





Abstract
The microbiome is heterogeneous at COPD exacerbation, but different microbiota profiles are associated with both the clinical presentation and severity https://bit.ly/2X1sTzd
To the Editor:
COPD exacerbations are associated with worsening symptoms including cough, shortness of breath, sputum production and airflow obstruction. Increased numbers of exacerbations are associated with morbidity and mortality [1]. Exacerbations are classically believed to be associated with viral or bacterial infection, although they may also be associated with noninfectious stimuli including eosinophilic inflammation or paucigranulocytic exacerbation such as the worsening of cardiovascular disease [2]. The mainstay treatment for exacerbation of COPD is antibiotics and corticosteroids; however, treatment with these is not always successful and there is a need for more personalised management of exacerbations [3]. One of the largest studies of the sputum microbiome in COPD compared the microbiome at stability and exacerbation in 161 exacerbations in 78 patients and found no consistent changes in the microbiome with no overall difference in Shannon diversity index between the groups [4]. The most striking finding of this study was that COPD exacerbations could be classified into bacterial, viral and eosinophilic and patients showed remarkable consistency of their exacerbation phenotype over time. A number of studies have supported these defined phenotypes of exacerbation in COPD [2]. Therefore, in this study we aimed to examine whether we could observe changes in the microbiome from stability to COPD exacerbation within these three subtypes of clinically defined events.
Patients were invited to participate in the study and were included if they were aged >40 years, had a forced expiratory volume in 1 s (FEV1)/forced vital capacity ratio <70% at screening, and a clinical diagnosis of COPD. Exclusion criteria included the inability to give informed consent; primary diagnosis of asthma; and systemic immunosuppression (excluding prednisolone ≤5 mg daily). Patients were required to be clinically stable and 4 weeks free from antibiotic or corticosteroid treatment at baseline for enrolment. Patients provided an induced sputum sample at baseline and attended for a further induced sputum sample at exacerbation if one occurred within 6 months. Details of this cohort have been reported previously [5]. Exacerbations were classified as bacterial (positive sputum culture), eosinophilic or viral/paucigranulocytic, as previously described [2, 4]. Bacterial/viral co-infections were analysed as bacterial for the purposes of this analysis. DNA was extracted from sputum followed by 16S rRNA gene sequencing on the Illumina MiSeq platform (San Diego, CA, USA). Bioinformatic analysis and quality checking of the resulting sequences was performed using QIIME (version 1.9.0; http://qiime.org/). Appropriate negative (water) extraction and sequencing controls were included. Shannon–Wiener diversity index was used as a measure of α-diversity within samples. β-diversity was analysed using principal coordinates analysis and groups were compared using permutational multivariate ANOVA (PERMANOVA) based on the Bray–Curtis similarity index. Differences between two groups were further evaluated using linear discriminant analysis effect size (LEfSe) with false discovery rate (FDR) adjustment for multiple testing. Paired tests were used when comparing paired stable and exacerbation samples, while exacerbation subgroups were analysed as independent groups. Detailed methods have been described previously [5] and all sequences generated are available in the National Center for Biotechnology Information Sequence Read Archive under the BioProject accession numbers PRJNA539959 and PRJNA316126.
We studied 46 participants who experienced a total of 73 exacerbations. Mean±sd age was 70.8±7.0 years; 27 (58.7%) were male; 69.6% were receiving inhaled corticosteroids; mean±sd body mass index was 27.3±4.8 kg·m−2; mean±sd Medical Research Council dyspnoea score was 2.9±1.3. The mean±sd FEV1 was 1.45±0.54 L equating to 63.3±22% predicted. Mean±sd baseline St George's Respiratory Questionnaire total score was 40.3±26.6 and COPD Assessment Test (CAT) score was 17.2±10.7. Using the Global Initiative for Chronic Obstructive Lung Disease (GOLD) classification system, five participants were GOLD A, five were GOLD B, two were GOLD C and 34 were classified as GOLD D.
Using the exacerbation endotype classification, 33 exacerbations were bacterial, 19 eosinophilic and 21 viral. For bacterial events, the most frequently identified bacteria were Haemophilus influenzae in 54.5% of cases, followed by Moraxella catarrhalis (27.2%). Pseudomonas aeruginosa was identified in three (9.1%) cases.
