Article Text

Abstract
Background: Fabry’s disease is an X-linked lysosomal storage disorder characterised by deficient activity of the enzyme α-galactosidase A.
Aim: To study eye abnormalities in patients with Fabry’s disease in the Fabry Outcome Survey (FOS).
Methods: This is the largest study of ocular manifestations in patients with Fabry’s disease. In all, 173 of the 688 patients enrolled in FOS underwent a detailed ophthalmic examination, with a special focus on abnormalities of the cornea, lens, conjunctival and retinal vessels.
Results: Cornea verticillata was reported in 76.9% of females and 73.1% of males; vessel tortuosity was observed in 21.9% of females and in 48.7% of males. Fabry cataract was recorded in 9.8% of females and in 23.1% of males. Cornea verticillata was therefore the most frequently reported ophthalmic abnormality in Fabry’s disease in both hemizygotic males and heterozygotic females. Tortuous conjunctival and retinal vessels and Fabry cataract were more frequently found in males than in females. Vessel tortuosity was more frequently observed in patients with a higher severity score and greater impairment of renal and cardiac function, suggesting that it may be associated with a more severe disease. The youngest patient with ocular changes was 3 years old. The prevalence of tortuous vessels in males increased with age.
Conclusion: The presence of cornea verticillata is a useful aid in the diagnosis of Fabry’s disease, as it is often present at the time of diagnosis. Vessel tortuosity may have some predictive value for systemic involvement.
- ERT, enzyme replacement therapy
- FOS, Fabry Outcome Survey
- MSSI, Mainz Severity Score Index
Statistics from Altmetric.com
Fabry’s disease is an X-linked lysosomal storage disorder characterised by deficient activity of the enzyme α-galactosidase A, with progressive deposition of sphingolipids within the lysosomes of different cells and organs.1,2 The estimated incidence of Fabry’s disease is 1 in 40 000–117 000 live births for males,3,4 and there is increasing recognition that disease-related complications can develop in heterozygotic females. The variable presentation and the large number of tissues and organs involved can often lead to misdiagnosis, or delayed diagnosis often for several years. Previously, treatment was limited to symptomatic relief; however, the recent advent of enzyme replacement therapy (ERT) has provided a safe and effective alternative to earlier treatment modalities.5
In Fabry’s disease, ophthalmological abnormalities occur mostly at the level of the conjunctival and retinal vessels, the cornea and the lens. They correlate with a progressive deposition of glycosphingolipids in ocular structures.6,7,8,9,10,11,12
Conjunctival and retinal vessels are tortuous and may exhibit aneurysmal dilatations.13,14 A vortex keratopathy (“cornea verticillata”) represents the ocular manifestation most commonly reported in Fabry’s disease.15–18 A small number of patients exhibit a typical lens opacity with a “spoke-like” pattern at the level of the posterior capsule, usually referred as a “Fabry cataract”.6,7
These signs can be detected by a basic slit-lamp examination, a procedure that is non-invasive, inexpensive and not time consuming.
The subtle eye manifestations of Fabry’s disease are visually insignificant to the patient, and therefore do not increase patient referrals to an ophthalmologist. However, they may prove to be useful in the diagnosis, in understanding the natural history of the disease and in assessing the response to treatment.
The analysis of eye abnormalities in patients with Fabry’s disease represents a significant part of the Fabry Outcome Survey (FOS), a European database for all patients with Fabry’s disease who are receiving, or are candidates for, ERT with agalsidase α.19 FOS represents the most comprehensive database of patients with Fabry’s disease, and offers a unique opportunity to study a large number of individuals affected by this rare disorder.
Here, we describe the clinical features of the common ophthalmic manifestations of Fabry’s disease, as recorded in the FOS, with special emphasis on the practical implications for the diagnosis and management of these patients.
