Article Text

Abstract
Neuroendocrine cell hyperplasia of infancy (NEHI) has recently been described as an obstructive airway disease that affects infants aged 1–24 months, and presents typically with tachypnoea, crackles and hypoxia. The pathogenesis of the disease is unknown. We describe the clinical course of nine infants with radiologically and histologically confirmed NEHI. Host or environmental factors were not associated with the disease development. All infants with lung function tests demonstrated findings consistent with severe irreversible peripheral airway obstruction, assessed with whole body plethysmography (6/6) or the rapid thoracoabdominal compression technique (5/5). While the symptoms abated in all infants, six infants developed a non-atopic asthma during the follow-up. Systemic or inhaled corticosteroid treatment did not affect the duration of the symptoms. NEHI may mimic severe asthma and thus this entity should be taken into account when evaluating infants with chronic respiratory symptoms.
Statistics from Altmetric.com
Introduction
Neuroendocrine cell hyperplasia of infancy (NEHI) has been recently described as a pulmonary disorder that affects infants aged 1–24 months.1 The previous name of the disease was ‘persistent tachypnoea of infancy’ and describes how NEHI presents typically with tachypnoea, retractions, crackles and occasionally hypoxia.2 Although the pathogenesis of the disease is unknown, the pulmonary pathology is characterised by abundant neuroendocrine cells in an otherwise structurally normal lung—hence the new name for the disease.3 High resolution CT shows patchy, ground-glass opacities and air-trapping.3 A recent study reported that lung function tests are compatible with an obstructive airway disease that does not, however, respond to treatment with glucocorticosteroids or bronchodilators.3 Since NEHI occurs in siblings, a genetic susceptibility has been proposed.4 Exposure to microbial infections or environmental toxins has not been associated with the disease. To further describe the clinical picture and to evaluate host- and environment-related risk factors of NEHI, we reviewed the clinical findings of nine infants with NEHI treated in our hospitals in 2003–2008.
Case reports
Infants participated in a follow-up study of interstitial lung diseases in 2003–2008. Their parents filled in a questionnaire on environmental factors, host factors and initial symptoms. The infants were prospectively followed, and the parents filled in a repeat questionnaire on symptoms and medications at the end of the follow-up. The study was approved by the local Ethics Committee.
All infants were full term and the pregnancies had been uneventful. There was no evidence of infection, maternal smoking or use of antidepressant or other medication during pregnancy. There was no history of neonatal complications. Most of the infants were boys (6/9) (table 1). There was no family history of significant pulmonary diseases, except in one family where two siblings had similar symptoms (patients 4 and 6). The family history with regard to asthma, parental sensitisation, day care or household pets did not differ from the general population. None of the infants lived in high altitude (table 1).
Demographics of infants with neuroendocrine cell hyperplasia of infancy
Symptoms
The initial symptom in all cases was tachypnoea (>60/min), usually before age 6 months (table 2). Chronic cough, recurrent wheezing or persistent hypoxia (pulse oximeter O2 saturation <95% at rest and breathing room air) occurred in three of nine infants, and crackles were heard on auscultation of four infants (table 2). Eight of nine infants failed to thrive. None of the infants had evidence of preceding viral infection and viruses tested by PCR from nasopharyngeal samples or lung biopsy specimen (patient 9) were negative for adenovirus, coronaviruses (strains OC43 and 229), enteroviruses, human metapneumovirus, influenza A and B viruses, parainfluenza type 1, 2 and 3 viruses, rhinovirus and respiratory syncytial virus (RSV). However, the lung biopsy specimens of infants 4 and 9 were positive for the Epstein–Barr virus by PCR and for Epstein–Barr virus-encoded RNA (EBER) by in situ hybridisation, respectively. The EBER was located exclusively in peribronchial lymphocytes. All other infants were EBER negative.
Patient characteristics of infants with neuroendocrine cell hyperplasia of infancy (NEHI)
Patient investigations
On admission to the hospital the infants were evaluated for other than respiratory causes of tachypnoea, but nothing of note was found. All had a normal cardiac sonography and none had evidence of pulmonary hypertension. Chest radiography was nearly normal in all cases, except for slight overinflation of the lungs with some interstitial markings in two children (figure 1D). Full inspiratory (1/10 mm slices) and expiratory (3–6 slices) images of the chest taken during sedation with high resolution CT demonstrated ground-glass opacities (figure 1E) and these occurred in all infants (table 2). The changes were typically located in the lingula and the right middle lobe. Interestingly, in all infants who underwent the test (6/6), whole body plethysmography5 demonstrated increased functional residual capacity (FRC, z-score >2.0) suggesting hyperinflation, and severely decreased specific airway conductance (sGaw, z-score <−3.0) with characteristic pressure flow tracings compatible with peripheral airway obstruction.6 None improved significantly (change in sGaw >30%) after inhalation of salbutamol.7 In five infants, maximal expiratory flows at FRC (VmaxFRC) were assessed with the tidal thoracoabdominal compression technique:8 they all had significantly reduced VmaxFRC (z-score <−2).9 Because of pulmonary symptoms, radiological findings and growth failure, all patients underwent lung biopsy at a median of 5 months (range 0–9 months) after symptom onset (table 2).

