Article Text

Abstract
Objective To report the oral corticosteroid-sparing effect of omalizumab in children with severe asthma.
Design 16-week therapeutic trial.
Setting Tertiary paediatric asthma clinic.
Patients 34 children with severe asthma maintained on oral prednisolone (median age 12 years; 15 children <12 years and 19 children ≥12 years).
Interventions Fortnightly or monthly subcutaneous injections of omalizumab; the dose was calculated as per manufacturer's instructions based on body weight and serum immunoglobulin E concentration.
Main outcome measures Reduction in prednisolone dose; mini-Asthma Quality of Life Questionnaire (AQLQ); Childhood Asthma Control Test (ACT); forced expiratory volume in 1 s (FEV1).
Results Median daily prednisolone dose reduced from 20 mg to 5 mg (n=34, p<0.0001), including seven children who stopped prednisolone completely. Mini-AQLQ score increased from 3.5 to 5.9 (n=24, p<0.0001). Childhood ACT score increased from 12 to 20 (n=23, p=0.0001). FEV1 increased from 2.10 to 2.25 litres (n=31, non-significant). The reduction in prednisolone dose and improvements in mini-AQLQ and childhood ACT were significant in children both under and over 12 years of age, with no differences in outcome detected between these two groups.
Conclusions A 16-week therapeutic trial of omalizumab allowed a significant reduction in daily prednisolone dose and was associated with improvements in asthma control and quality of life in 34 children with severe asthma. Similar benefits were seen in children both above and below 12 years of age. These uncontrolled data are very encouraging. There is an urgent requirement for a multicentre randomised placebo-controlled trial of omalizumab in children with severe asthma, with reduction in oral corticosteroid dose as the primary outcome measure.
Statistics from Altmetric.com
Introduction
Asthma is the most common chronic disease of childhood in developed countries.1 The majority of asthmatic children respond well to appropriate guideline-based treatment such as that outlined by the British Thoracic Society and Scottish Intercollegiate Guidelines Network (BTS/SIGN).2 Children with symptoms that do not respond adequately to treatment should be referred to specialist paediatric respiratory services for further investigation and management.3 ,4 Following critical re-examination of the diagnosis and addressing of the basics of asthma management, including a nurse-led home visit, a group of children remain who have genuinely severe disease that does not respond to standard approaches.5,–,7 Many such children require maintenance treatment with oral corticosteroids, which is associated with considerable adverse effects.8 ,9
What is already known on this topic
▶ Despite many impressive anecdotal success stories and increasing clinical use, evidence is sparse for omalizumab in children with genuinely severe asthma maintained on oral corticosteroids.
▶ Studies to date have largely included children with mild to moderate disease in North American healthcare settings.
▶ NICE guidance issued in October 2010 does not recommend the use of omalizumab in children under 12 years of age.
What this study adds
▶ A 16-week therapeutic trial of omalizumab was associated with a significant reduction in prednisolone dose and improvements in asthma control and quality of life in children with severe asthma.
▶ Benefits were found in children both above and below 12 years of age.
Deaths in children from asthma are now thankfully unusual in most countries, but the condition is still associated with considerable morbidity.1 ,3 ,10 In severe asthma this is reflected in hospital admissions, frequent outpatient attendances, time off school and impaired quality of life for both the patient and close family members.1 ,11 In the longer term severe asthma in childhood may lead to the development of irreversible airways obstruction, impact on educational attainment and influence career choice.12
Omalizumab is a monoclonal anti-immunoglobulin E (IgE) antibody that has emerged as a therapeutic option in IgE-mediated asthma.13 ,14 The majority of patients included in published studies have been adults.14 But there is evidence of efficacy in children aged 6–12 years from two randomised placebo-controlled trials that reported reduction in inhaled corticosteroid dose,15 and decreased exacerbation rate,16 respectively. Improved symptom control was also demonstrated in a recent study in which the mean age of participants was 11 years.17 Most children in these studies had disease of only moderate severity.