METHODS
FOS data were collected by 74 centres providing treatment for Fabry’s disease throughout Europe, with the approval of the ethical review board of each participating centre. All patients gave written informed consent. On enrollment into FOS, each patient’s medical history, including the year of diagnosis, and signs and symptoms of the disease and treatment, was documented by a doctor. In all, 173 of the 688 (25.1%) patients enrolled in the FOS underwent a detailed ophthalmological examination, with special focus on the cornea, lens, and conjunctival and retinal vasculature. In the centres participating in the study, the diagnosis of the eye abnormalities was done on the basis of the doctors’ personal experience and pictures and descriptions reported in the literature. The ophthalmologists were only asked to report the presence or absence of the specific ocular signs, without any attempt to grade the severity of the ocular manifestations.
Vessel tortuosity was defined as tortuous conjunctival and/or retinal vessels. The assumption was that the pathogenesis of vessel tortuosity was essentially the same in both the anterior and posterior eye segments.
Depersonalised data were submitted electronically to the central FOS database. The prevalence of eye manifestations was analysed in the general FOS population according to sex and age. The possible local association of different ocular signs in the same eye was also studied, and the correlation between eye abnormalities and the severity of systemic involvement was investigated.
Differences in the prevalence of ocular manifestations according to sex and age were analysed using contingency tables. Patients were divided into three groups according to age: <20 years, 20–40 years and >40 years. The same method was used to investigate the concurrence of different eye abnormalities. Differences in disease progression were analysed using the linear regression of disease severity after adjusting for age, sex and a class variable that accounts for the difference in slope of the age-related progression between patients who had eye abnormalities and those who did not. The severity of the disease was measured using an adaptation of the Mainz Severity Score Index (MSSI),20 the FOS Severity Index (FOS-MSSI),21 which is a scoring system developed to measure the severity of Fabry’s disease. The MSSI is composed of four sections that cover the general, neurological, cardiovascular and renal signs and symptoms of Fabry’s disease, weighted according to their contribution to the morbidity of the disease. The modified version of the MSSI, the FOS-MSSI, has been developed for use with the data collected in the FOS database. In addition, the renal function was analysed using an estimated glomerular filtration rate, as determined by the four-variable modification of diet in renal disease equation, and cardiac size was analysed using mean wall thickness, as assessed by echocardiography.
