Article Text

Abstract
Objectives To evaluate the efficacy and safety of ianalumab (VAY736), a B cell-depleting, B cell activating factor receptor-blocking, monoclonal antibody, in patients with active primary Sjögren’s syndrome (pSS) in a double-blind, placebo-controlled, phase II, single-centre study.
Methods Patients with pSS, EULAR Sjögren’s Syndrome Disease Activity Index (ESSDAI) ≥6, were randomised to ianalumab single infusion at either 3 mg/kg (n=6), 10 mg/kg (n=12) or placebo (n=9). Outcomes were measured blinded at baseline and weeks 6, 12, 24, and unblinded at end of study (EoS) when B cell numbers had recovered. Clinical outcomes included ESSDAI, EULAR Sjögren’s Syndrome Patient Reported Index (ESSPRI), salivary flow rate, ocular staining score, physician global assessment and patient assessments of fatigue and general quality of life. Laboratory-based measures included circulating leucocyte subsets and markers of B cell activity.
Results A similar trend showing positive therapeutic effect by ianalumab was observed across the primary clinical outcome (ESSDAI) and all secondary clinical outcomes (ESSPRI, Multidimensional Fatigue Inventory, Short Form-36, global assessments by physician and patient) versus the placebo-treated group. Rapid and profound B cell depletion of long-lasting duration occurred after a single infusion of ianalumab at either dose. Serum Ig light chains decreased, with return to baseline levels at EoS. Changes in some clinical outcomes persisted through to EoS in the higher dose group. Adverse effects were largely limited to mild to moderate infusion reactions within 24 hours of ianalumab administration.
Conclusions Overall results in this single-dose study suggest potent and sustained B cell depletion by ianalumab could provide therapeutic benefits in patients with pSS without major side effects.
- autoimmunity
- B cells
- treatment
- Sjögren'ssyndrome
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Patients with primary Sjögren’s syndrome (pSS) display numerous signs of B cell activation that appear involved in the pathobiology underlying this autoimmune disease. However, demonstrating the clinical benefits of depleting B cells in these patients have proved challenging in randomised, controlled clinical trials.
B cell activating factor (BAFF) is a key cytokine for B cells, promoting their maturation, proliferation and survival. Elevated BAFF levels are often present in patients with pSS, supporting autoimmunity and potentially blocking therapeutic elimination of pathogenic B cell clones.
What does this study add?
This is the first reported use of ianalumab (VAY736), a novel targeted biologic against the BAFF receptor (BAFF-R) on B cells with dual mechanisms of action: direct lysis of B cells and blockade of BAFF:BAFF-R signalling with its receptor.
This study demonstrates the safety and efficacy of a single dose of ianalumab administered to patients with pSS.
How might this impact on clinical practice or future developments?
Direct depletion of B cells coupled with blockade of BAFF:BAFF-R signalling may provide more thorough elimination of pathogenic B cells in patients with pSS and improve clinical outcomes.
Ianalumab is currently under development by Novartis for the treatment of pSS.
Introduction
Primary Sjögren’s syndrome (pSS) is a chronic autoimmune disease of unknown aetiology characterised primarily by lymphoid infiltration and progressive destruction of exocrine glands.1 Nearly all patients suffer from mucosal dryness, fatigue and diffuse musculoskeletal pain, with a subset of patients experiencing extraglandular disease manifestations with increased risk for lymphoma development.