{kind=link}
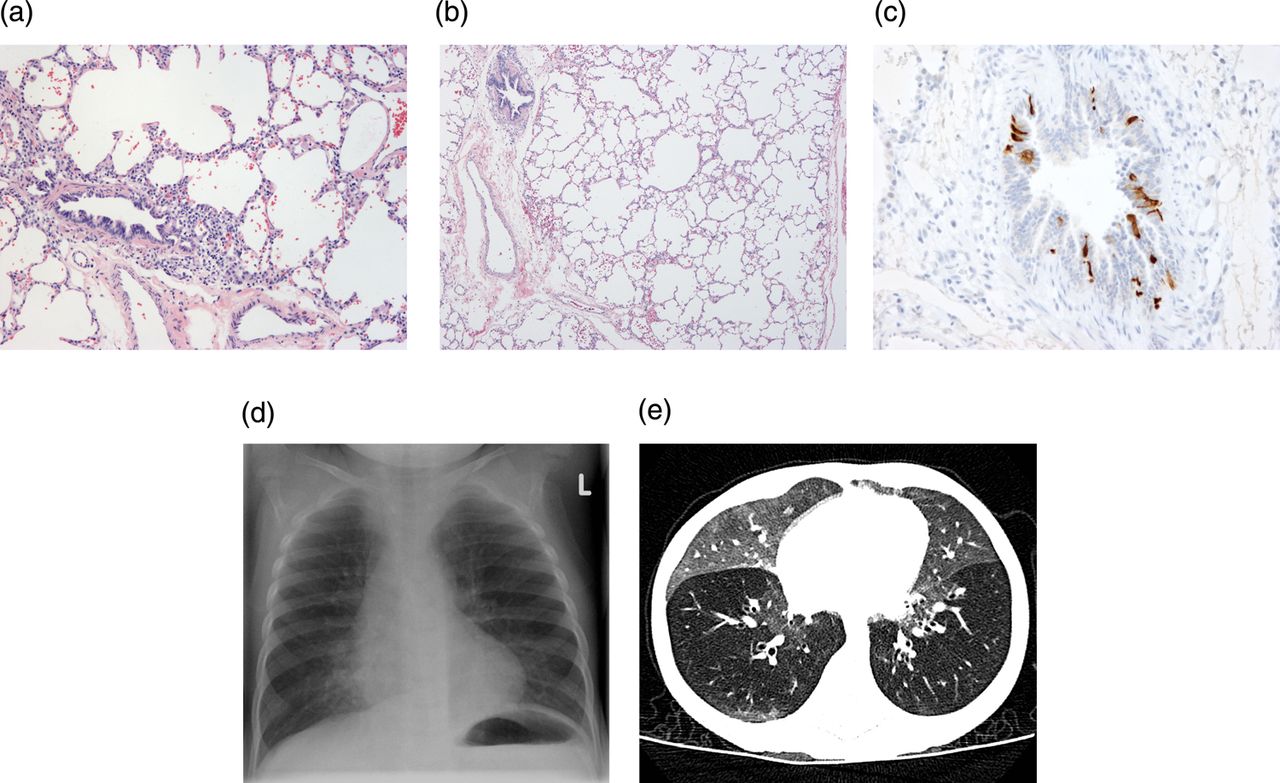
Lung histology and radiological findings in neuroendocrine cell hyperplasia of infancy. H&E-staining demonstrated distension of distal airspaces and minor peribronchial accumulation of lymphocytes in lung biopsy specimen (A, B), magnification ×100 and ×10, respectively. Bombesin-staining showed an increased number of neuroendocrine cells within a bronchiole (C), magnification ×200. Chest radiography demonstrated interstitial markings in both lungs (D) and ground-glass opacities were seen in both lungs on high resolution CT (E).