Data processing for statistical analysis was performed using SAS V.9.1. Data collection and analysis were supported by SHIRE Europe (Basingstoke, UK). The sponsor had no role in the interpretation of data or writing the report.
RESULTS
Patient demographics
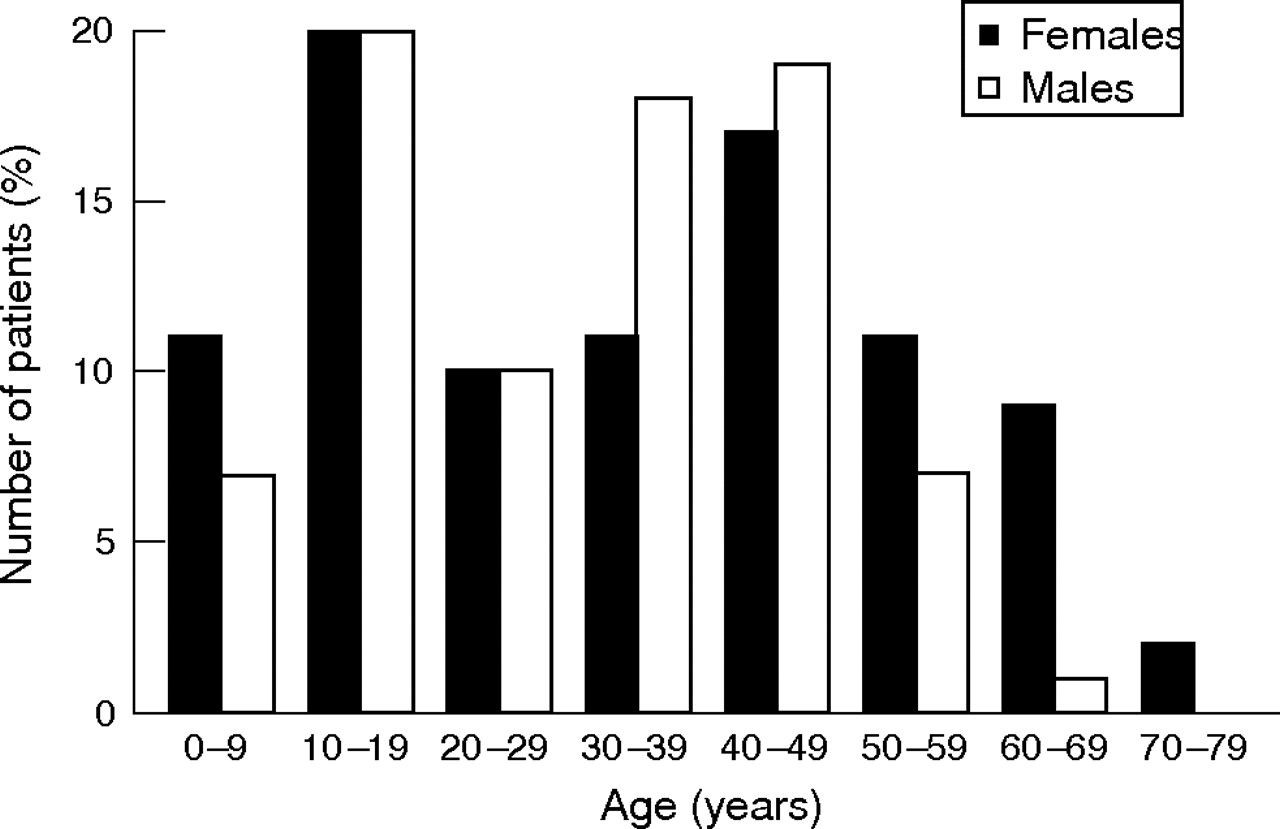
As of March 2005, there were 688 patients enrolled in the FOS. Of them, 173 (25.1%; 91 females and 82 males) underwent a complete ophthalmological examination. The patients originated from 10 European countries, with the majority from Italy (n = 33), the UK (n = 28), Spain (n = 26) and Norway (n = 23). The median age was 33.5 years (range 1.6–71.0 years; fig 1).

Age distribution of patients in the Fabry Outcome Survey who underwent a detailed ophthalmic examination (n = 173; 82 males and 91 females).
ERT with agalsidase α had already been initiated in 40 (23%) patients and had lasted for >3 months in 30 (17%) patients.
Prevalence
In some patients, conjunctival vessels showed increased tortuosity, sometimes with localised aneurysmal dilatations (fig 2A). Abnormalities in the course of vessels were often evident also in the retinovascular tree (mainly vessel tortuosity, sometimes with a typical “corkscrew” appearance), in association with arteriolar narrowing and segmental dilatation of the retinal veins (fig 2B). Corneal involvement (“cornea verticillata”) usually consisted of bilateral whorl-like opacities, located in the epithelial and subepithelial layers, more commonly in the inferior half of the cornea. These opacities were typically cream coloured, although they could range from whitish to golden brown (fig 2C). A few patients showed a typical Fabry cataract located at the level of the posterior capsule of the lens, with a “spoke-like” appearance (fig 2D). In our experience, this lens opacity is not easily detected by direct observation using the slit lamp, and is best seen using retroillumination.

Eye abnormalities associated with Fabry’s disease. (A) Conjunctival vessel tortuosity; (B) retinal vessel tortuosity; (C) cornea verticillata (vortex opacities located in the superficial corneal layers); and (D) Fabry cataract (posterior lens opacities with a radiating appearance).
The presence of cornea verticillata was reported in 76.9% of females and 73.1% of males (age range, 3–71 years), tortuous vessels in 21.9% of females and 48.7% of males (age range, 4–69 years), and Fabry cataract in 9.8% of females and 23.1% of males (age range, 5–68 years).
Of the 30 patients (9 females and 21 males; only 2 were <18 years of age) receiving ERT for >3 months, cornea verticillata was detected in 88.9% of females and 80.9% of males, tortuous vessels in 44.4% of females and 61.9% of males, and Fabry cataract in 33.3% of females and 38.1% of males. This subset of patients was too small to perform a statistical analysis.
