





Abstract
Acute respiratory distress syndrome (ARDS) can be derived from two pathogenetic pathways: a direct insult on lung cells (pulmonary ARDS (ARDSp)) or indirectly (extrapulmonary ARDS (ARDSexp)). This review reports and discusses differences in biochemical activation, histology, morphological aspects, respiratory mechanics and response to different ventilatory strategies between ARDSp and ARDSexp. In ARDSp the direct insult primarily affects the alveolar epithelium with a local alveolar inflammatory response while in ARDSexp the indirect insult affects the vascular endothelium by inflammatory mediators through the bloodstream.
Radiological pattern in ARDSp is characterised by a prevalent alveolar consolidation while the ARDSexp by a prevalent ground-glass opacification. In ARDSp the lung elastance, while in ARDSexp the chest wall and intra-abdominal chest elastance are increased. The effects of positive end-expiratory pressure, recruitment manoeuvres and prone position are clearly greater in ARDSexp.
Although these two types of acute respiratory distress syndrome have different pathogenic pathways, morphological aspects, respiratory mechanics, and different response to ventilatory strategies, at the present, is still not clear, if this distinction can really ameliorate the outcome.
- computed tomography
- positive end-expiratory pressure
- prone position
- pulmonary and extrapulmonary acute respiratory distress syndrome
- respiratory mechanics
- ventilator-induced lung injury
Since its initial description, the acute respiratory distress syndrome (ARDS) has been considered as a morphological and functional expression of a similar underlying lung injury caused by a variety of insults. In fact, Ashbaugh et al. 1 in defining this syndrome stated that “The etiology of this respiratory distress syndrome remains obscure. Despite a variety of physical and possibly biochemical insults, the response of the lung was similar in all 12 patients. In view of the similar response of the lung to a variety of stimuli, a common mechanism of injury may be postulated”.
This observation used the term syndrome to refer to “a group of symptoms and signs of disordered function related to one another by means of some anatomic, physiologic, or biochemical peculiarity” 2. In 1994, the American-European Consensus Conference defined two pathogenetic pathways leading to ARDS: a direct (“primary” or “pulmonary”) insult, that directly affects lung parenchyma, and an indirect (“secondary” or “extrapulmonary”) insult, that results from an acute systemic inflammatory response 3. The differentiation between direct and indirect insult is often straightforward as for primary diffuse pneumonia or ARDS originating from intra-abdominal sepsis. In other situations, the precise identification of the pathogenetic pathway is somewhat questionable, as for trauma or cardiac surgery. The distinction, however, was mainly speculative until Gattinoni et al. 4 reported possible differences in the underlying pathology, respiratory mechanics, and response to positive end-expiratory pressure (PEEP) in pulmonary ARDS (ARDSp, primarily pneumonia) and extrapulmonary ARDS (ARDSexp, primarily due to abdominal disease). In table 1⇓ are reported the underlying etiologies in ARDSp and ARDSexp. Since then, the distinction between ARDSp and ARDSexp has gained attention and an increasing number of papers on this subject have appeared in the scientific literature 5–8.
Underlying etiologies of pulmonary and extrapulmonary acute respiratory distress syndrome
However, it is increasingly debated whether distinction between ARDSp and ARDSexp is only anecdotic or can have a clinical impact on therapeutic strategies 9–11.
This review, reports and discusses possible differences in ARDS of different origins regarding: 1) epidemiology, 2) pathophysiology, 3) morphological aspects, 4) respiratory mechanics, 5) ventilatory strategies, 6) response to pharmacological agents and 7) long-term recovery.