Guidance issued in October 2010 by the National Institute for Health and Clinical Excellence (NICE) recommended that the use of omalizumab be restricted to those over 12 years of age due to a lack of evidence of efficacy and cost-effectiveness in younger children.18 This decision has generated considerable controversy and has raised several important issues.7 Conversely the Scottish Medicines Consortium and a panel of independent European specialists in paediatric respiratory medicine recommend a 16-week therapeutic trial in children prescribed chronic systemic corticosteroids in whom all other standard treatments have failed.8 ,19
In this paper we report the oral corticosteroid-sparing effect of a 16-week therapeutic trial of omalizumab in 34 children with severe asthma requiring maintenance oral corticosteroids, along with asthma control and quality of life data.
Methods
Study design and participants
All children were thoroughly assessed and investigated in a tertiary paediatric respiratory clinic to confirm the diagnosis of severe asthma. Investigations included flexible bronchoscopy, high-resolution CT scanning and a basic screen of immune function where clinically indicated. A nurse-led home visit was performed to assess inhaler technique, improve patient education, maximise concordance with treatment and address any obvious environmental factors including avoidable exposure to allergens and tobacco smoke. Concordance with treatment was also assessed by checking with general practitioners on the uptake of repeat prescriptions for asthma medication.20 The protocol used prior to commencing omalizumab is provided in online Appendix 1.
Children were managed according to the stepwise approach of the BTS/SIGN guidelines; all required maintenance treatment with oral prednisolone (step 5) prior to the therapeutic trial of omalizumab.2 All patients considered for a trial of omalizumab had required prednisolone for a minimum of 3 months. Prior to commencing the trial a formal assessment was made to determine the minimum maintenance dose required in each patient by a stepwise reduction over several weeks until clinical deterioration and/or reduced lung function occurred.
A total of 34 consecutive children completed a 16-week therapeutic trial of omalizumab. The median age was 12 years (range 5–16 years), with 15 children aged <12 years and 19 aged ≥12 years. Omalizumab was administered monthly or fortnightly subcutaneously by nursing staff in a dedicated clinic according to the manufacturer's instructions, with the dose based on serum IgE and body weight.21
The median serum IgE level at the commencement of treatment was 411 IU/ml (range 119–1193 IU/ml), which was comparable in the subgroups of children aged <12 and ≥12 years at 429 and 365 IU/ml, respectively (p=1.0, Mann–Whitney test).
The daily dose of prednisolone was recorded at the commencement and conclusion of the therapeutic trial. Where a child was prescribed a different dose of prednisolone on alternate days, the median daily dose was recorded. Children were followed up at a minimum of 4-weekly intervals. Prednisolone dose was altered at each clinic visit at the judgement of a consultant respiratory paediatrician, based on overall clinical status and lung function measurements. Other antiasthma therapies were not altered during the trial.
Each pragmatic therapeutic trial was performed as part of routine clinical management and therefore this work did not require ethical approval.
Lung function measurement
Forced expiratory volume in 1 s (FEV1) was measured according to American Thoracic Society guidelines in children who were able to reliably perform spirometry.22
Questionnaire assessment of quality of life and asthma control
The mini-Asthma Quality of Life Questionnaire (AQLQ) and Childhood Asthma Control Test (ACT) were administered where possible prior to commencement and at the conclusion of each therapeutic trial.23 ,24 Possible mini-AQLQ scores range from 1 to 7, with a higher score indicative of a better quality of life.23 A change of >0.5 has been established as being clinically significant in adults.25 The childhood ACT ranges from 0 to 27 for children under 12 years and from 5 to 25 in children aged 12 years or over. A higher score represents greater asthma control.24 In adults a change of ≥3 in the ACT has been demonstrated to be clinically significant.26
Statistical analysis
The Wilcoxon matched pairs test was used to compare the results before and after the therapeutic trial. A p value <0.05 was considered significant and the Holm–Bonferroni method was used where multiple comparisons were performed.27 Prism 5 for Mac Os X (GraphPad Software, La Jolla, California, USA) was used to perform the analyses.
