





Abstract
In patients with pulmonary hypertension associated with interstitial lung disease, pulmonary vascular resistance provides stronger prognostic information than mean pulmonary arterial pressure https://bit.ly/3w1QcIS
To the Editor:
Pulmonary hypertension (PH) is a common complication of many chronic lung diseases, especially COPD and interstitial lung disease (ILD) [1]. In these conditions, the development of PH is associated with an aggravation of symptoms and an increase in mortality risk. In most patients with chronic lung disease, the haemodynamic severity of PH is mild to moderate, while some patients develop severe PH, which is presently defined by a mean pulmonary arterial pressure (mPAP) ≥35 mmHg or mPAP ≥25 mmHg in the presence of a cardiac index <2.0 L·min−1·m−2 [2]. These haemodynamic criteria were introduced per expert consensus but were not based on solid data.
In patients with PH associated with COPD, Zeder et al. [3] showed recently that a pulmonary vascular resistance (PVR) >5 WU was the strongest haemodynamic predictor of mortality, and the authors suggested to use this threshold to define severe PH in this group of patients. We wondered whether this threshold might also apply to patients suffering from PH associated with ILD (PH-ILD).
To address this question, we analysed data from the Comparative, Prospective Registry of Newly Initiated Therapies for Pulmonary Hypertension (COMPERA). Details of COMPERA (www.COMPERA.org; Clinicaltrials.gov identifier NCT01347216) have been reported previously [4]. In brief, COMPERA is a large-scale ongoing web-based PH registry that prospectively collects detailed data on characteristics, treatment and outcomes of patients who receive therapies for PH. PH centres from various European countries participate (Austria, Belgium, Germany, Greece, Hungary, Italy, Latvia, Lithuania, Netherlands, Slovakia, Switzerland and UK), with about 80% of the enrolled patients coming from Germany. COMPERA has been approved by the ethics committees of all participating centres, the data are pseudonymised, and all patients provide written informed consent prior to inclusion.
For the present analysis, patients were selected from the COMPERA database by the following criteria: 1) adult patients newly diagnosed with PH-ILD between13 June, 2006, and 21 January, 2021; 2) haemodynamics available at inclusion with mPAP ≥25 mmHg and pulmonary artery wedge pressure (PAWP) ≤15 mmHg; and 3) at least one documented follow-up visit. Continuous data were presented as median and first and third quartile (Q1, Q3), categorical data as number and percentage. Follow-up ended on 30 April, 2021. Group comparisons were done by Wilcoxon rank sum test for continuous variables and by Chi-squared test for binary variables. Survival was evaluated using Kaplan–Meier curves, log-rank tests and multivariable Cox regression models with results shown as hazard ratio (HR) and 95% confidence intervals. All statistical analyses were performed using R version 4.0.0.
At cut-off day (1 May, 2021), 10 651 patients were registered in the COMPERA database, of which 662 patients were classified as PH-ILD. Of these, 213 patients were excluded for the following reasons (more than one may apply): PH diagnosis >6 months prior to the baseline visit (n=73), age <18 years (n=2), lung transplantation at any time (n=29), no documented follow-up visit (n=55), failure to meet the haemodynamic inclusion criteria (no baseline PVR value, n=50; PAWP >15 mmHg or mPAP <25 mmHg, n=61). Finally, 449 patients were eligible for the present analysis.
The median (Q1, Q3) age of the included patients was 73 (67, 78) years; 65% were male. Usual interstitial pneumonia was the most common underlying disease (40%), followed by combined pulmonary fibrosis and emphysema (27%), non-specific interstitial pneumonia (15%) and others (18%). Pulmonary function tests at inclusion showed a total lung capacity (TLC) of 72 (60, 86) % predicted, a forced vital capacity (FVC) of 67 (53, 84) % predicted, a forced expiratory volume in 1 s (FEV1) of 69 (55, 81) % predicted and a diffusion capacity of carbon monoxide (DLCO) of 26 (20, 34) % predicted. Haemodynamics at baseline were as follows: mPAP 39 (33, 46) mmHg, PAWP 8.0 (6.0, 11.0) mmHg, cardiac index 2.1 (1.7, 2.6) L·min−1·m−2, and PVR 7.6 (6.0, 10.6) WU.