Age-related and gender-related prevalence of eye abnormalities
The prevalence of cornea verticillata was similar in males and females, as well as in different age groups; however, the prevalence of tortuous vessels and Fabry cataract was lower among females (p<0.01 and p = 0.02, respectively), and the prevalence of tortuous vessels in males increased with age (p = 0.05). At 20 years of age, approximately 30% of males and 25% of females had tortuous vessels, and approximately 20% of males and 10% of females had Fabry cataract. The incidence after 40 years of age was approximately 60% in males and 25% in females for tortuous vessels, and >30% in males and 15% in females for Fabry cataract (fig 3).

Prevalence of cornea verticillata (CV), tortuous vessels (TV) and Fabry cataract (FC) in FOS patients (n = 173; 82 males and 91 females). Numbers per group are shown in the figure.
Local association of eye abnormalities
In all, 19 females and 32 (39%) males with cornea verticillata also had tortuous vessels, as compared with 1 female and 8 (21%) males among the patients without cornea verticillata (p = 0.03). Also, 7 females and 10 (28%) males with tortuous vessels also had Fabry cataract, as compared with 2 females and 9 (10%) males among the patients without tortuous vessels (p = 0.01). There was no overall local association seen between cornea verticillata and Fabry cataract.
Association of eye abnormalities with systemic involvement
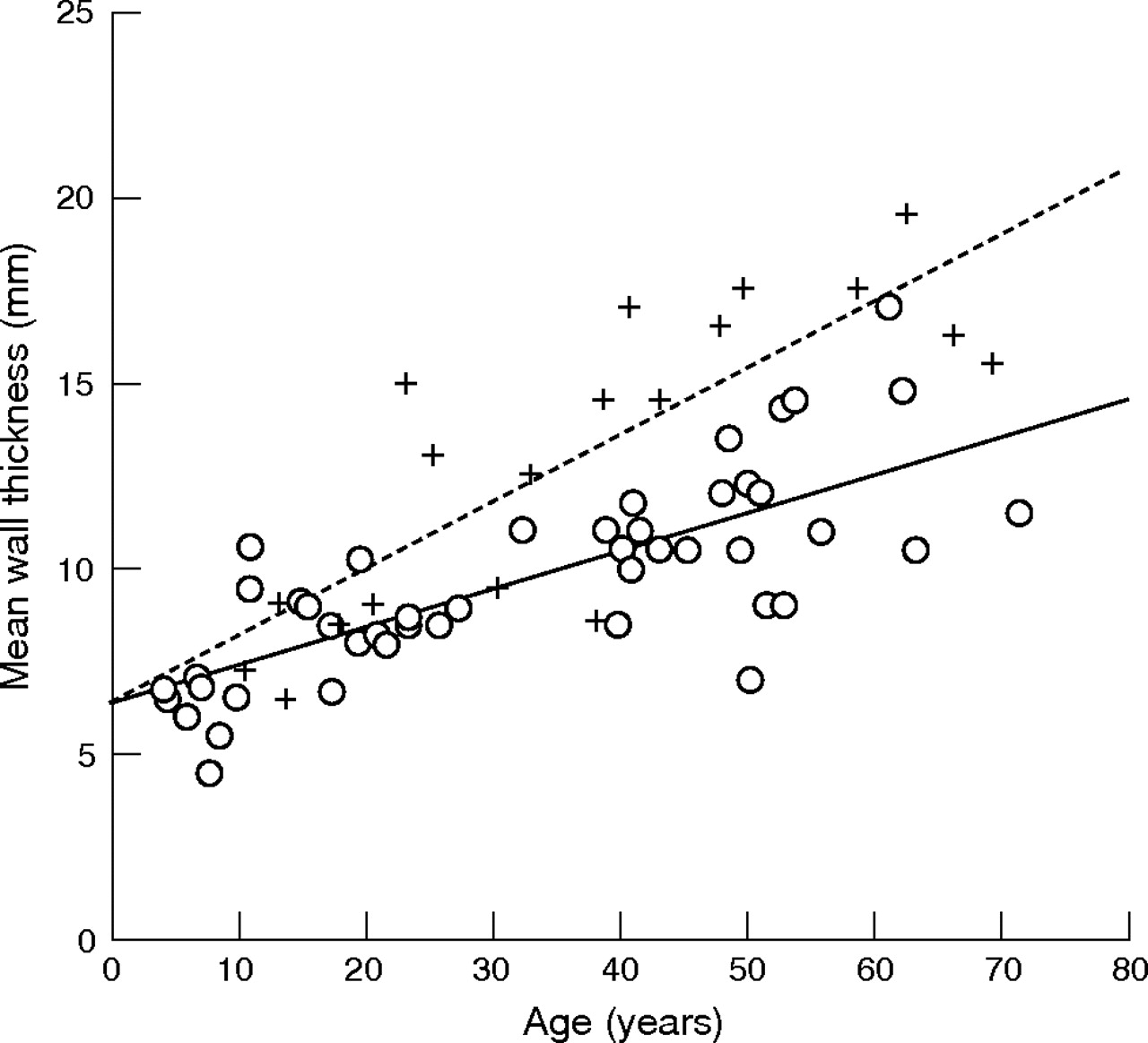