Results
Oral corticosteroid dose
There was a significant reduction in daily prednisolone dose during the 16-week therapeutic trials from a median of 20 mg (range 2.5–50 mg) to 5 mg (range 0–40 mg) (p<0.0001; figure 1A). In 29 children (85%) the prednisolone dose was reduced, with a median drop of 15 mg (range 2–40 mg); in one child the dose stayed the same. A total of seven children stopped maintenance prednisolone completely.

(A) Change in prednisolone dose in all children. Each symbol represents an individual child (n=34). The horizontal lines represent the median prednisolone dose. (B) Change in prednisolone dose in children under 12 years of age. Each line represents an individual child (n=15). (C) Change in prednisolone dose in children aged 12 years or over. Each line represents an individual child (n=19).
Subgroup analysis of children aged <12 and ≥12 years showed a significant reduction in prednisolone dose in both groups. In children aged <12 years the median prednisolone dose fell from 20 mg (range 5–50 mg) to 5 mg (0–40 mg) (p<0.0001; figure 1B). In those aged ≥12 years it fell from 10 mg (2.5–40 mg) to 5 mg (0–20 mg) (p=0.0054; figure 1C).
Quality of life
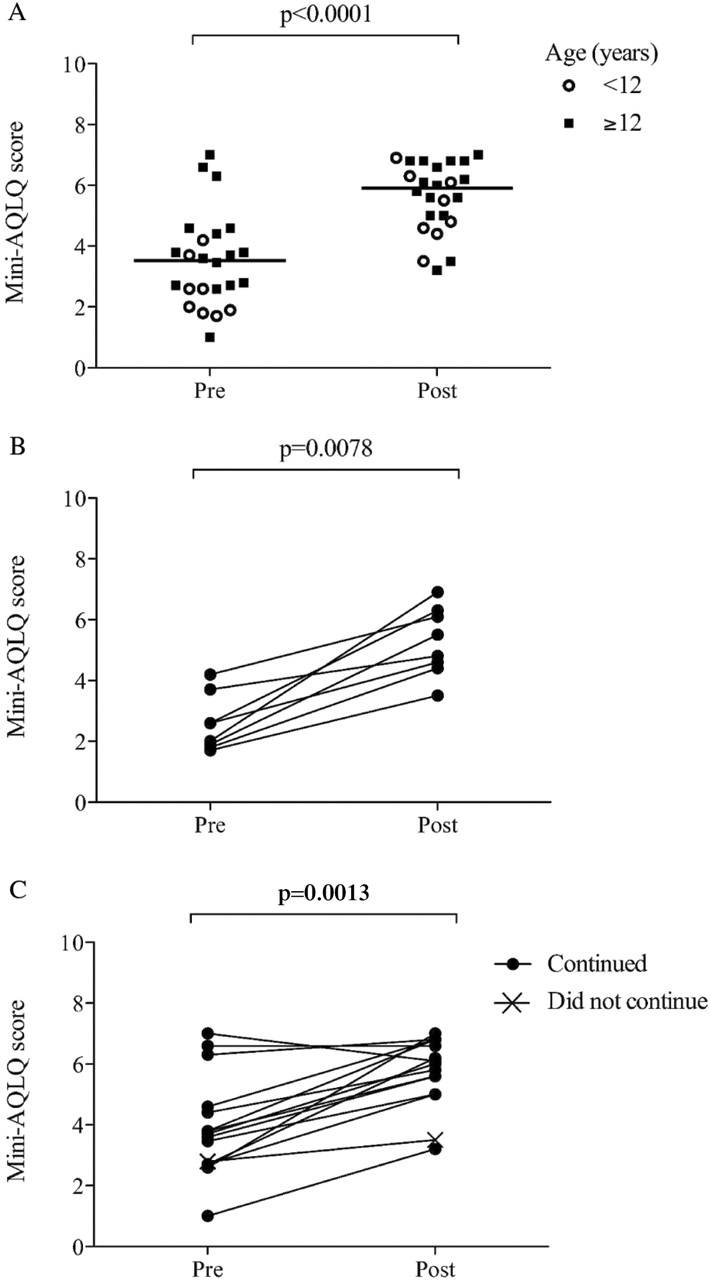
A total of 24 children satisfactorily completed mini-AQLQ questionnaires at both commencement and conclusion of the therapeutic trial. The median score increased significantly during the trial from 3.5 (range 1–8.4) to 5.9 (3.2–9.9) (p<0.0001; figure 2A). The mini-AQLQ score increased in 22/24 children (92%).