Treatment is limited to symptomatic care of mucosal dryness. Steroids and typical disease-modifying antirheumatic drugs are ineffective, and there is no pharmacological intervention against the fatigue. Early efficacy of B cell depletion therapy in patients with pSS using anti-CD20 monoclonal antibody (mAb) rituximab2 3 was not replicated in subsequent studies,4–6 linked to persistence of Ig-producing clonal cells within the salivary glands.7
Patients with pSS have elevated levels of B cell activating factor (BAFF) correlating with disease activity, ectopic germinal centre formation and serum autoantibody levels.8 9 The BAFF receptor (BAFF-R; synonyms BR3, TNFSF13C) is predominantly expressed on B cells. Signalling of BAFF through the BAFF-R is critically involved in B cell maturation, activation and survival, and for isotype class switching in response to T cell-dependent antigens.10 High baseline BAFF levels in pSS and other autoimmune diseases such as systemic lupus erythematosus (SLE) and rheumatoid arthritis (RA) are inversely correlated with extent and duration of B cell depletion by rituximab, two efficacy markers for this treatment.9 11–13
Ianalumab (VAY736) is a human IgG1/κ mAb designed to target human BAFF-R and to competitively inhibit binding of BAFF to BAFF-R, thereby blocking BAFF-R-mediated signalling in B cells (online supplementary method 1). In addition, ianalumab was engineered to effectively eliminate B cells from circulation in vivo by antibody-dependent cellular cytotoxicity (ADCC). ADCC activity of ianalumab is greatly enhanced by elimination of fucose residues from the carbohydrate moiety attached to the Fc part of the antibody.14 Accordingly, ianalumab shows potent ADCC activity in vitro with an EC50 of 2.0 pM (online supplementary method 2). Thus, ianalumab eliminates BAFF-R + mature and immature B cells via dual mechanisms: (1) antibody-dependent cytotoxicity (ADCC) and (2) induction of B cell apoptosis by blocking BAFF:BAFF-R interaction and downstream survival pathway in B cells. BAFF-R expression is limited to immature and mature B cells up to the lymphoblast stage, and thus earlier stage pro-B and pre-B cells are not directly affected by ianalumab. Consequently, ianalumab should represent a more effective therapeutic agent in B cell-driven autoimmune diseases with high BAFF levels such as pSS.8 9 This clinical study was designed to evaluate safety, tolerability, pharmacokinetics (PK) and therapeutic efficacy of a single ianalumab intravenous infusion in patients with pSS to enable further development of the compound for treating this disease population.
Methods
This single-centre study (NCT02149420) was conducted between 23 May 2014 and 7 February 2018 (online supplementary method 3). Patients enrolled are 18–75 years fulfilling revised European US consensus criteria for pSS,15 antinuclear antibody (ANA) ≥1:160 and seropositive for rheumatoid factor (RF) or for anti-Sjögren’s-syndrome-related antigen A (anti-SSA), with stimulated whole salivary flow rate of >0 mL/min and active disease (EULAR Sjögren’s Syndrome Disease Activity Index [ESSDAI] ≥6). Exclusion criteria included concurrent connective tissue diseases, therapy with prednisone >10 mg/day or azathioprine within 84 days of randomisation, prior use of any B cell depleting therapy, or use of other biologics within 180 days prior randomisation. All patients provided written informed consent before study participation. The protocol and informed consent were approved by local ethics committee before study initiation.
Treatment
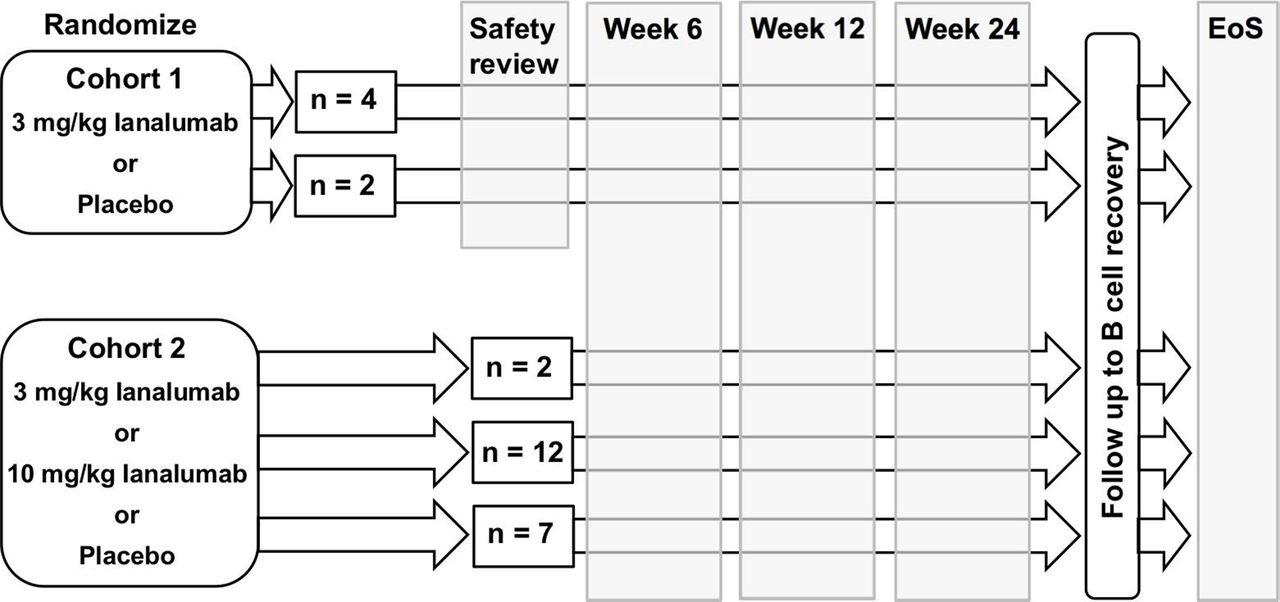
Patients meeting eligibility criteria were enrolled into two sequential cohorts (figure 1). Ianalumab (150 mg lyophilisate) was reconstituted with water and diluted in 5% dextrose infusion bag. Placebo was administered as vehicle only. Paracetamol 500 mg was administered 1 hour prior and 5 hours after ianalumab dosing. Patients were allowed use of artificial tears and artificial saliva/salivary stimulants outside of a 48-hour period before or during disease activity assessments.