Epidemiology
ARDS occurs following a variety of risk factors 12. A strong evidence that supports a cause-and-effect relationship between ARDS and risk factors was identified for sepsis, trauma, multiple transfusions, aspiration of gastric contents, pulmonary contusion, pneumonia, and smoke inhalation. However, only a few studies have investigated the prevalence and mortality considering ARDSp and ARDSexp. In the majority of available studies the prevalence of ARDSp was higher compared to ARDSexp, varying from 47 to 75% of all cases 4–6, 13–15. In the most recent retrospective analysis of patients enrolled in the Acute Respiratory Distress Syndrome Network (ARDSNet) trial of low tidal volume ventilation, roughly an equal proportion of ARDSp and ARDSexp was identified 16. It has been reported that pulmonary trauma was associated with higher survival rate, whereas opportunistic pneumonia had a lower survival rate 17, 18. Among complications, acute renal failure, pulmonary infection, and bacteraemia seem to be independent factors associated with increased mortality 19. However, the reported mortality in patients with ARDS attributable to pulmonary and extrapulmonary causes varies considerably. In one study a direct pulmonary insult triggering ARDS was identified as being associated with increased mortality 20, whereas in another study no relationship was found between direct pulmonary insults and increased mortality (36% and 34% mortality for pulmonary and extrapulmonary causes, respectively) 16. Moreover, in the same cohort of patients, the proportion of patients in whom organ failure developed, the pulmonary and extrapulmonary were equal between groups, and the proportion achieving liberation from mechanical ventilation at 28 days was also identical. The lack of agreement among various studies can be explained by differences in: 1) baseline status; 2) the prevalence of the disease precipitating ARDS in each centre; 3) the impact of therapy; and 4) the overall distribution of these factors in the studied population. Thus, it is not known whether different clinical management and ventilatory treatment modified accordingly with the different pathophysiological characteristics could improve outcome. In the current authors' opinion, the distinction between ARDSp and ARDSexp should not be focused, at the moment, on possible differences in morbidity and mortality. It is more important first to understand if this distinction is truly large and carries major implications for clinical management. If it does, further studies on morbidity and mortality would be reasonable once differences in clinical strategy were clarified.
Pathophysiology
The alveolar-capillary barrier is formed by two different structures, the alveolar epithelium and the vascular endothelium. Traditionally, it has been though that insults applied to the lung, through the airways or the circulation, result in diffuse alveolar damage. Although many insults may converge in the stage of ARDS, the present authors wonder if, in early stages, a direct or indirect insult to the lung may have different manifestations 21. The different histological and biochemical alterations in ARDSp and ARDSexp are reported in table 2⇓.
Histological and biochemical alterations in pulmonary and extrapulmonary acute respiratory distress syndrome
Evidence of histological and biochemical alterations in experimental models of pulmonary and extrapulmonary acute respiratory distress syndrome
A direct insult has been studied in experimental models by using intratracheal instillation of endotoxin 22, complement 23, tumour necrosis factor (TNF) 24, or bacteria 25. After a direct insult, the primary structure injured is the alveolar epithelium, while the capillary endothelium is roughly normal 26. This causes activation of alveolar macrophages and neutrophils and of the inflammatory network, leading to intrapulmonary inflammation. An increased amount of apoptotic neutrophils and alterated type I and type II cells has been reported as well as an increase in interleukins (IL)‐6, 8 and 10 in the bronchoalveolar lavage (BAL) in direct injury compared to indirect injury 26. The prevalence of the epithelial damage determines a localisation of the pathological abnormality in the intra-alveolar space, with alveolar filling by oedema, fibrinous exudate, collagen, neutrophilic aggregates, and/or blood, with a minimum interstitial oedema. This pattern has often been described as pulmonary consolidation, probably representing a combination of alveolar collapse and prevalent fibrinuous exudates and alveolar wall oedema in ARDSp.
An indirect insult has been studied in experimental models by intravenous 27 or intraperitoneal 28 toxic injection. After an indirect insult, the lung injury originates from the action of inflammatory mediators released from extrapulmonary foci into the systemic circulation. In this case, the first target of damage is the pulmonary vascular endothelium, with an increase of vascular permeability and interstitial oedema. A decreased amount of apoptotic cells has been described in experimental model of ARDSexp as well as a decreased amount of ILs in the BAL 26. Thus, the pathological alteration due to an indirect insult is primarily microvascular congestion and interstitial oedema, with relative sparing of the intra-alveolar spaces. Recently Rocco et al. 29 investigated the effect of corticosteroids in the ARDSp and ARDSexp. They found that steroids inhibited extracellular matrix remodelling independently from the etiology but their ability to attenuate the inflammatory response was greater in ARDSp.
Evidence of histological and biochemical alterations in patients with pulmonary and extrapulmonary acute respiratory distress syndrome
Histologically the ARDS lung is characterised by diffuse lung damage with subdivision of temporal course in early and late lesions, designated as acute and chronic fibroproliferative diffuse alveolar damage 30, 31. The acute stage of diffuse lung damage by interstitial and intra-alveolar oedema and hyaline membrane 30. This stage is followed by consecutive proliferation by fibroblastic cells characterised by chronic and or fibroproliferative damage. The disease process finally leads to the gross destruction of the pulmonary lobes resulting in fibrosis and honeycombing. A recent study Hoelz et al. 32 described the morphological differences between pulmonary lesions in patients with ARDSp and ARDSexp. They found a predominance of alveolar collapse, fibrinous exudate and alveolar wall oedema in ARDSp. However the acute inflammatory phase of lung injury is also associated with fibroproliferative response that leads to alveoli obliteration and derangement in the spatial distribution of the extracellular matrix. In a recent study, Negri et al. 33 reported an increased collagen content in ARDSp than in ARDSexp in the early phase of the disease, while no differences were observed concerning the elastic fibres content. They concluded that extracellular matrix remodelling occurs early in the development of ARDS and appears to depend on the site of the initial insult, being prevalent in ARDSp.