(A) Change in mini-Asthma Quality of Life Questionnaire (AQLQ) scores in all children. Each symbol represents an individual child; complete data were available for 24 children. The horizontal lines represent the median. (B) Change in mini-AQLQ scores in children under 12 years of age. Each line represents an individual child; complete data were available for eight children (all continued on omalizumab). (C) Change in mini-AQLQ scores in children aged 12 years or over. Each line represents an individual child; complete data were available for 16 children.
Subgroup analysis of children aged <12 and ≥12 years showed a significant increase in mini-AQLQ scores in both groups. In children aged <12 years the median mini-AQLQ score increased from 2.3 (range 1.7–4.2) to 5.2 (3.5–6.9) (p=0.0078; figure 2B). In children aged ≥12 years it increased from 3.8 (1–8.4) to 6.1 (3.2–9.9) (p=0.0013; figure 2C).
Asthma control
The childhood ACT was completed satisfactorily by 23 children at both commencement and conclusion of the therapeutic trial. There was a significant increase during the trial from a median score of 12 (range 6–24) to 20 (12–26) (p=0.0001; figure 3A). The childhood ACT increased during the trial in 21/23 children (91%).
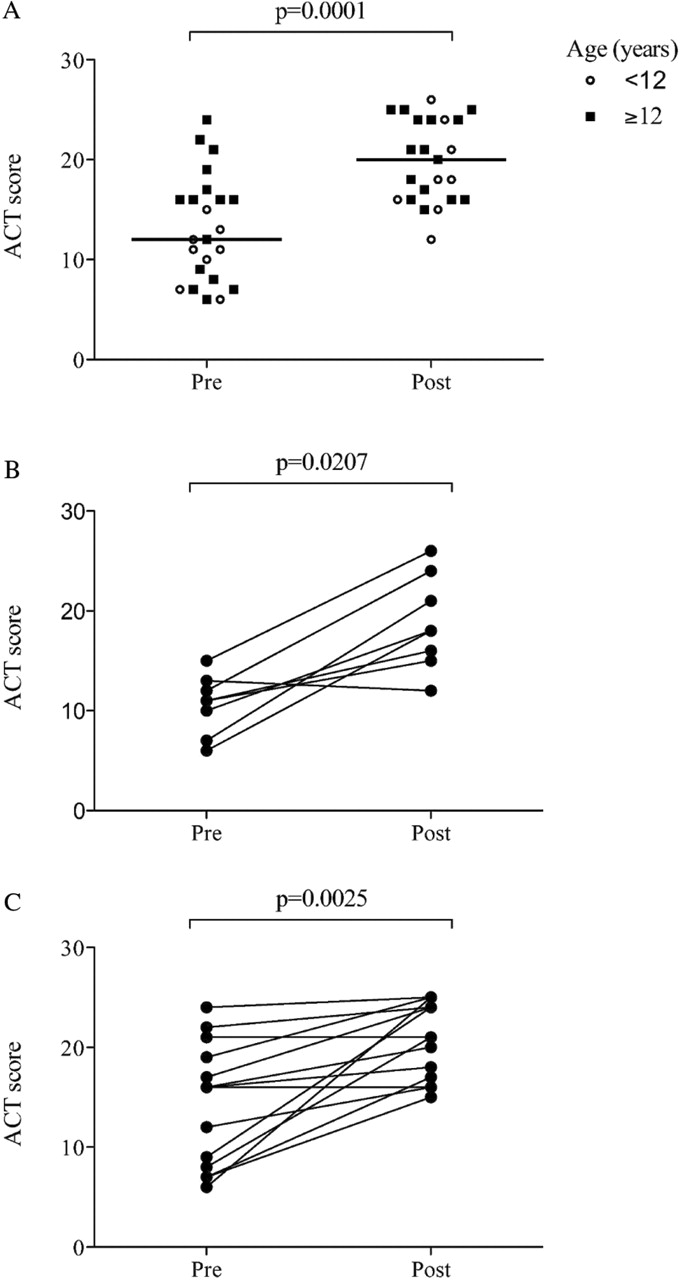
(A) Change in asthma control test (ACT) scores in all children. Each symbol represents an individual child; complete data were available for 23 children. The horizontal lines represent the median. (B) Change in ACT scores in children under 12 years of age. Each line represents an individual child; complete data were available for eight children (all continued on omalizumab). (C) Change in ACT scores in children aged 12 years or over. Each line represents an individual child; complete data were available for 15 children (all continued on omalizumab).