There was no relationship between the presence of cornea verticillata and the progression of Fabry’s disease (as measured using the FOS-MSSI), deterioration of renal function or increase in cardiac size. A relationship with FOS-MSSI was observed for vessel tortuosity (p = 0.01); in fact, for all age groups the FOS-MSSI was higher in the patients with vessel tortuosity than in the group of patients without this ocular manifestation (fig 4). For Fabry cataract, this pattern was the same but less significant (p = 0.12). Patients with vessel tortuosity also showed a more progressive deterioration of renal function (estimated glomerular filtration rate, p = 0.01; fig 5) and a more rapid increase in cardiac size with age (p<0.01; fig 6). The relationship between the increase in cardiac size and the prevalence of Fabry cataract was also found to be significant (p = 0.02); however, it should be noted that the number of cases with Fabry cataract in this subgroup was small.
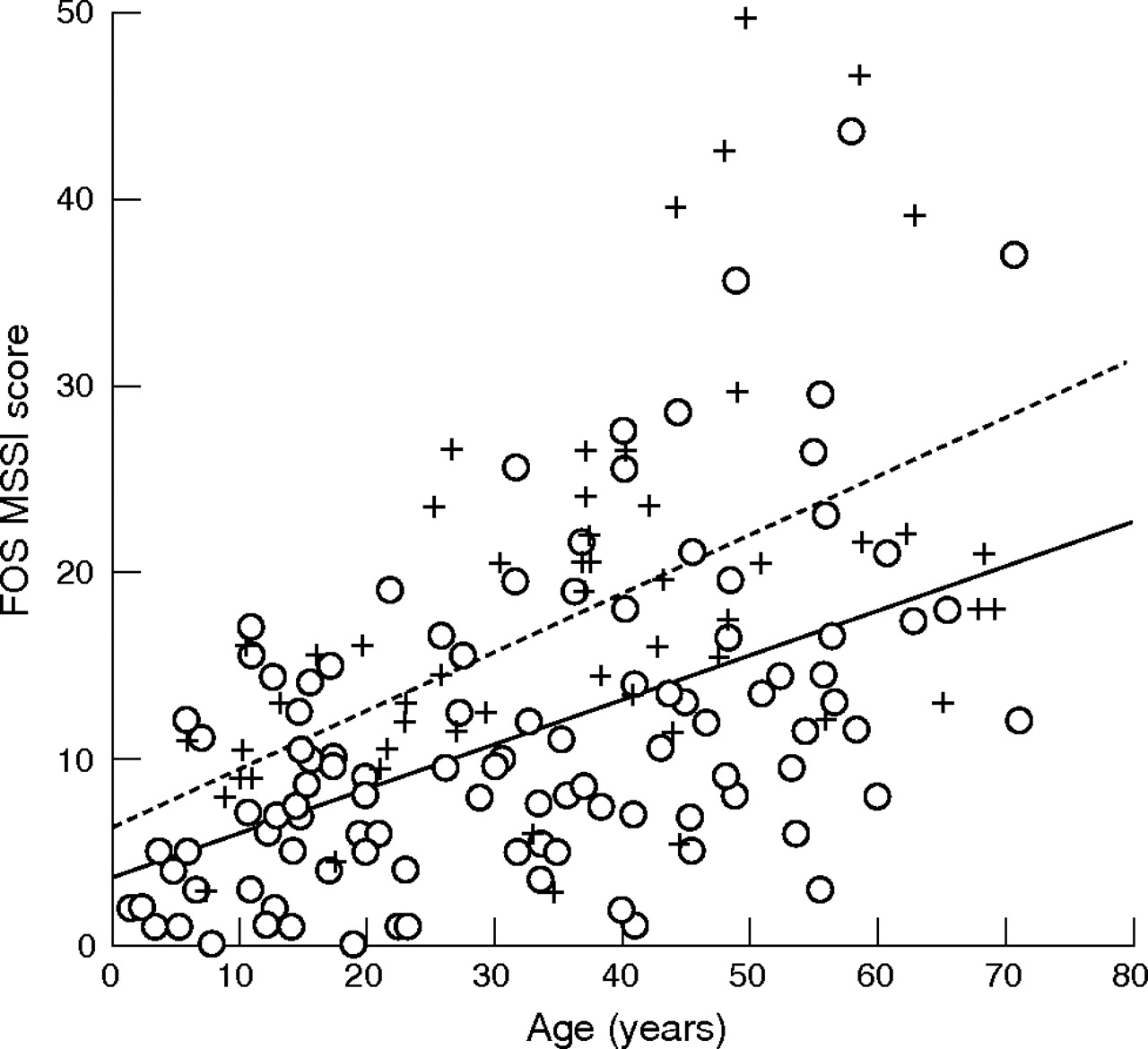
Scatter plot of the Fabry Outcome Survey Mainz Severity Score Index (FOS-MSSI) score (ie, disease severity) and age in patients in FOS with (n = 57, +/dashed line) and without (n = 107, o/solid line) tortuous vessels. For all age groups, FOS-MSSI is higher in patients with vessel tortuosity than in those without this ocular manifestation.

Scatter plot of estimated glomerular filtration rate (eGFR; a measure of renal function) and age in patients in FOS with (n = 40, +/dashed line) and without (n = 72, o/solid line) tortuous vessels. For all age groups, the eGFR is lower in patients with vessel tortuosity than in those without this ocular manifestation.