Study design. Cohort 1: six patients randomised to receive single intravenous dose at 3 mg/kg ianalumab or placebo at 2:1 ratio, and cohort 2: 21 patients randomised to receive single intravenous dose ianalumab at 3 or 10 mg/kg, or placebo at a 1:6:3 ratio, respectively. A blinded review of safety data was performed on the first six patients of cohort 1 prior to advancing to cohort 2. Main study visit schedule was as follows: 28-day screening period prior to randomisation, baseline assessments and dosing over domiciled day 1 and day 2, study visits at weeks 1, 2, 3, 6, 9 and 12, then every 4 weeks until week 24. Safety follow-up visit schedule after week 24 was as follows: every 8 weeks until week 40, every 12 weeks to week 52, every 24 weeks to week 100 and every 48 weeks thereafter. Patients achieving B cell recovery criteria proceeded to EoS within 4 weeks. EoS, end of study.
Assessment time points
Blinded safety and efficacy markers were assessed on day 1 prior to drug administration and again at weeks 6, 12, 24 and at end of study (EoS). Patients returned for safety and PK evaluations at days 8 and 15, and weeks 3, 6, 9 and 12, and at 4-week intervals thereafter until week 24. Following week 24 assessments, patients were unblinded. Patients achieving B cell recovery criteria, defined as ≥80% of baseline levels or ≥50 cells/μL,16 proceeded to EoS visit within 6 weeks. Otherwise, patients remained in study for monitoring until meeting recovery criteria.
Clinical outcomes
The primary clinical outcome was the ESSDAI.17 18 Patient-reported outcomes included the EULAR Sjögren’s Syndrome Patient Reported Index (ESSPRI),19 Multidimensional Fatigue Inventory (MFI)20 and Medical Outcomes Study Short Form-36 (SF-36).21 Physician’s global assessment (PhGA) and patient’s global assessment (PaGA) were measured by 100 mm visual analogue scale (VAS). Functional clinical outcomes of disease activity included stimulated and unstimulated salivary flow rate and ocular staining score.22
Laboratory-based outcomes
Selective B cell depletion was evaluated by flow cytometry gated on CD45+ leucocytes to measure absolute counts of CD19+ B cells, B cell subsets and other leucocyte classes (online supplementary method 4). Soluble serum biomarkers included BAFF, autoantibodies (RF, ANA, anti-SSA and anti-SSB), β2 microglobulin, immunoglobulins (IgG, IgM) and free Ig light chains (kappa, lambda).
Pharmacokinetics
Serum ianalumab levels were measured on day 1 (before dose and at 2 hours after dose) and at each subsequent visit by validated ELISA (online supplementary method 5) with lower limit of quantification of 0.025 µg/mL.
Statistical analysis
The primary analysis for change from baseline in ESSDAI was conducted via a Bayesian repeated measures model, including data up to week 24. The posterior probabilities were used to evaluate the predefined dual efficacy criteria: more reduction in ESSDAI week 12 in ianalumab-treated patients than placebo with high confidence (90%), and an average magnitude (50%) of effect of 5 points more reduction in ESSDAI week 12 compared with placebo, where the 5 points more reduction is considered clinically meaningful difference. The study was powered for comparison of ianalumab treatment versus placebo regardless of dose levels. However, the data revealed some consistent difference in response between the two ianalumab groups; therefore, the Results section will focus on the individual ianalumab groups for discussion.
