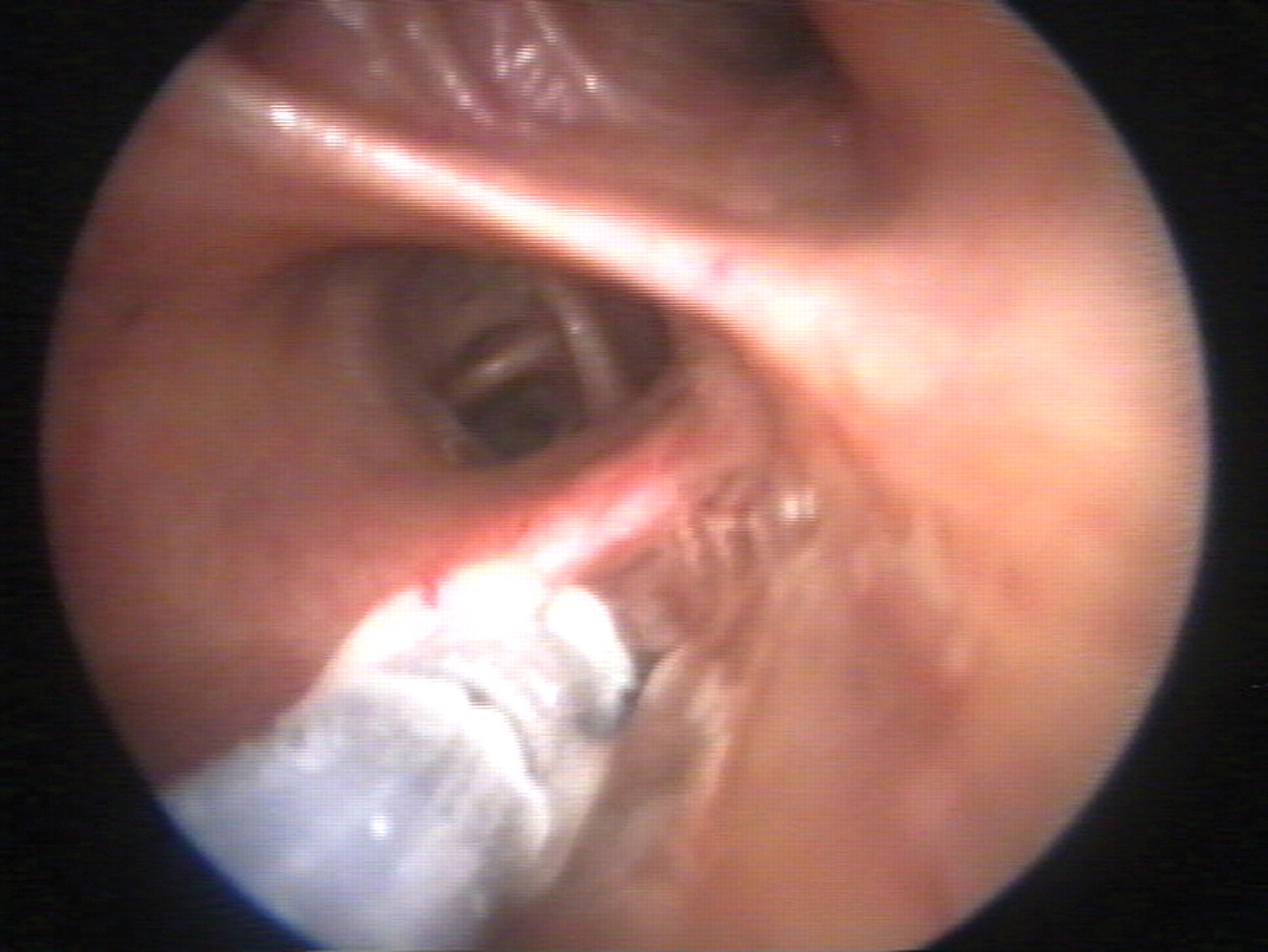
Rigid-probe cryotherapy of an early stage lung cancer located on a right lower lobe carena.
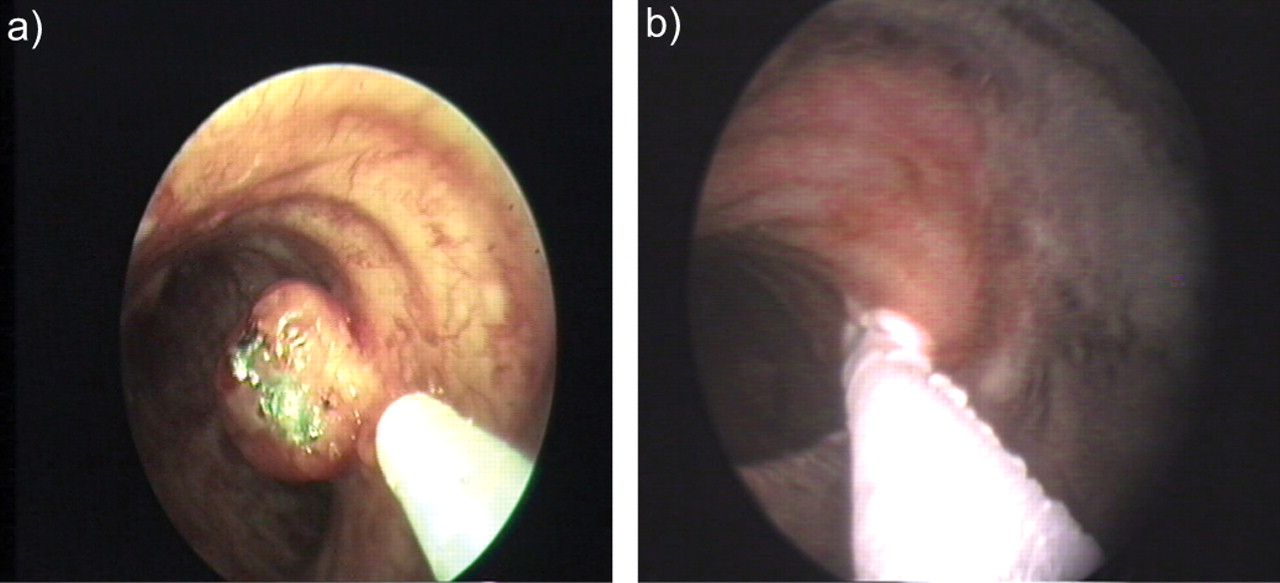
Metastatic renal tumour in the trachea treated with a) laser-assisted resection and then b) cryotherapy, applied on the residual stalk.