From animal experiments an increase of inflammatory agents in the BAL in ARDSp, while in the serum in ARDSexp, is expected. Chollet-Martin et al. 34 found an increase in BAL and serum of IL‐8 in extrapulmonary ARDS 34 as well as Bauer et al. 35 who found an increased level of serum TNF‐α in patients with ARDSexp compared to ARDSp. Shutte et al. 36 found high levels of IL‐6 and IL‐8 in the BAL irrespectively of the etiology in the first 10 days of intubation 36. However, as expected with time the BAL levels of IL‐6 and IL‐8 decreased in ARDSexp while not in ARDSp.
These experimental and in vivo findings suggest that the damage in the early stage of direct insult is primarily focused on the alveolar epithelium, whereas in indirect injury on the vascular endothelium. The inflammatory agents are more increased in the serum in ARDSexp, while in the BAL in ARDSp. However, it is worth noting the possible co-existence of the two insults: one lung with direct injury (as pneumonia) and the other with indirect injury (through mediator release from the original pneumonia) 37.
Morphological aspects
In recent years, a number of studies have identified differences by chest radiography and computed tomography (CT) between ARDSp and ARDSexp.
Chest radiography
The current authors retrospectively scored the chest radiographs, performed in a standardised way, in 21 ARDS patients (9 ARDSp and 12 ARDSexp), to identify the amount of “hazy” and “diffuse” lung densities likely representing interstitial oedema and compression atelectasis, and patchy densities likely representing pulmonary consolidations 5. Patients with ARDSp presented an increased amount of patchy densities compared to ARDSexp. No significant differences were found between the right and the left lung. Overall the lung injury severity scores were significantly higher in patients with ARDSp.
Computed tomography scan
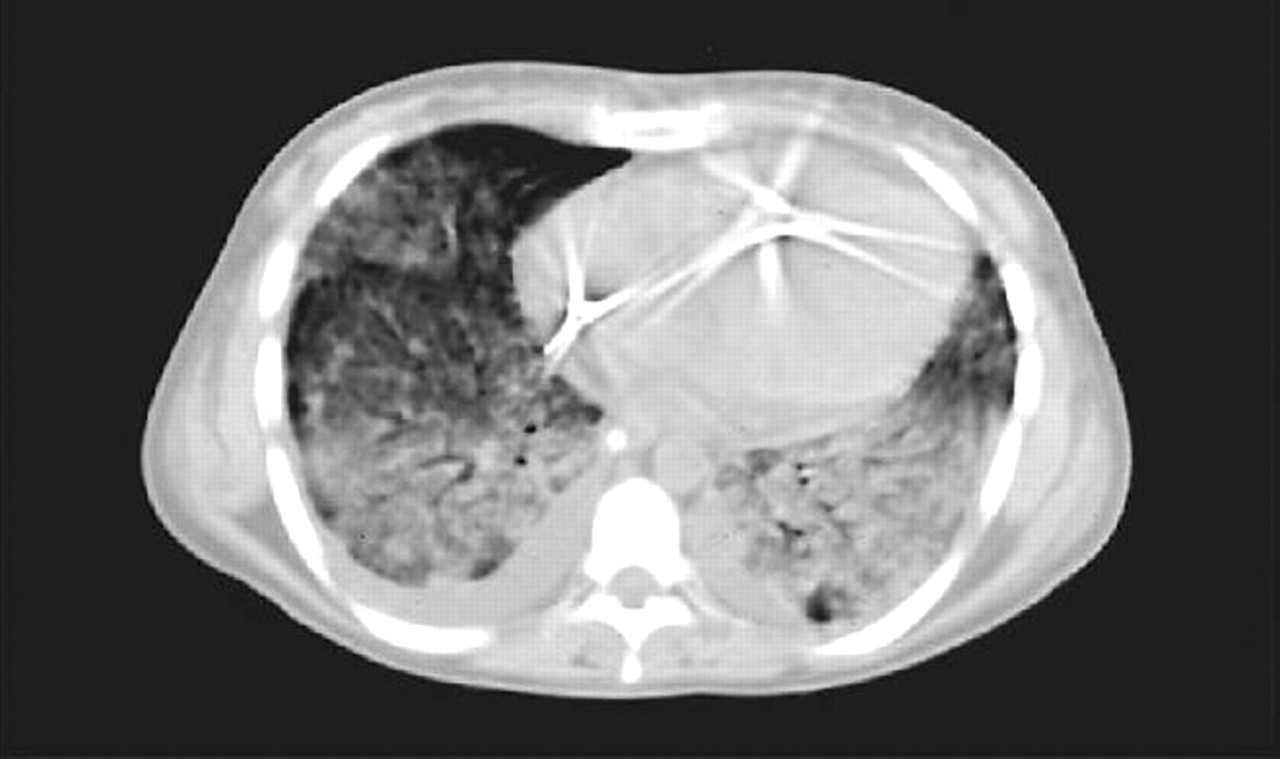
Goodman et al. 6 studied 33 ARDS patients (22 ARDSp and 11 ARDSexp) by performing three representative scans at the apex (top of the upper aortic arch), at the hilum (first section below the carina), and at the base (2 cm above the highest diaphragm). The ventilatory setting was not standardised during scans. The lung was scored as follows: “normal lung,” “ground-glass opacification” (mild increased attenuation with visible vessels), and “consolidation” (markedly increased attenuation with no visible vessels). They found that in ARDSexp, ground-glass opacification was more than twice as extensive as consolidation (fig. 1⇓). This contrasted markedly with ARDSp, in which there was an even balance between ground-glass opacification and consolidation (fig. 2⇓). When the type of opacification between the two groups was compared, the patients with ARDSexp had 40% more ground-glass