Results
Patient characteristics
A total of 27 patients were enrolled and randomised (figure 1) as follows: 3 mg/kg ianalumab (n=6), 10 mg/kg ianalumab (n=12), placebo (n=9). All enrolled patients completed the initial 24-week blinded period and were included for analysis, and all 18 patients from the ianalumab treatment groups completed the study through to time of B cell recovery.
Demographic and other baseline parameters were comparable for the three treatment groups (table 1). The primarily female patients had moderate to severe disease of ESSDAI between 6 and 19, except for one patient in the 3 mg/kg ianalumab group scoring 31. There was also comparable prior use of background corticosteroids, hydroxychloroquine and methotrexate that remained stable throughout the study.
Demographic and baseline disease characteristics of enrolled study patients
EULAR Sjögren’s Syndrome Disease Activity Index
After one infusion per patient, the difference at week 12 in the change from baseline ESSDAI between placebo and ianalumab-treated patients, including the combined ianalumab group as well as the two individual dose groups, did not meet the predefined criteria. High variability in this endpoint was observed especially in the ianalumab treatment groups (figure 2). Evaluation of individual ESSDAI domains revealed that most improvement was in the articular domain with ianalumab treatment (data not shown). ESSDAI scores at EoS in patients treated with 10 mg/kg ianalumab remained at reduced levels achieved over the 24-week blinded period, while scores in patients receiving 3 mg/kg ianalumab returned towards baseline values.

Time course of selected clinical outcomes in the first 24 weeks and EoS. Change from baseline values is shown in box plots. Arithmetic means are shown in diamonds in the box plots. Dotted horizontal line denotes a change from baseline of zero, that is, no difference from baseline. Time of actual EoS visits ranged from 39 to 154 weeks. Comparative EoS data are lacking for placebo arm patients due to transition after week 24 to open-label ianalumab treatment. BL, baseline; EoS, end of study; ESSDAI, EULAR Sjögren’s Syndrome Disease Activity Index; ESSPRI, EULAR Sjögren’s Syndrome Patient Response Index; MFI, Multidimensional Fatigue Inventory.
Patient-reported outcomes
The ESSPRI is the average of scores for the three symptoms of dryness, fatigue and pain. Changes in ESSPRI over the study course are shown in figure 2. At week 12, no significant difference was observed in change from baseline of ESSPRI between ianalumab groups and placebo. In the 3 mg/kg ianalumab group, ESSPRI reduction appeared transient; an early reduction at week 6 returned towards baseline by week 12 and even increased at EoS. In contrast, ESSPRI reduction in the 10 mg/kg ianalumab group was maintained until week 24 and at EoS. A repeated measurement model for this outcome revealed greater reductions in the 10 mg/kg ianalumab group versus placebo at week 12 (1.55 points; 95% CI 0.03 to 3.08) and at week 24 (1.92 points; 95% CI 0.33 to 3.52). Individual evaluation of the three ESSPRI components suggested more improvement occurred in dryness and fatigue for most ianalumab-treated patients compared with patients receiving placebo, especially at week 12 (data not shown).
Severe fatigue affects up to 70% of patients with pSS and is a major contributor to disease-associated disability.23 24 The MFI individually assesses five different parameters of fatigue, including general fatigue, physical fatigue, mental fatigue, reduced activity and reduced motivation. Early but transient response to treatment with 3 mg/kg ianalumab was observed at week 6 in all the MFI domains (statistically significant for general fatigue and physical fatigue), with scores returning to baseline by week 24 (physical fatigue, figure 2; others in online supplementary figure S1). For the 3 mg/kg ianalumab group at week 6 there was a 5.4-point greater reduction from baseline in general fatigue score (95% CI 0.97 to 9.72) and in physical fatigue score there was a 4.4-point greater reduction from baseline (95% CI 0.87 to 7.96), both with statistical significance. In contrast, in the 10 mg/kg ianalumab group, early reductions were observed at week 6 for all MFI domains, sustained between week 6 and week 24, and continued to EoS for the MFI domains of general fatigue, physical fatigue and reduced activity.
Supplemental material
Changes from baseline over the study for SF-36, PaGA and PhGA were similar to patterns observed for ESSDAI, ESSPRI and MFI (figure 2, online supplementary figures S2 and S3). Early responses in patients receiving 3 mg/kg ianalumab tended to be transient and returned towards baseline levels by week 24 and EoS. Patients in the 10 mg/kg ianalumab group tended towards more sustained clinical responses up to week 24 and, for PaGA and PhGA, responses, extended out to EoS.