Subgroup analysis of children aged <12 and ≥12 years showed a significant increase in childhood ACT scores in both groups. In children aged <12 years, median childhood ACT increased from 11 (range 6–15) to 18 (12–26) (p=0.00207; figure 3B). In children aged ≥12 years it increased from 16 (6–24) to 21 (15–25) (p=0.0025; figure 3C).
Lung function
Complete data for FEV1 at both commencement and conclusion of the therapeutic trial was available in 31 children (figure 4A). There was an increase in median FEV1 from 2.10 to 2.25 litres that was not statistically significant (p=0.1). In 26/31 children (83%), FEV1 increased during the trial. In children aged <12 years, median FEV1 increased from 1.80 to 2.10 litres (n=13, p=0.0058; figure 4B), and in those aged ≥12 years, from 2.31 to 2.48 litres (n=18, p=0.052; figure 4C).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) Change in forced expiratory volume in 1 s (FEV1) in all children. Each symbol represents an individual child; complete data were available for 31 children. The horizontal lines represent the median. (B) Change in FEV1 in children under 12 years of age. Each line represents an individual child; complete data were available for 13 children. (C) Change in FEV1 in children aged 12 years or over. Each line represents an individual child; complete data were available for 18 children.
Tolerance of omalizumab and long-term outcome following therapeutic trial
All children completed the 16-week trial. Omalizumab was generally well tolerated and no major adverse effects were reported. Following the trial, 30 children (88%) continued on omalizumab. In four children omalizumab was discontinued due to lack of apparent benefit in terms of prednisolone dose, lung function and overall clinical status.
Discussion
A 16-week therapeutic trial of omalizumab in 34 consecutive children with severe asthma allowed a significant reduction in daily prednisolone dose and improved asthma control and quality of life in more than 90% of children. There was also a small, but statistically non-significant, increase in FEV1 despite the decrease in prednisolone dose.
An obvious limitation of this work is that the therapeutic trials were uncontrolled, but these data represent an important contribution to the extremely sparse literature regarding the steroid-sparing effects of omalizumab in children with genuinely severe asthma. The published randomised controlled trials of omalizumab in children were performed in North American healthcare settings and the vast majority of the children enrolled had moderate asthma.15,–,17 For example, in the recent Lanier study only 2% of children were maintained on oral corticosteroids.16 Outcomes have included reduction in inhaled corticosteroid dose,15 exacerbation rate16 and asthma symptoms.17 This contrasts starkly with clinical practice in Europe where there is an urgent requirement for an agent to reduce the burden of oral corticosteroids in children with severe disease.7
The adverse effects of long-term oral corticosteroids in children are substantial. Covar et al reported a series of 163 children with severe asthma who received an average of six rescue courses of prednisolone per year; half of them were maintained on oral corticosteroids.9 They found a high prevalence of steroid toxicity including hypertension (80%), cushingoid features (66%), adrenal suppression (39%), myopathy (50%), growth suppression (39%), obesity and hypercholesterolaemia (30%), osteopenia (46%) and cataracts (14%).9 In the 29 children in our series that reduced their prednisolone dose during the trial, there was a median drop of 15 mg; seven children stopped maintenance prednisolone completely. The decision was made to change prednisolone dose based on objective lung function data and overall assessment of current clinical status by a consultant respiratory paediatrician.