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Scatter plot of mean wall thickness (a measure of cardiac size) and age in patients in FOS with (n = 19, +/dashed line) and without (n = 48, o/solid line) tortuous vessels. Mean cardiac wall thickness is higher in patients with vessel tortuosity than in those without this ocular manifestation, and the difference is more significant with increasing age.
DISCUSSION
We have presented results from the largest study of ophthalmological abnormalities in patients with Fabry’s disease, comprising data from 173 patients from FOS.
About 75% of the patients enrolled in FOS could not be included in the study because they could not undergo the eye examination, or the ophthalmological data were incomplete. However, their demographic features were similar to the 173 patients examined, and we believe that the conclusions made can be applied to the whole group of patients in FOS.
In our series, cornea verticillata was observed in most hemizygotic male and heterozygotic female patients. Vessel tortuosity and Fabry cataract were observed in fewer patients, with a higher prevalence in males. These data are in agreement with other reported series.6,7,8,9,10,11,12 The observed lower prevalence of cornea verticillata in this series is explained by the age and sex distribution; in fact, most patients were females and 58 (33%) were aged <20 years. Furthermore, there is the potential effect of treatment, as 17% of patients had been receiving ERT for >3 months at the time of data collection. Patients were seen at participating centres throughout Europe; so there is potential interobserver variation in the evaluation of ocular signs.