Salivary flow rate and ocular staining score
Variability for these two outcomes was high in all groups, making difficult any comparison between ianalumab groups and placebo groups (online supplementary figures S4 and S5). Ianalumab-treated patients had numerically greater increases in unstimulated salivary flow from week 6 to week 24 and in stimulated salivary flow from week 12 to week 24, with both measurements declining back towards baseline at EoS in ianalumab-treated patients. Ocular staining scores for both eyes in patients receiving 10 mg/kg ianalumab remained reduced from baseline through to EoS, but of uncertain clinical relevance.
Laboratory biomarker analysis
B cell and B cell subsets. Minimal changes occurred over time in circulating CD19+ B cell numbers for placebo-treated patients. In contrast, a single infusion of ianalumab resulted in rapid and profound depletion of CD19+ B cells in the two-dose groups (figure 3). Patients in the 10 mg/kg ianalumab group widely varied, with a time to reach minimum, post-treatment B cell numbers ranging from 1 to 83 days. In contrast, patients receiving the 3 mg/kg dose achieved maximum depletion by 2 weeks after treatment.

B cell depletion/serum BAFF levels. The top panel shows the individual CD19+ B cell count over time for three treatment groups, with a horizontal line at 50 cells/µL to denote the lower limit of normal. Both x and y axes are presented in log10 scale. The bottom panel shows the BAFF levels in box plots over time, where the arithmetic means are illustrated with diamonds. The y axis is presented in log10 scale. Time of actual EoS visits ranged from 39 to 154 weeks. Absence of EoS data for placebo patients as noted in the Methods section. BAFF, B cell activating factor; EoS, end of study.
Time to B cell recovery also varied considerably between individual patients, ranging from week 7 to week 148, both extreme cases occurring in the 3 mg/kg ianalumab group. Recovery time in the 10 mg/kg dose group ranged from 16 to 76 weeks. Median recovery time was 402 days in the 3 mg/kg ianalumab group and 224 days in the 10 mg/kg ianalumab group. Within the CD19+ B cell population, substantial depletion occurred within 24 hours in the peripheral blood mature, naive, memory and transitional B cell subsets (data not shown). By EoS, these B cell subpopulations had returned to baseline levels with the exception of memory B cells which were increased relative to naive B cells. Additionally, at day 2 after ianalumab exposure, transient reductions occurred in non-B cell leucocytes, primarily of effector cells involved in B cell lysis (eg, T cells and natural killer cells). All largely recovered back towards baseline levels by day 7 (data not shown). No impact on leucocyte surface activation markers related to the treatment was observed.
B cell activity markers. There was no consistent difference in percentage change from baseline in autoantibody levels. However, compared with placebo-treated patients, there were numerically greater reductions from baseline in serum levels of free kappa and lambda Ig light chains in ianalumab-treated patients which returned to baseline by EoS (online supplementary figure S6).
Within 24 hours of ianalumab dosing, patients’ serum BAFF levels peaked, followed by persistently elevated values until at least week 24, returning towards baseline by EoS (figure 3). Baseline BAFF levels in ianalumab-treated patients did not correlate with the change from baseline in any clinical outcomes at week 12 or at week 24 (online supplementary figure S7).