A placebo effect associated with the introduction of a new treatment is well recognised in children with severe asthma. For example, in a double blind placebo-controlled study of nebulised budesonide in preschool children with severe asthma, children randomised to placebo reduced their prednisolone requirement by 41%.28 Although it is plausible that there was a degree of placebo effect during the therapeutic trials of omalizumab reported in this paper, the 75% median drop in prednisolone dose is likely to be clinically significant.
Fifteen children (44%) were aged under 12 years; there was also a significant reduction in prednisolone dose in this age group, along with improvements in asthma control and quality of life where measured. These findings are pertinent because omalizumab is not recommended for children aged 6–11 years in England and Wales in the most recent guidance issued by NICE.18 This decision has generated controversy and frustration because several expert clinicians have anecdotally experienced seeing younger children who have benefited greatly from omalizumab treatment.7 ,18 Our uncontrolled data are therefore particularly important in this age group. Furthermore, there is an increasing acceptance of the view that a more diverse approach embracing the totality of clinical evidence, including non-randomised uncontrolled data, may be appropriate when considering interventions in rare conditions, such as children with genuinely severe asthma.29
In keeping with the published literature, omalizumab treatment was generally well tolerated and all children completed the 16-week therapeutic trial.14 The decision to not continue omalizumab in four children was due to lack of apparent symptomatic or objective benefit rather than adverse effects. There are logistical implications attached to the administration of fortnightly or monthly subcutaneous injections as there is a theoretical risk of anaphylaxis with omalizumab and specifically trained staff are required. We found a designated nurse-led clinic to be the most effective method.
Although outside the UK licence, a child aged 5 years underwent a therapeutic trial of omalizumab after careful multidisciplinary team discussion. This patient was critically dependent on oral corticosteroids to control their severe asthma and avoid frequent life-threatening exacerbations. The trial was of symptomatic benefit and the child has remained on omalizumab long term. An older 13-year-old was also prescribed omalizumab off-licence due to their IgE level and body weight exceeding recommendations. In this case the maximum recommended dose was administered and the child continued on omalizumab with clinical benefit.
The fact that omalizumab is administered as an injection in a nurse-led clinic means that concordance with treatment is definitively recorded. As outlined in online Appendix 1, it is our practice to only commence a trial of omalizumab in children who are dependent on oral corticosteroids to control their asthma after a thorough diagnostic investigation, home visit and concerted effort to check that concordance is maximised with their current standard asthma treatment. This allows a distinction to be made between children with asthma that is difficult to treat due to concordance, environmental, social and/or psychological issues and those with genuinely severe disease despite carefully administered maximal standard treatment. This is important because we consider that the use of this very expensive treatment should be limited to children with genuinely severe disease.
In conclusion, we report evidence of a significant oral corticosteroid-sparing effect during a 16-week therapeutic trial of omalizumab in 34 children with severe asthma that was associated with improvements in asthma control and quality of life. Similar benefits were seen in children both above and below 12 years of age. These uncontrolled data, while very encouraging, were obtained in a relatively small patient cohort and should be interpreted with appropriate caution. There is an urgent requirement for a multicentre randomised placebo-controlled trial of omalizumab in children with severe asthma, with reduction in oral corticosteroid dose as the primary outcome. The data presented should inform power calculations for such a trial. Other important research questions with regard to omalizumab in paediatric asthma include formal cost-effectiveness analyses, family-wide and societal quality of life measures, and confirmation of safety beyond 12 months.
Acknowledgments
The authors gratefully acknowledge the help of Ann Kirk and Sally Hails, Respiratory Nurse Specialists, Great North Children's Hospital, Newcastle upon Tyne, in collecting data, administering omalizumab and performing home visits.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Web Only Data - This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
-
Competing interests SM and DAS have received support to attend the European Respiratory Society annual congress from Novartis, and DAS has received honoraria for lectures from Novartis.
-
Provenance and peer review Not commissioned; externally peer reviewed.