Typical carcinoid of the right upper lobe treated with cryotherapy alone: aspect a) before and b) 2 weeks after the treatment, showing a perfect result with no stricture. (Supplied courtesy of R. Jean-François, Montreal University Hospital, Montreal, Canada.)

Removal of a clot located in the left main stem bronchus with a rigid cryoprobe.

Two human lung adenocarcinoma were xenografted on the back of the SKID mouse as shown. The initial size of the two tumours was similar. The aspect of the tumours shown is 2 weeks after a treatment with i.v. vinorelbine (Navelbine®; Pierre Fabre Laboratories, Gaillac, France). Only the left tumour was treated before chemotherapy with three cycles of cryotherapy.

Cryotherapy followed by irradiation of human small cell lung cancer xenografted on the back of a “nude” mouse. The mouse at the top underwent irradiation alone. The mouse at the bottom underwent cryotherapy followed by irradiation.

The principle of isodoses in high dose-rate brachytherapy. Orange: 5 Gy; green: 10 Gy. #: 7 cm.

Placement of the afterloading catheter in the left upper lobe of the lung.

Treatment planning with isodose distribution (values are in Gy).
Tumour a) before first brachytherapy session and b) 3 weeks later (before the second session).

a) Radiation bronchitis and b) stenosis.
Tumour mass in the right upper lobe a) with cylindrical diffuser in the tumour and b) with illumination in progress.

a) Bronchoscopic view of an early cancer and b) with surface illumination.

Bronchoscopic photodynamic therapy with the use of a combined rigid and flexible bronchoscope. Note the optical fibre with its end diffuser protruding through the biopsy channel of the fibreoptic bronchoscope for illumination.
a) White light bronchoscopic view of a case of left upper lobe carcinoid. b) Fluorescence bronchoscopic view using Xillix LIFE-Lung Fluorescence Endoscopy System (Xillix Technologies Corp., Richmond, BC, Canada) of the same case showing more extensive mucosal alteration.

a) Bronchoscopic view showing tumour almost completely obstructing the right main bronchus. b) Clearance of the bronchus 1 month after bronchoscopic photodynamic therapy. c) Tumour debris mixed with a fibrin clot removed 1 week after bronchoscopic photodynamic therapy.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
a) White light bronchoscopic view of an obstructive tumour in the right main bronchus. b) Pre-treatment chest radiograph of the same patient showing complete collapse (atelectasis) of the right lung. c) White light bronchoscopic view 1 week after treatment. d) Post-treatment chest radiograph.
Evolution of photodynamic therapy and definition of treatments involving light
Comparison of the two methods of illumination for bronchoscopic photodynamic therapy(see text for details)
Mortality and morbidity of bronchoscopic photodynamic therapy(PDT)
Therapeutic endoscopy indications in lung cancers
Results in lung cancers
Acknowledgments
The authors would like to thank G. Collier (Cardiff, UK) for help with the English language. K Moghissi would like to thank K. Dixon for her editorial work on the manuscript and E. Binnington and J. Melvin for secretarial work.
Footnotes
-
Previous articles in this series: No. 1: Bolliger CT, Sutedja TG, Strausz J and Freitag L. Therapeutic bronchoscopy with immediate effect: laser, electrocautery, argon plasma coagulation and stents. Eur Respir J 2006; 27: 1258–1271.
- Received January 30, 2006.
- Accepted March 29, 2006.
- © ERS Journals Ltd
References