Lung biopsy findings
Lung histology demonstrated normal alveolar structure without any significant fibrosis. Slightly enlarged peribronchial lymphocyte aggregates were seen in some cases (figure 1A,B), but there was no inflammatory cell accumulation in the alveolar walls or airspaces. A typical finding was hyperinflated airspaces in subpleural area suggesting air trapping (figure 1A,B). Immunohistochemistry showed a significant number of bombesin-positive cells in the walls of small airways, compatible with neuroendocrine cells (figure 1C). Ki-67/PCNA-staining demonstrated few positive cells in the lung parenchyma, epithelium and endothelium demonstrating normal rate of proliferation in these lungs. NEHI was set as the diagnosis on the basis of a nearly normal lung histology, increased number of bombesin-positive cells, characteristic radiological findings and clinical symptoms.1 ,3
Treatment and outcome
All infants were treated with oral prednisolone at a starting dose of 2–3 mg/kg daily for 1–2 weeks followed by a decreasing dosing over several weeks (median 14 weeks; range 2–184 weeks). There was no association between improvement of clinical symptoms or pulmonary function tests and duration or dose of glucocorticoid therapy during follow-up (table 2). Most of the infants received also inhaled corticosteroid treatment, but this treatment had no effect on symptoms. None of the infants benefited from inhaled salbutamol. The median duration of the symptoms was 18 months (range 6–60 months) and the tachypnoea abated in all infants during the follow-up. However, 6 of the 9 infants developed a non-atopic asthma that persisted throughout follow-up (table 2). In contrast to the symptoms in early childhood, two patients (2/2 investigated children) treated in our hospital had a positive bronchodilator response in spirometry and/or >15% decrease in the FEV1 in the free running test. None of the infants with asthma had significant sensitisation at the time of last contact. Half of the patients with asthma (3/6) had combined therapy with inhaled corticosteroid and long-acting β-agonist.
Discussion
Our observations suggest that NEHI is an obstructive airway disease of infancy as also recently reported by Young et al.3 Although the prevalence of NEHI is unknown, milder forms of the disease may be far more common than acknowledged, since only the most severe cases undergo extensive examinations. The pathogenesis of the disease is unknown, but the hypothesis is that the symptoms could be caused by overactive pulmonary neuroendocrine cells that produce bioactive peptides like serotonin which is a well known bronchiolar constrictor. Other bioactive peptides that have vasoactive properties and may control inflammation and regulate ventilation10 include bombesin-like peptides, gastrin releasing peptide, calcitonin gene-related peptide, cholecystokinin, vasoactive intestinal peptide and substance P. Accordingly, pulmonary neuroendocrine cells are preferentially located in neuroepithelial bodies, specialised oxygen-sensing chemoreceptors of the airways that control the respiratory rate and alveolar ventilation through neural pathways.10
Studies characterising the lung function changes in NEHI are so far few. In those infants who underwent lung function testing, we could assess findings in whole body plethysmography and maximal expiratory flows that were compatible with severe airway obstruction and hyperinflation. These observations are in agreement with Young et al3 who applied raised volume thoracoabdominal technique in some of their subjects. Hyperinflation is also a characteristic radiological finding in NEHI.11
Systemic or inhaled glucocorticosteroid treatment was not associated with the clinical course of the disease in our patients, as has been the case for other patients.12 Thus, our observations do not support routine use of systemic glucocorticosteroids to treat NEHI. NEHI seems to improve usually within 1–2 years and almost all infants described in the literature have had a favourable outcome. Consequently, it has been suggested that lung biopsy is no longer needed to diagnose NEHI.11 Infants with suspected NEHI who follow healthy growth curves and who do not need supplemental oxygen may certainly be followed-up without lung biopsy, but we feel that infants with poor weight gain and oxygen dependency should still undergo lung biopsy to exclude other, more severe interstitial lung diseases. If the lung biopsy supports a diagnosis of NEHI, this implies a good prognosis, which will reduce anxiety in the family.
We did not find any association between environmental or host factors and disease development. Since none of the infants were symptomatic during their first weeks of life, NEHI does not seem to be congenital, although there probably is some genetic susceptibility, since a similar disease has been described in siblings.4 Also among our nine patients, two were siblings. While the pathogenesis of NEHI remains to be solved, the clinical picture of the disease has become clearer. Although wheezing is not a major symptom of NEHI, bronchial obstruction is typical and this specific constellation should be considered in the differential diagnosis by all paediatricians when evaluating children with chronic obstructive airway disease.
References
Footnotes
-
Contributors All authors have significantly contributed to the study.
-
Funding None.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval The Ethics Committee of the Helsinki and Uusimaa Hospital District.
-
Provenance and peer review Not commissioned; externally peer reviewed.