Cornea verticillata is very rare in individuals without Fabry’s disease (its differential diagnosis includes use of specific drugs such as amiodarone or chloroquine). The positive finding of cornea verticillata therefore represents a test with high sensitivity and specificity for the diagnosis of Fabry’s disease. However, cornea verticillata and other ophthalmological manifestations of Fabry’s disease do not result in visual symptoms, and so do not increase the referral of patients to an ophthalmologist. Moreover, ophthalmologic screening programmes for ocular manifestations typical of Fabry’s disease have not been particularly successful.22
The prevalence of vessel tortuosity in patients in FOS is lower than expected, in comparison with previous reports on smaller series.6,7,8,9,10,11,12 This discrepancy may be due to the age and sex distribution and the possible effect of ERT in the treated patients.
Tortuous vessels and Fabry cataract were more prevalent in males than in females. This may be due to the earlier clinical manifestations of the disease in hemizygotic males, or to some other unknown effects, such as hormonal influences on ocular blood flow dynamics.23,24
We detected ocular manifestations of Fabry’s disease in young children; the youngest child was 3 years old. This is in agreement with previous reports of the very early presence of cornea verticillata,25 even in a 6-month-old child6 and a fetus,26 and highlights the need for performing an ophthalmic examination in paediatric patients.
Moreover, the probable early appearance of cornea verticillata in the natural history of Fabry’s disease supports the clinical value of the ophthalmological examination in those patients in whom Fabry’s disease is suspected, but not diagnosed at a genetic or biochemical level; in those cases, a positive report of cornea verticillata can be suggestive for the diagnosis in the interim period before laboratory confirmation.
Cornea verticillata may be an isolated finding in patients with Fabry’s disease without other eye abnormalities; hence, it is the most reliable ocular marker of the disease. Furthermore, the presence of cornea verticillata did not show a positive predictive value for disease severity. This is in agreement with a recent report of a much smaller series of 10 patients with Fabry’s disease, which found no clear relationship between ocular abnormalities and the systemic, cardiac and renal manifestations of the disease.11
In contrast, vessel tortuosity is very rarely present as the only ocular sign in patients with Fabry’s disease and shows an association with both cornea verticillata and Fabry cataract; hence, the isolated presence of tortuous vessels (especially in the fundus), without any corneal or lens involvement, is not diagnostic for Fabry’s disease.
Furthermore, we found that increased vessel tortuosity seems to be associated with more severe systemic involvement, with a more rapid increase in the FOS-MSSI score with age and changes in indices of cardiac and renal function.
In Fabry’s disease, the disruption of vascular architecture is due to substrate accumulation within the vessel walls, resulting in vascular impairment due to endothelial cell dysfunction, abnormal blood flow and hypercoagulability. Hence conjunctival and retinal vessel abnormalities may represent a clinically significant marker of a diffuse microvascular disorder leading to end-organ pathology throughout the body.27
The data also suggest a positive predictive value in performing regular eye examinations (particularly focusing on vessel tortuosity) in patients with systemic involvement.
CONCLUSION
Data from FOS represent the largest study of ophthalmological abnormalities in patients with Fabry’s disease. The data indicate that cornea verticillata is the most frequently reported eye abnormality in both hemizygotic males and heterozygotic females with Fabry’s disease, and, at present, can be considered the most significant ophthalmological marker for the diagnosis of Fabry’s disease. In contrast, vessel tortuosity is not useful in the diagnosis of Fabry’s disease, although it is potentially a marker of systemic progression of the disease.
These results support the role of the ophthalmological examination as a useful tool for early diagnosis and for monitoring disease progression in Fabry’s disease.
Technological advances may improve the evaluation of the ocular signs, providing measurable and reproducible parameters. The candidate technologies include digital analysis of the retinal vessels and the study of possible subclinical alterations of the optic pathways by means of computerised perimetry and electrophysiological tests.
REFERENCES
Footnotes
-
Published Online First 13 September 2006
-
Funding: Data collection and analysis were supported by TKT Europe.
-
Competing interests: None.