A total of 321 (71.5%) patients died during follow-up; the estimated median survival time from inclusion was 1.8 (95% CI 1.6–2.0) years. Independent predictors of death by multivariable Cox regression analyses (based on 367 patients for whom all variables were available) were higher age (HR 1.02, 95% CI 1.01–1.04; p=0.004), male sex (HR 1.38, 95% CI 1.05–1.81; p=0.022), lower TLC (HR 0.99, 95% CI 0.98–1.00; p=0.012) and higher PVR (HR 1.09, 95% CI 1.02–1.17; p=0.014). Other haemodynamic variables, including mPAP, cardiac index and PAWP did not predict survival (HR 0.99, 95% CI 0.97–1.02; p=0.511; HR 1.08, 95% CI 0.79–1.48; p=0.614; and HR 1.02, 95% CI 0.98–1.06; p=0.419, respectively). Similarly, FVC and FEV1 (HR 1.00, 95% CI 0.99–1.01; p=0.964; and HR 1.00, 95% CI 0.99–1.01; p=0.658, respectively) were not predictors in the model.
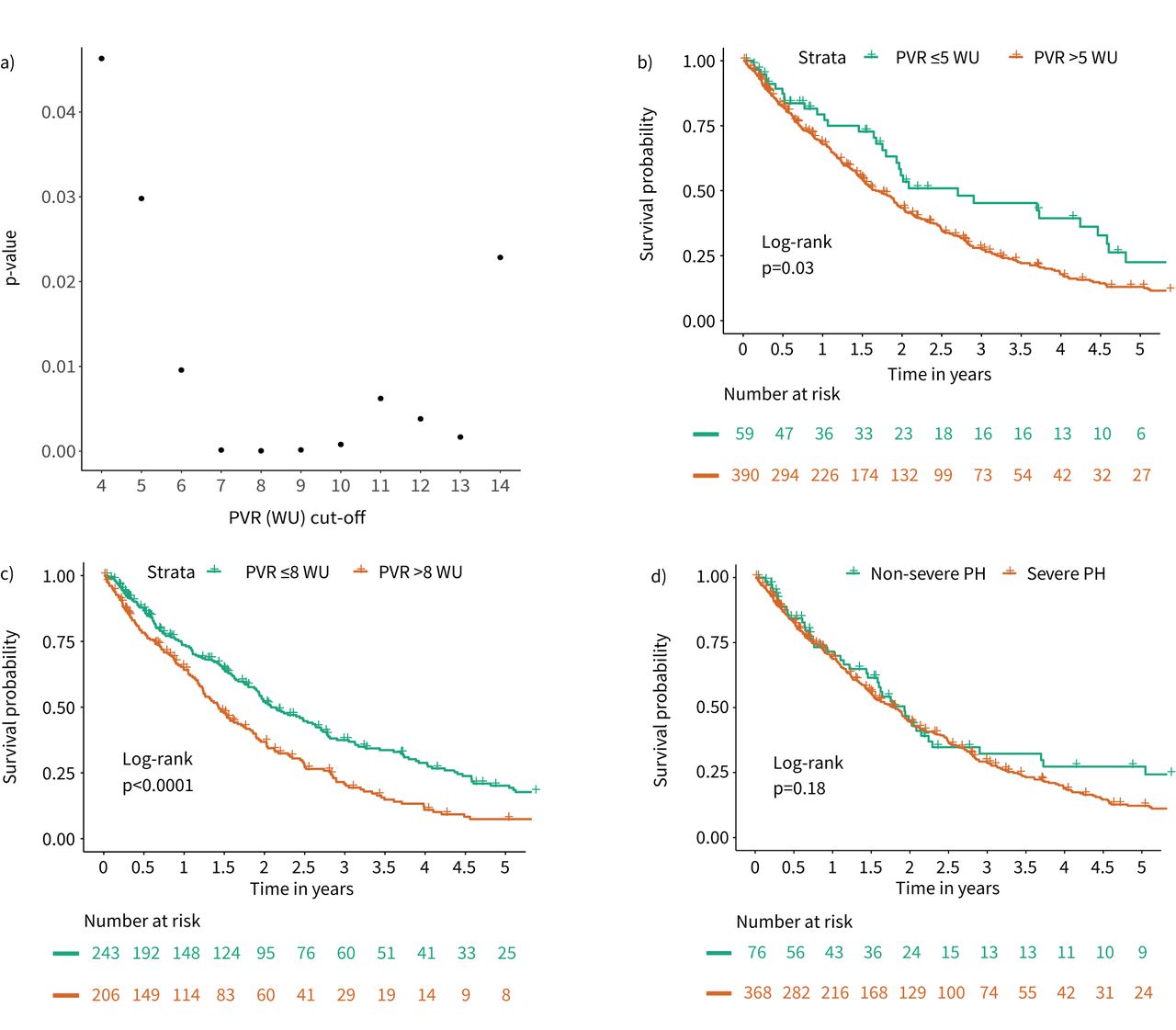
When looking at various PVR cut-off levels, PVR >5 WU was associated with a significantly worse survival compared to PVR ≤5 WU (figure 1a). The corresponding Kaplan–Meier analysis visualises the survival difference (p=0.03; figure 1b). Patients with PVR ≤5 WU and >5 WU did not differ in age, sex, BMI, TLC, FVC and FEV1 at baseline (p>0.05 for all group comparisons; data not shown). However, patients with PVR >5 WU had lower 6-min walk distance (222 (144, 300) m versus 295 (222, 351) m) and lower DLCO (25 (20, 33) % predicted versus 34 (21, 39) % predicted) at inclusion.