opacification than did those with ARDSp. Conversely, the ARDSp patients had >50% more consolidation than did those with ARDSexp. The authors also found differences in the regional distribution of the densities. In ARDSexp ground-glass opacification was greater in the central (hilar) third of the lung than in the sternal or vertebral third. There was no significant craniocaudal predominance for ground-glass opacification or consolidation, but consolidation showed a preference for the vertebral position over the sternal and central positions. In ARDSexp ground-glass opacification was evenly distributed in both the craniocaudal and sternalvertebral directions. Consolidation tended to favour the middle and basal levels, but also favoured the vertebral position. The total lung disease was almost evenly distributed between the left and right lungs in both ARDSp and ARDSexp. However, grossly asymmetric disease was always due to asymmetric consolidation. Moreover, the presence of air bronchograms and pneumomediastinum were prevalent in ARDSp, while emphysema-like lesions (bullae) were comparable in both groups.

A computed tomography scan of extrapulmonary acute respiratory distress syndrome at end-expiration. There is a predominantly ground-glass opacification.

A computed tomography scan of pulmonary acute respiratory distress syndrome at end-expiration. There is extensive consolidation, with an approximately equal amount of normal lung and ground-glass opacification and air bronchograms.
Unfortunately, it appears that the word consolidation may have different meanings in different contexts. In radiology, consolidation simply means a “marked increase in lung attenuation with no visible vessels,” and it may derive from alveolar atelectasis as well as alveolar filling. In pathology, consolidation refers only to alveolar filling.
D'Angelo et al. 38 reported homogeneous diffuse interstitial and alveolar infiltration, without evidence of atelectasis, in eight patients with ARDSp due to Pneumocystis carinii, whereas Winer-Muran et al. 39 found that dependent atelectasis were more common in patients with early ARDSexp compared to ARDSp.
Desai et al. 40 reported a significantly higher incidence of intense parenchymal opacification in nondependent areas of the lung in patients with direct insults (indicative of consolidation secondary to inflammatory infiltrate), but no other differences emerged between the two groups. Moreover, the extent of intense parenchymal opacification in nondependent areas of the lung was inversely related to the time from intubation to CT. The authors concluded that differentiating between ARDSp and ARDSexp on the basis of CT findings is not straightforward, and that no single radiological feature is specifically associated with lung injury of either type.