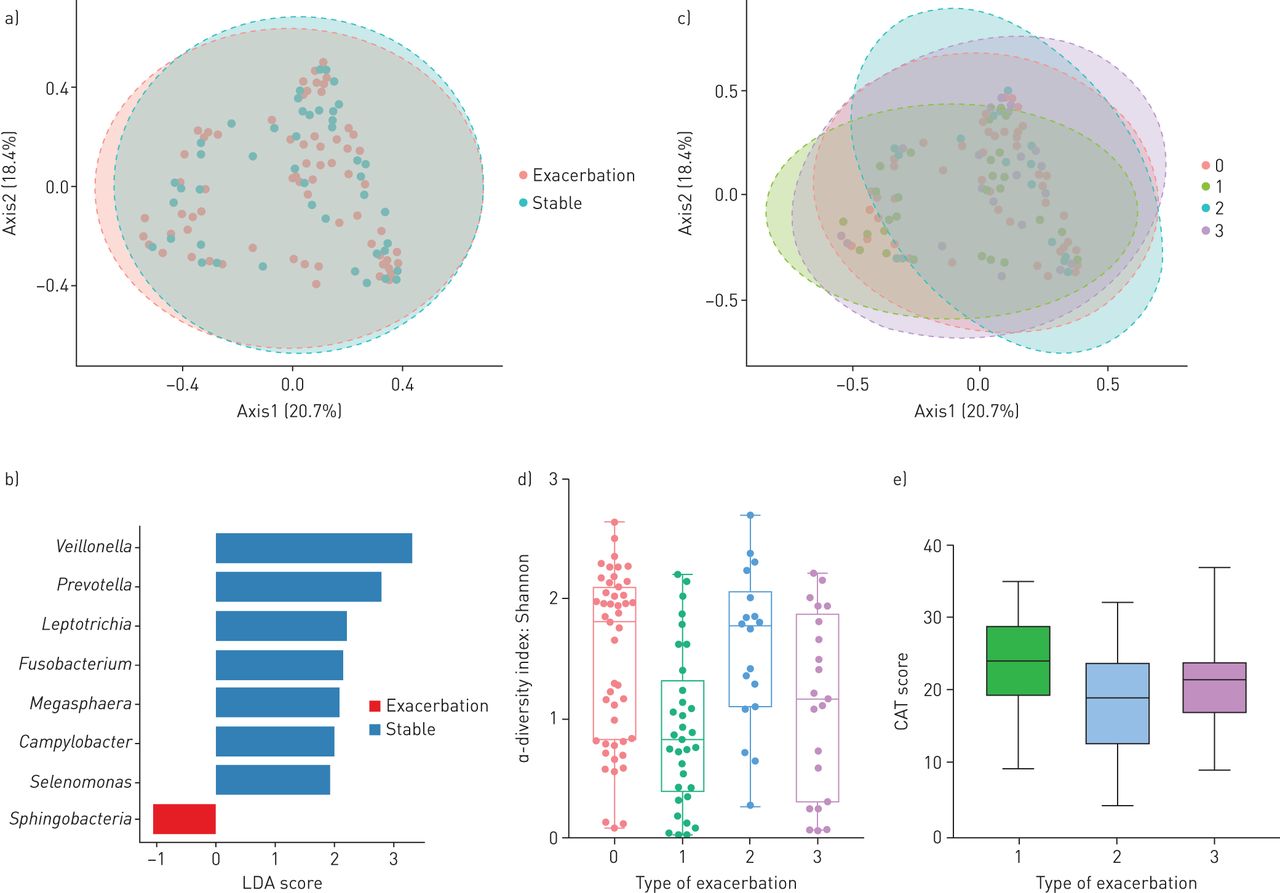
Visualising stable and exacerbation samples by principal coordinate analysis, there was no obvious clustering of stable and exacerbation samples (figure 1a). Consistent with this observation, there were no significant differences between groups by PERMANOVA (p=0.08). LEfSe identified reduced levels of Megasphaera (linear discriminant analysis (LDA) score 2.1, FDR adjusted p=0.014), Leptotrichia (LDA score 2.22, FDR adjusted p=0.043), Veillonella (LDA score 3.32, FDR adjusted p=0.043) and Campylobacter (LDA score 2.0, FDR adjusted p=0.043) at exacerbation. Prevotella was not significantly different after FDR adjustment (LDA score 2.78, p=0.059) (figure 1b). Inhaled corticosteroid use was not found to be associated with microbiome composition, in terms of either α-diversity (p=0.77) or β-diversity (p=0.86).

{kind=link}
a) Principal component analysis showing clustering of stable and exacerbation samples in the study. No differences were observed by permutational multivariate ANOVA (PERMANOVA) between the two groups (p=0.075). b) Linear discriminant analysis effect size. Features with a linear discriminant analysis (LDA) score >1 are shown. Those that reach statistical significance after false discovery rate adjustment are described in the text. Blue indicates taxa that are more abundant in stable samples, while red indicates samples more abundant in exacerbation samples. c) Principal component analysis as in (a), but with samples labelled 0–3 where 0=stable, 1=bacterial exacerbation, 2=eosinophilic exacerbation, 3=viral exacerbation or unexplained exacerbation. The ellipses are coloured according to group. The differences between exacerbation groups were statistically significant by PERMANOVA (p=0.003). d) Differences between stable and exacerbation subgroups using the Shannon diversity index as an α-diversity metric. e) Mean COPD Assessment Test (CAT) scores for each exacerbation subgroup: 1=bacterial, 2=eosinophilic, 3=viral (p=0.0067).