{kind=link}
Prognostic value of pulmonary haemodynamics in patients with pulmonary hypertension (PH) associated with interstitial lung disease. a) Scatterplot of different pulmonary vascular resistance (PVR) cut-off levels and the corresponding p-values of the log-rank test. b) Kaplan–Meier survival curve stratified by PVR ≤5 WU and PVR >5 WU. c) Kaplan–Meier survival curve stratified by PVR ≤8 WU and PVR >8 WU. d) Kaplan–Meier survival curve stratified by the current haemodynamic definition of severe PH in current lung disease (mean pulmonary arterial pressure (mPAP) ≥35 mmHg or mPAP ≥25 mmHg with cardiac index <2.0 L·min−1·m−2).
A PVR cut-off level of 8 WU had the lowest p-value (figure 1a) and provided the best discrimination in survival (figure 1c). In contrast, the currently proposed haemodynamic definition of severe PH in chronic lung disease failed to distinguish between survivors and non-survivors (figure 1d).
We acknowledge the limitations of the present study, including retrospective design, incomplete follow-up data, limited patient numbers, especially in the non-severe PH group, and potential selection bias, given that COMPERA enrols only patients who receive treatment with drugs approved for pulmonary arterial hypertension.
Despite these limitations, our data corroborates and extends previous observations by Zeder et al. [3] and Vizza et al. [5], both showing that in patients with PH-COPD, PVR provides stronger prognostic information than mPAP or other haemodynamic variables. In Zeder et al. [3]'s analysis of patients with PH-COPD, PVR >5 WU was the best prognostic cut-off value, while in our analysis of patients with PVR-ILD, the best discrimination between survivors and non-survivors was seen at PVR >8 WU. However, our analysis also showed that mortality increased significantly with PVR >5 WU. At the same time, the current mPAP-based definition of severe PH in chronic lung disease was not found to be prognostic in the present analysis. Based on these findings, while bearing in mind the limitations of this and previous analyses, we believe that PVR >5 WU should be used to define the presence of severe PH in patients with chronic lung disease.
Shareable PDF
Supplementary Material
This one-page PDF can be shared freely online.
Shareable PDF ERJ-01483-2021.Shareable
Acknowledgements
The authors are indebted to the COMPERA investigators and their co-workers.
Footnotes
This article has an editorial commentary: https://doi.org/10.1183/13993003.02008-2021
Conflict of interest: K.M. Olsson has received fees for lectures and/or consultations from Actelion, Bayer, Janssen, MSD, United Therapeutics, GSK and Pfizer.
Conflict of interest: M.M. Hoeper has received fees for lectures and/or consultations from Acceleron, Actelion, Bayer, GSK, Janssen, MSD and Pfizer.
Conflict of interest: C. Pausch has no disclosures.
Conflict of interest: E. Grünig received fees for lectures and/or consultations from Actelion, Bayer, GSK, Janssen, MSD, United Therapeutics and Pfizer.
Conflict of interest: D. Huscher has received fees for lectures and consultations from Actelion.
Conflict of interest: D. Pittrow has received fees for consultations from Actelion, Biogen, Amgen, Aspen, Bayer, Boehringer Ingelheim, Daiichi Sankyo, Viatris, Takeda and Sanofi.
Conflict of interest: S. Rosenkranz has received fees for lectures and/or consultations from Abbott, Acceleron, Actelion, Bayer, BMS, Gilead, GSK, Janssen, Pfizer, MSD, Novartis, United Therapeutics and Vifor.
Conflict of interest: H. Gall reports personal fees for lectures and/or consultations from Actelion, AstraZeneca, Bayer, BMS, Gilead, GSK, Janssen-Cilag, Lilly, MSD, Novartis, OMT, Pfizer, and United Therapeutics.
Support statement: This work was supported by the German Centre of Lung Research (DZL). COMPERA is funded by unrestricted grants from Acceleron, Bayer, GSK, Janssen and OMT. These companies were not involved in data analysis or the writing of this manuscript. Funding information for this article has been deposited with the Crossref Funder Registry.
- Received May 25, 2021.
- Accepted June 17, 2021.
- Copyright ©The authors 2021. For reproduction rights and permissions contact permissions{at}ersnet.org