Others observations were obtained by Rouby et al. 41 in 69 ARDS patients (49 ARDSp and 20 ARDSexp) in whom a CT scan of the whole lung was performed. CT densities were classified as consolidation or ground-glass opacification. Consolidation was defined as a homogeneous increase in pulmonary parenchymal attenuation that obscures the margins of the vessels and airway walls. Ground-glass opacities were defined as hazy, increased attenuation of the lung but with preservation of bronchiolar and vascular margins. The patient was classified as having a “lobar” pattern if areas of lung attenuation had a lobar or segmental distribution established on the recognition of anatomical structures such as the major fissure or the interlobular septa, a “diffuse” pattern if lung attenuation were diffusely distributed throughout the lungs, and “patchy” pattern if there were lobar or segmental areas of lung attenuation in some parts of the lungs but lung attenuation without recognised anatomical limits in others. They found that ARDSp was more frequent among patients with diffuse and patchy attenuation, whereas ARDSexp was more common in patients with lobar attenuation.
Patients with head injury have been shown to be at particularly high risk of ventilator-associated pneumonia (VAP) 42. Its incidence is estimated to reach 40–50%. The most frequent etiological agents include Staphylococcus aureus, and less frequently, Streptococcus pneumoniae and Hemophilus influenzae 43. The early onset of pulmonary infection and the peculiar microbial pattern may be due to oropharyngeal or gastric colonisation followed by high inoculums aspiration of oropharyngeal secretion. This represents an excellent “in vivo” model of direct pneumonia (i.e. ARDSp) in humans. Recently, the present authors' investigated by CT scan the morphological lung alterations in patients with head injury, of traumatic and nontraumatic origin, developing severe respiratory insufficiency (arterial oxygen tension (Pa,O2)/inspiratory oxygen fraction (FI,O2) <200 and bilateral infiltrates) within the first week of mechanical ventilation (early onset pneumonia) 44.
The CT scans were classified as by Goodman et al. 6. The current authors found that all the patients showed consolidation opacities in the dependent part of the lung (fig. 3a⇓). However differently from ARDSp originating from community-acquired pneumonia, in VAP the amount of aerated lung was increased while ground-glass opacification was less compared to community-acquired pneumonia. However, when these patients were turned prone a marked reduction of previously dependent densities was found (nondependent in prone, fig. 3b⇓). This suggests that lung areas previously considered consolidated due to VAP, were not really consolidated but mainly atelectatic. Application of recruitment manoeuvres or PEEP (up to 15 cmH2O) were unsuccessful to reopen these zones in supine position, likely because of a marked inhomogeneity of pulmonary parenchyma (well aerated-elastic in nondependent and nonaerated-stiff in dependent zones) 45. Thus, it is possible to hypothesise that the pathophysiology and the lung morphology in ARDSp may be different in community-acquired pneumonia and VAP. It is possible that the period of time from the infection and the development of severe respiratory failure (usually within 1 week), can favour some initial diffusion of inflammatory agents, which can explain the presence of amounts of ground-glass opacification in ARDSp from community-acquired pneumonia. Moreover, the aggressive therapeutic management VAP, and thus a potential reduction in release of inflammatory agents in the peripheral circulation, may limit the radiological pattern to consolidation and/or atelectasis.

{kind=link}
{kind=link}
{kind=link}
A computed tomography scan of pulmonary acute respiratory distress syndrome due to ventilator-associated pneumonia at end-expiration. a) Supine position with extensive bilateral apparent consolidations; b) prone position, with an almost total clearing of the apparent consolidations. This indicates the atelectatic nature of the densities.
With all the limits and somewhat arbitrary classification of patients and interpretation of morphological observation, these findings support the hypothesis that the radiological pattern is different in ARDSp and ARDSexp. It can be concluded that: 1) in ARDS, the increase in the lung densities is most prominent in the dependent lung regions in the supine position but may, in a minority of patients, be more homogeneously distributed throughout the lung parenchyma; 2) in ARDSp due to community-acquired pneumonia, two prevalent patterns have been described: the first, extensive consolidation and air bronchograms in the dependent part of the lung together with ground-glass opacification, or the second, homogeneous diffuse interstitial and alveolar infiltration, without evidence of atelectasis; 3) in ARDSp, due to VAP, densities in the dependent part of the lung (likely atelectasis) are prevalent with the remaining nondependent lung substantially normal; and 4) on the contrary in ARDSexp, there is predominantly ground-glass opacification.