We concluded that there are no large differences between stable disease and exacerbation at the overall community level. Therefore, we evaluated whether there were differences between exacerbation endotypes. Classifying exacerbations as bacterial, eosinophilic or viral/other resulted in significant differences by PERMANOVA (p=0.003) (figure 1c). Differences in α-diversity were observed across the three exacerbation groups (ANOVA, p=0.0005) with a lower Shannon–Wiener diversity index, particularly in the bacterial exacerbation group (t-test, p=0.0003). There was no significant difference in Shannon diversity index between stable and exacerbation for the other groups (p=0.66 for eosinophilic and p=0.053 for viral/other by paired t-tests). Similar results were observed with different α-diversity metrics, with between group differences in Chao index (p=0.019) and Simpson's index (p=0.0024), with lower diversity again demonstrated in those exacerbations associated with positive bacterial culture.
Higher CAT scores indicate more severe symptoms during exacerbations. The mean±sd CAT scores for the three exacerbation subtypes were bacterial 24.2±6.7, eosinophilic 17.6±8.5, viral/other 21.1±7.0. The difference between bacterial and eosinophilic exacerbations was statistically significant (t-test, p=0.0067).
Our analysis demonstrates that subgrouping exacerbations into bacterial, eosinophilic and viral/other endotypes results in significant differences in microbiome composition and identifies more symptomatic exacerbations as measured by the CAT. We found, as reported by others, that there are no significant differences between stable and exacerbation microbiome profiles as a whole [6–8]. This adds to the growing literature suggesting that COPD exacerbations are heterogeneous events with diverse aetiologies and likely to require different treatments [9]. LEfSe shows that the taxa associated with a stable microbiome, which are predominantly oral taxa, constitute the largest change across the whole of the group at exacerbation. This suggests that a loss of these organisms, as opposed to increases of traditionally regarded pathogenic taxa such as Haemophilus or Pseudomonas, is the most common change observed at exacerbation. This is highly consistent with the findings from the Acute Exacerbation and Respiratory Infections in COPD (AERIS) study, where no consistent changes in Haemophilus or Streptococcus were observed comparing stability to exacerbation [4]. We show that bacterial events are associated with a significant loss of diversity and divergent changes in the overall composition of the microbiome, unlike subjects in the “eosinophilic exacerbation” endotype, who do not experience significant changes in microbiome composition. Additionally, higher CAT scores were observed in the bacterial exacerbation subgroup overall and were significantly different from the eosinophilic subgroup. This seems to confirm that bacterial and eosinophilic exacerbations are different and underscores the importance of a personalised approach to treatment.
A limitation of this study was the relatively small sample size (n=46); however, the results were concordant with the larger AERIS study (n=78) and COPDMAP cohort [4, 6]. In particular, COPDMAP, using different analysis methods identified a reduction in Veillonella at exacerbation which was replicated here [6]. As this was a study that included patients experiencing an exacerbation, there was a certain bias towards GOLD D patients, and so may be reflective of a more severe COPD population than other studies. We allowed up to two exacerbations per patient, which may introduce bias, but analysis limited to one exacerbation per subject produced similar results (not shown). Although 16 s rRNA sequencing is a powerful tool in providing a comprehensive description of the lung microbiome, it does have certain limitations, including bias towards certain bacterial taxa, exclusion of mycobacteria and viruses, and risk of contamination [6]. This study used sputum, which are typically high-biomass samples, and included appropriate negative controls to minimise contamination risk. Nevertheless, sputum is regarded as an intermediate sample between the upper and lower airway microbiome and so different results may be seen with studies utilising bronchoalveolar lavage [10].
Taken together, recent 16 s rRNA sequencing data highlight the importance of phenotyping and endotyping exacerbations. Although the microbiome is not currently an easily accessible technology for clinical practice, our analysis demonstrates that using easily available biomarkers like bacterial culture or potentially a rapid PCR test for pathogens, blood eosinophils or biomarker surrogates may be practical options and may allow more personalised treatment of exacerbations.
Shareable PDF
Supplementary Material
This one-page PDF can be shared freely online.
Shareable PDF ERJ-00391-2020.Shareable
Footnotes
Conflict of interest: H.R. Keir has nothing to disclose.
Conflict of interest: A. Dicker has nothing to disclose.
Conflict of interest: M. Lonergan has nothing to disclose.
Conflict of interest: M. Crichton has nothing to disclose.
Conflict of interest: B.E. Miller is an employee and shareholder of GSK.
Conflict of interest: R. Tal-Singer is a former employee and shareholder of GSK.
Conflict of interest: J.D. Chalmers reports grants from GlaxoSmithKline, during the conduct of the study; grants and personal fees from GlaxoSmithKline, Boehringer Ingelheim, Pfizer, Bayer Healthcare, Grifols and Insmed, grants from AstraZeneca, personal fees for consultancy from Napp and Aradigm corporation, outside the submitted work.
Support statement: This work was supported by GlaxoSmithKline. Funding information for this article has been deposited with the Crossref Funder Registry.
- Received February 22, 2020.
- Accepted May 7, 2020.
- Copyright ©ERS 2020