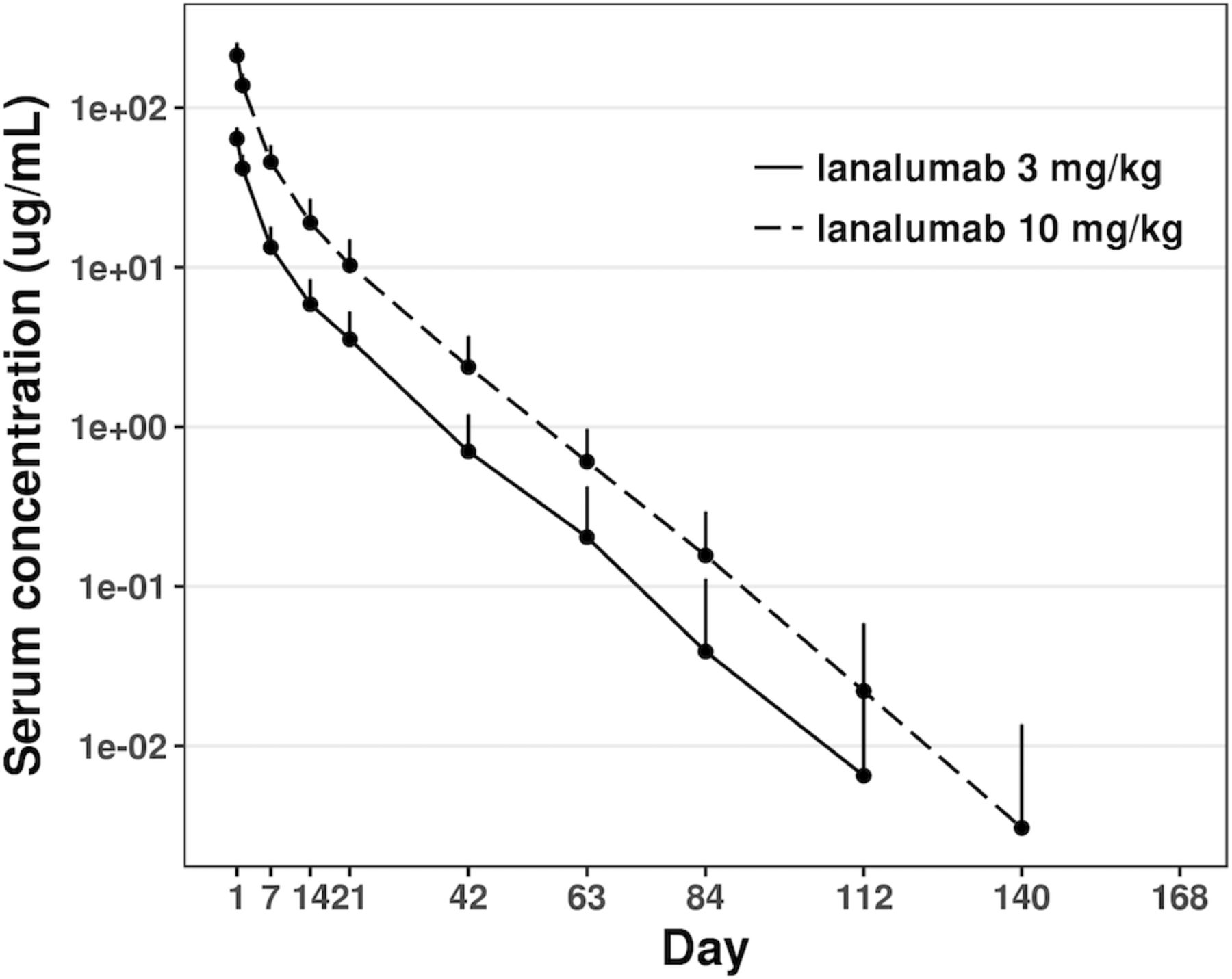
Pharmacokinetics. Ianalumab exhibited a typical PK profile for a mAb of the IgG1 type (figure 4). A 3.3-fold increase in dose resulted in a 3.1-fold increase in area under the curve and a 3.3-fold increase in Cmax. Elimination of ianalumab was relatively fast for a mAb, with an average half-life around 9–10 days.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
VAY736 concentration-time profiles. Arithmetic mean of VAY736 serum concentration profiles after a single intravenous dose of 3 mg/kg (solid line) and 10 mg/kg (long dash line, only double-blind period), along with SD illustrated by a short vertical interval. The y axis is shown in log10 scale.
Safety analysis
Adverse events (AE). Most AEs were mild to moderate in severity without any severe AEs suspected related to ianalumab (table 2). The most commonly observed AE was mild to moderate infusion-related reaction, characterised by acute onset within hours after ianalumab exposure of one or more of the following: headache, fever, chills, nausea and arthralgias. Fifteen patients receiving ianalumab experienced an infusion reaction (83.3%) compared with one placebo-treated patient (11.1%). Infusion reactions were mild (n=3) to moderate (n=12) in severity and not related to dose but did trend with the number of circulating B cells present at baseline; patients with moderate infusion-related reactions tend to have relatively higher B cell counts at baseline than those with mild reaction or none (online supplementary figure S8). All infusion-related reactions resolved within 24 hours either spontaneously or with additional paracetamol treatment.
Most frequent AEs occurring in two or more patients reported during double-blind period
The reported incidence of nasopharyngitis was also higher in ianalumab-treated patients (n=6; 33.3%) versus placebo-treated patients (n=1; 11.1%). There was no increase in infections otherwise in the ianalumab group versus placebo group, nor in the incidence of other AEs over the 24-week, blinded study period.