Respiratory mechanics
Traditionally, the mechanical alterations of the respiratory system observed during ARDS were attributed to the lung because the chest wall elastance was considered nearly normal 46. Studies in which respiratory system, lung, and chest wall mechanics were partitioned have proved this assumption wrong. The present authors consistently found that the elastance of the respiratory system was similar in ARDSp and ARDSexp, but the elastance of the lung was higher in ARDSp, indicating a stiffer lung 4. Conversely, the elastance of the chest wall was more than twofold higher in ARDSexp than in ARDSp, indicating a stiffer chest wall. The increase in the elastance of the chest wall was related to an increase in the intra-abdominal pressure, which was threefold greater in ARDSexp. In critically ill patients, data on intra-abdominal pressure are surprisingly scanty. In most of the current authors' patients, the elevated values could be explained by primary abdominal disease or oedema of the gastrointestinal tract. The sonographic findings of the abdomen were analysed in normal spontaneously breathing subjects, in patients with ARDSexp due to abdominal sepsis, and in patients with ARDSp due to community-acquired pneumonia 44. In the normal subjects it was difficult to recognise the abdominal wall and the gut anatomical structure. In the patients with ARDSexp and related abdominal problems, the increased dimension and thickness of the gut, with intraluminal debris and fluid and with reduced peristaltic movements, were visible. In the patients with ARDSp, the dimension of the gut were slightly increased while the gut wall thickness was not increased, without any consistent debris or fluid. Thus, it is evident that patients with abdominal problems present important anatomical alterations of the gut, which can explain the increased intra-abdominal pressure. Thus, these findings suggest that in ARDS the increased elastance of the respiratory system is produced by two different mechanisms: in ARDSp a high elastance of the lung is the major component, whereas in ARDSexp increased elastance of the lung and of the chest wall equally contributed to the high elastance of the respiratory system. Moreover, it was found that respiratory resistance, partitioned into its airway and viscoelastic components, was comparable in ARDSp and an ARDSexp. However, the resistance of the chest wall was also elevated in ARDSexp and significantly correlated to intra-abdominal pressure, suggesting that intra-abdominal pressure can affect the viscoelastic properties of the thoracoabdominal region.
However, it is important to consider that most of the patients in the extrapulmonary group had ARDS caused by intra-abdominal pathological conditions, and it seems likely that some of the changes seen in chest wall elastance relate to intra-abdominal mechanics and effects on diaphragmatic movements. Altered lung elastance with relatively normal chest wall elastance was also found in patients affected by severe P. carinii pneumonia 38, and in patients with VAP 44that usually present the same histopathology as ARDSp. Similarly Ranieri et al. 47 reported a marked alteration in chest wall mechanics in patients with ARDSexp, while not in ARDSp. Different findings were reported by Rouby et al. 41 in which a significantly lower respiratory system compliance (higher elastance) and worse oxygenation was demonstrated in the pulmonary group. All these data suggest the importance of respiratory partitioning for a better characterisation of the pathology underlying ARDS and an improvement in clinical management.
Ventilatory strategies
The most important consequence of the different respiratory mechanics in ARDSp and ARDSexp is that for a given applied airway pressure, the transpulmonary pressure (i.e. the distending pressure of the lungs), is lower in ARDSexp. Indeed, the main differences between ARDSp and ARDSexp seems to be: 1) a different underlying pathology (prevalent consolidation versus prevalent collapse); and 2) a different transpulmonary pressure for the same applied airway pressure.
Lung protective ventilation (low tidal volume)
The ARDSNet trial of low tidal volume ventilation strategy showed a reduction in mortality with the use of a protective ventilatory strategy (tidal volumes 6 mL·kg−1 versus 12 mL·kg−1) 48. In a post hoc subgroup analysis according to pulmonary or extrapulmonary causes of ARDS no difference was found between the two groups in terms of the beneficial effect of this type of ventilation 16.
Positive end-expiratory pressure and recruitment
The differences in underlying pathology and respiratory mechanics may have clinical consequences. In fact, the potential for recruitment is higher in alveolar collapse and lower in alveolar consolidation. On the other hand the applied pressures for lung recruitment may lead to different transpulmonary pressures according to chest wall elastance. This hypothesis is supported by the finding that in ARDSp, increasing PEEP mainly induced overstretching, while in ARDSexp PEEP mainly induced recruitment. Gattinoni et al. 4 found that an increase of PEEP leads to opposite effects on elastance. In ARDSp, increasing PEEP caused an increase of the elastance of the total respiratory system due to an increase in lung elastance with no change in chest wall elastance. Conversely, in ARDSexp the application of PEEP caused a reduction of the elastance of the total respiratory system, mainly due to a reduction in lung elastance and chest wall elastance. Moreover, although an increased PEEP led to an elevation of end-expiratory lung volume in both ARDSp and ARDSexp, it resulted in alveolar recruitment primarily in ARDSexp. In neuro-injured patients with “pure” VAP and severe respiratory insufficiency, the current authors found no beneficial effects on respiratory mechanics, alveolar recruitment, or gas exchange with PEEP or recruitment manoeuvres 44, 45, 49.
Really, in the study by Gattinoni et al. 4 the majority of the patients had ARDSp due to VAP, poorly responding to PEEP and recruitment manoeuvres. Thus, the current authors believe that future studies are warranted to better elucidate possible differences in the pathophysiology of community-acquired pneumonia and VAP.
A proposed intervention to facilitate alveolar recruitment in ARDS other than application of PEEP is the introduction of regular “sigh” breaths into the ventilator setting. Although there is a controversy regarding the long-term benefit of this type of ventilatory adjunct, the measured benefits (increased alveolar recruitment, improved oxygenation, and reduced shunt) seem to be greater in patients with ARDSp than in those with ARDSexp 50.
These clinical findings are in line with the results obtained in pathological studies and animal experiments.
In a very elegant morphological study, Lamy et al. 51 found that in patients in whom gas exchange did not improve with PEEP in early ARDS, severe lung tissue damage resulted, with alteration of alveolar spaces by haemorrhage and purulent exudate, whereas the responders to PEEP had less severe lung damage but diffuse congestion, microatelectasis, and some alveolar damage 51. However, it is possible that different responses to PEEP disappear in late ARDS where the lung structures undergo important changes such as remodelling and fibrosis 52. Comparing three different experimental models of acute lung injury during recruitment manoeuvres, Van der Kloot et al. 53 found that more alveolar recruitment occurred in the oleic acid model, similar to ARDSexp, compared with the model of intratracheal instillation of bacterial pneumonia, more similar to ARDSp.
Inconsistent with these findings, two recent studies found a similar response to PEEP on alveolar recruitment and oxygenation in patients with ARDSp and ARDSexp 8, 54. This could reflect differences in the clinical characteristics of the population investigated or in the ventilatory and clinical management at the moment of the study.
In sum, this data indicate that in the presence of “pure” pulmonary consolidation, the use of recruitment manoeuvres and levels of high PEEP are less beneficial and, sometimes, even deleterious.
Prone position
If chest wall mechanics, intra-abdominal pressures, and underlying pathology are different in ARDSp and ARDSexp, it is not surprising that the response to prone position may also be different. In fact, several factors that are different between ARDSp and ARDSexp (i.e. chest wall elastance and regional transpulmonary pressure), are likely involved in determining the response to prone position 55.
Two recent small studies investigated the possible differences in the response in oxygenation to prone position in ARDSp and ARDSexp 55–56. Lim et al. 56, in a 2‐h physiological study, investigated 47 patients (31 ARDSp and 16 ARDSexp). They showed that the effect of prone position on respiratory function appears to be different in patients with early ARDSp and ARDSexp. Briefly they found that in prone position: 1) the response in oxygenation (defined as an increase of Pa,O2/FI,O2 >40% from baseline) was more marked in ARDSexp compared with ARDSp (63% versus 23% at 0.5 h, and 63% versus 29% at 2 h, respectively); 2) the rate of increase in oxygenation was slower in ARDSp; 3) the decrease of respiratory system compliance was greater in ARDSexp; 4) the densities determined on the chest radiograph, decreased to a greater degree in ARDSexp.
On the contrary, Rialp et al. 57 found no difference in gas-exchange improvement between patients with pulmonary and extrapulmonary ARDS when turned prone.
Recently, Pelosi et al. 15 performed a large prospective trial in 73 patients (51 ARDSp and 22 ARDSexp) with bilateral chest infiltrates, a Pa,O2/FI,O2 ratio <200 with PEEP ≥5 cmH2O, and no evidence of cardiac problems. Patients were evaluated daily for a 10-day period for the presence of respiratory failure criteria (the same as entry criteria). Patients who met these criteria were placed in a prone position for 6 h once a day. The improvement in oxygenation was greater in ARDSexp compared with ARDSp, although the overall mortality was not different between the two groups.