Clinical laboratory findings. Treatment with ianalumab was not associated with significant changes in circulating neutrophils or IgG levels. IgM levels decreased in ianalumab-treated patients but remained within normal limits and had largely returned to baseline levels by EoS (online supplementary figure S9).
Discussion
In this trial, the strongest benefit observed in these patients with pSS after receiving ianalumab (VAY736) was reduction of fatigue, a major pSS disease component typically resistant to therapeutic intervention.6 Patients treated with ianalumab showed reductions in all elements of fatigue measured by the MFI, with particularly strong responses in general fatigue and physical fatigue. This is consistent with reported benefits of B cell-targeted therapy on patient fatigue in pSS and other diseases. Reduction of fatigue in response to rituximab has been observed in patients with RA, SLE and chronic fatigue syndrome.25–27 Patients with pSS receiving open-label rituximab reported reductions in VAS-measured fatigue.28 However, rituximab effects on fatigue in larger, placebo-controlled pSS studies showed either only transient reduction of fatigue that did not persist at 24 weeks4 or no reduction at all.6 Blockade of soluble BAFF by belimumab in patients with SLE enrolled in the BLISS study had significant improvement of their fatigue,29 with further improvement in responders over the second half year of exposure. The benefits on fatigue observed in this pSS study with ianalumab will require confirmation in larger trials with longer exposure and observation time.
A single dose of ianalumab did not meet predefined criteria for the primary endpoint ESSDAI. In addition, a post hoc analysis was performed for the more recently developed endpoint, the ClinESSDAI,30 developed particularly for B cell-targeted therapies. The results in this endpoint (online supplementary figure S10) are similar to findings with ESSDAI (figure 2). However, in addition to the benefits on fatigue (MFI), a trend showing positive therapeutic effect by the compound versus placebo was observed for the ESSDAI and across the other key secondary clinical outcomes, including the primary (ESSDAI) and all secondary clinical outcomes (ESSPRI, SF-36, global assessments by physician and patient).
There was variability between the two ianalumab dose groups in the clinical outcomes of ESSDAI, ESSPRI, MFI and patient and physician global assessments. In some outcomes, the effect of 3 mg/kg ianalumab appeared transient, with early signs of improvement at week 6 returning back towards baseline by week 12 or 24. In contrast, patients receiving 10 mg/kg ianalumab showed sustained effects up to week 24. These observations were in accordance with the observed ianalumab exposure, that is, ianalumab quantifiable levels detected approximately up to 8–12 weeks and to 12–16 weeks for the 3 mg/kg and 10 mg/kg dose groups, respectively. This dose response in duration of clinical outcomes suggests that more sustained exposure to the compound may be more effective against the pSS disease process.
Ianalumab was well tolerated by patients, with AEs largely limited to infusion reactions of mild to moderate intensity occurring within 24 hours after infusion. There was a trend between the baseline B cell numbers and severity of infusion reactions, consistent with the rapid lysis of circulating B cells by ianalumab. Aside from an increase in the incidence of nasopharyngitis, there were no other adverse effects associated with ianalumab that were increased compared with placebo. Importantly, there were no incidences of late-onset neutropenia or hypogammaglobulinaemia in these ianalumab-treated patients over the B cell recovery period.
Rapid, selective and profound B cell depletion occurred in these patients after a single infusion of ianalumab at either 3 mg/kg or 10 mg/kg. Depletion was also long lasting, with only 14 of 18 patients achieving minimal B cell recovery criteria at 1 year. Ianalumab-mediated depletion occurred across B cell subsets, including mature, naive, memory and transitional B cells, with an increase observed in the proportion of mature over naïve B cell populations at EoS; a finding also reported for patients treated with rituximab.28 Additional evidence of ianalumab effects on the underlying pSS disease process includes reduction of Ig free light chains; a parameter characteristically elevated in B cell-driven autoimmunity and correlated in patients with pSS to disease activity and extraglandular involvement.31
Initial, sharp peaks in BAFF levels in the immediate, 24-hour period after ianalumab administration are likely due to a combination of factors, including (1) an acute drop in the number of available receptors for BAFF due to receptor binding by ianalumab and to rapid reduction of B cells expressing BAFF-R, (2) release of stored BAFF by lysed cells, and (3) increased BAFF production in response to lowered B cell numbers. BAFF levels remained elevated in these ianalumab-treated patients, with a gradual return to baseline levels in parallel with B cell recovery, consistent with findings with B cell depletion by rituximab in this patient population.28
In this study, no correlations were found between baseline BAFF serum levels and the clinical efficacy endpoints. This is in contrast to B cell depletion by CD20-targeted therapy with rituximab where higher baseline BAFF levels correlated with attenuated efficacy.9 32 Thus, the absence of such correlations may reflect the ianalumab dual mechanisms of action blocking BAFF:BAFF-R signalling as well as direct, ADCC-mediated B cell depletion. This BAFF-R signalling blockade by ianalumab is important because BAFF levels elevated on B cell depletion are thought to protect B cells from depletion by rituximab and to drive disease relapse in patients with SLE.33 In patients with immune thrombocytopenic purpura, high BAFF levels following rituximab treatment may cause differentiation of pathogenic, long-lived plasma cells.34 Thus, the ianalumab dual mechanisms of action may provide more thorough B cell elimination within tissues while also reducing the incidence of BAFF-driven disease flare; a hypothesis pursued by SLE studies combining direct B cell depletion and soluble BAFF blockade by initial treatment with rituximab followed by a maintenance regimen with belimumab35 and also under consideration for pSS (NCT02631538).
In conclusion, the overall results of this study suggest that potent and sustained B cell depletion by ianalumab could lead to therapeutic benefits in patients with pSS without major safety issues. However, it should be noted that this initial phase II trial involved patients of a heterogeneous phenotype recruited according to ESSDAI score. Also, there was no direct evaluation in these patients of drug effect at the tissue level, for example, through minor salivary gland biopsies. There were also inconsistent effects by ianalumab on objective parameters of pSS disease activity such as salivary flow and ocular staining scores. Nevertheless, patients in this single-dose study, though limited to a small number, appeared to benefit from a single infusion of ianalumab, and further efficacy with greater exposure is suggested by sustained clinical changes in higher dosed patients out to EoS; a time for which minimal pharmacodynamic effects remained of the compound. Although the EoS assessments were by necessity open label, these persisting clinical benefits suggest potential for long-term disease modification with ianalumab treatment. Thus, determination of efficacy for ianalumab in pSS will require further investigation of more sustained treatment in larger numbers of patients, and a larger phase II study in patients with pSS is currently underway (NCT02962895).
References
Footnotes
TD and MGP contributed equally.
Handling editor Josef S Smolen
Presented at Portions of these reported findings have been presented in poster or podium format at the following conferences: (1) Poster presentation at the European Union League Against Rheumatism 2016 Congress: Dörner T, Posch M, Wagner F, Hüser A, Fischer T, Mooney L, Petricoul O, Maguire P, Pal P, Doucet J, Cabanski M, Kamphausen E, Oliver S. Double-blind, randomized study of VAY736 single dose treatment in patients with primary Sjögren’s syndrome (pSS). Ann Rheum Dis 2016; 75(suppl 2):S300. (2) Podium presentation at the American College of Rheumatology 2016 National Meeting: Dörner T, Posch M, Wagner F, Hüser A, Fischer T, Mooney L, Petricoul O, Maguire P, Pal P, Doucet J, Cabanski M, Kamphausen E, Kazma R, Oliver S. Safety and efficacy of single dose VAY736 (anti-BAFFR mAb) in patients with primary Sjögren’s syndrome (pSS). Arthritis Rheum 2016; 68 (suppl S10):3033.
Contributors SJO, OP, MAV, TD, MGP, LM, FDW and AH participated in the design, conduct and analysis of the study. HG provided preclinical background and participated in analysis and manuscript preparation. MC, JMM, MGP and CS participated in the conduct and analysis of the study. All authors contributed to manuscript preparation and review.
Funding This study was funded by Novartis Pharma.
Competing interests All authors listed as affiliated with Novartis Pharma are full-time employees of the company, with SJO, OP, LM, MAV and CS also owning company stock. TD has received scientific consulting fees from Novartis. FDW, MGP and AH are employees of the Charité Research Organisation which has past and currently ongoing contract work with Novartis Pharma.
Patient consent for publication Not required.
Ethics approval This study was conducted in accordance with the Declaration of Helsinki, the International Conference on Harmonisation Guidelines for Good Clinical Practice and local regulations. The protocol, consent form and any other written information provided to patients were approved by the Ethik-Kommission des Landesamt für Gesundheit und Soziales Berlin.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Additional study design details and study results are available on www.clinicaltrials.gov under the listed trial identifier.