The different time course of oxygenation according to the etiology of ARDS suggests that the mechanisms of oxygenation in the prone position may be multifactorial or time-dependent, or both. An attenuation of the vertical gradients of the pleural pressure, or an increased effective transpulmonary pressure at the dependent lung regions, is obtained immediately as the patients are turned to the prone position. This mechanical benefit could then result in the reversal of compressive atelectasis in ARDSexp, but would not bring about an immediate change in the consolidated lung units in ARDSp. The greater decrease in consolidation densities in the prone position of ARDSexp as compared with ARDSp suggests that the effects of position and the mechanism through which it may improve respiratory function can be different in ARDSp and ARDSexp. In ARDSexp, in which collapse and compression atelectasis together with an increase of intra-abdominal pressure play a major role in inducing hypoxia 58, the redistribution of atelectasis from dorsal to ventral 59 and possibly the changes in regional transpulmonary pressure 60 may induce an immediate improvement of oxygenation. ARDSp, in which collapse is likely less relevant, the same mechanism may operate to a lesser degree and possibly the redistribution of ventilation may play an additional role. These two studies reinforce the hypothesis that the mechanism by which prone position improves oxygenation may be different or may operate to different degrees in ARDSp and ARDSexp.
Response to pharmacological agents
Several drugs have been unsuccessfully used to improve outcome in ARDS, but few trials have compared the effects of drugs between ARDSp and ARDSexp.
Inhaled nitric oxide and nebulised prostacyclin
Both inhaled nitric oxide (iNO) and nebulised prostacyclin have been extensively studied in ARDS. Both have been shown to improve oxygenation, possibly causing vasodilation in ventilated areas, thereby improving ventilation-perfusion matching and decreasing pulmonary vascular resistance.
Rialp et al. 57 compared the effects of iNO with or without placement in the prone position in ARDSp and ARDSexp. They found a significant improvement in oxygenation due to iNO prevalently in the pulmonary group. Furthermore, the number of patients responding to iNO at all was significantly higher in the pulmonary group than in the extrapulmonary one. The authors suggested that this difference in response related to the greater degree of intrapulmonary shunting that occurs in ARDSp (where consolidation appears to predominate over atelectasis) which is partially corrected by the vasoactive properties of iNO. However, other authors have been unable to demonstrate a significant difference between ARDSp and ARDSexp in terms of the proportions of patients showing improved oxygenation in response to iNO 61.
Nebulised prostacyclin has effects similar to those of iNO in patients with ARDS. In a recent study Domenighetti et al. 62 examined the response to inhaled prostacyclin in ARDSp and ARDSexp. They found a more marked improvement in oxygenation in ARDSexp, associated with less morphological alterations as examined at the CT scan. The authors concluded that the clinical recognition of the two types of the syndrome together with CT analysis may be associated with better prediction of the prostacyclin‐2 nebulisation response on oxygenation.
Long-term recovery
In long-term follow-up of survivor ARDS patients the pulmonary function test showed a reduction of diffusion capacity and exercise tolerance in the 6‐min walking test similar to patients with chronic obstructive disease associated with normal blood gas value 63. The assessment of lung function of survivors of ARDS 6 month after hospital discharge suggested that long-term function recovery is identical between ARDSp and ARDSexp 20.
Conclusions
ARDSp and ARDSexp are different diseases and not just a useful concept. ARDSp and ARDSexp are characterised by different pathophysiological, biochemical, radiological, and mechanical patterns: 1) in ARDSp, the prevalent damage in early stages is likely intra-alveolar, whereas in ARDSexp is interstitial oedema with a greater amount of inflammatory agents in the blood stream; 2) the radiological pattern, from chest radiograph or CT, is different in ARDSp (characterised by prevalent consolidation) and ARDSexp (characterised by prevalent ground-glass opacification); 3) in ARDSp lung elastance is more markedly increased than in ARDSexp, where the main abnormality is the increase in chest wall elastance, due to abnormally increased intra-abdominal pressure; 4) PEEP, inspiratory recruitment, and prone position more effectively improved respiratory mechanics, alveolar recruitment, and gas-exchange in ARDSexp. The response to inhaled drugs can be different in ARDSp and ARDSexp.
Further studies are warranted to better define whether the distinction between acute respiratory distress syndrome of different origins can really improve clinical management and survival.
Acknowledgments
The authors are particularly indebted to E.M. Negri and C. Hoelz (Division of Respiratory Diseases, University of Sao Paulo, School of Medicine, Sao Paulo, Brazil) for their useful suggestions and for the iconographic materials for the preparation of the manuscript.
- computed tomography
- positive end-expiratory pressure
- prone position
- pulmonary and extrapulmonary acute respiratory distress syndrome
- respiratory mechanics
- ventilator-induced lung injury
- © ERS Journals Ltd
References









