Article Text

Abstract
Background: Heterogeneous data have been reported regarding the detection and number of circulating endothelial progenitor cells (EPCs) in systemic sclerosis (SSc).
Objective: We investigated the number of circulating EPCs using recent recommendations and we quantified their late outgrowth in patients with SSc and healthy controls.
Patients and methods: EPCs, defined as Lin–/7AAD–/CD34+/CD133+/VEGFR-2+ cells, were quantified in 50 patients with SSc (mean age: 55 (16) years, disease duration: 9 (9) years) and 26 controls (mean age: 53 (19) years) by cell sorting/flow cytometry and by counting late outgrowth colony-forming units (CFU).
Results: Patients with SSc displayed higher circulating EPC counts than controls (median 86 (5–282) vs 49 (5–275)) EPCs for 1 million Lin– mononuclear cells; p = 0.01). Lower EPC counts were associated with the higher Medsger’s severity score (p = 0.01) and with the presence of past and/or current digital ulcers (p = 0.026). There was no difference for the number of late outgrowth EPC-CFUs between patients with SSc and controls in cell culture evaluation. The formation of colonies was associated with higher levels of circulating EPCs (p = 0.02) and the number of colonies correlated with levels of EPCs (R = 0.73, p = 0.0004), validating our combination of fluorescence-activated cell sorter surface markers.
Conclusions: We quantified circulating EPCs with an accurate combination of markers herein validated. Our data demonstrate increased circulating EPC levels in SSc, supporting their mobilisation from bone marrow. Furthermore, the subset of patients with digital vascular lesions and high severity score displayed low EPC counts, suggesting increased homing at this stage. The predictive value of this biomarker now warrants further evaluation.
Statistics from Altmetric.com
Systemic sclerosis (SSc) is a severe connective tissue disorder1 of unknown origin that affects the skin and internal organs. Cardiovascular2 and small vessel involvement3 4 are key features of the disease, with perivascular inflammatory infiltrates preceding the onset of systemic fibrosis. The microvascular network of patients with SSc is less dense than normal and has a chaotic structure. These abnormalities result in blood flow being insufficient thereby causing a severe tissue hypoxia,5 which is a major stimulus for angiogenesis. However, adapted angiogenesis does not occur in patients with SSc despite severe tissue hypoxia.6 Indeed, defective vascularisation contrasts with the overexpression of vascular endothelial growth factor (VEGF) in the serum7 and in the skin5 8 of patients with SSc throughout various stages of the disease.
New blood vessels may form in two ways in human adults: via endothelial sprouting from pre-existing endothelial cells (angiogenesis) or via the peripheral recruitment of circulating endothelial progenitor cells (EPCs) (vasculogenesis).9 EPCs, first described by Asahara et al,10 are a population of bone marrow-derived cells characterised by the presence of surface markers such as CD34, VEGF receptor-2 (VEGFR-2 or kinase-insert domain receptor, KDR)11 and CD133,12 able to differentiate into mature endothelial cells and to participate in the formation of new blood vessels. It has been previously suggested that vasculopathy in SSc may be related to insufficient vascular repair machinery due to defective vasculogenesis. Indeed, Kuwana et al13 performed EPC detection by immunomagnetic separation of CD34+ cells and triple labelling with conjugated monoclonal antibodies to CD34, CD133 and VEGFR-2 and found that patients with SSc had fewer circulating EPCs than patients with rheumatoid arthritis or healthy controls. By contrast, two other studies performed on whole blood reported significantly higher numbers of circulating EPCs (defined as CD34+/CD133+ cells) in patients with SSc than in healthy subjects concomitantly with increased levels of activated circulating endothelial cells.14 15 Thus, findings concerning EPC levels in SSc seem to be conflicting; however, these different reports were based on different methods and definitions, which have been recently standardised by the publication of general recommendations improving EPC detection by flow cytometry.16
Previous data also suggested that early outgrowth EPCs from patients with SSc displayed a lower ability to differentiate into mature endothelial cells in vitro despite the paradoxically high concentrations of angiogenic factors.13 However, early outgrowth EPCs are known to have monocytoid features and weak proliferation potential.17 Another distinct group of EPCs isolated from mononuclear cells has been described, called late outgrowth EPCs or endothelial colony-forming cells. These cells appear after a longer time in culture than the early outgrowth EPCs, have a stronger proliferative capacity, uniformly express endothelial markers and form perfused vessels in vivo.18
We aimed to investigate the number of circulating EPCs to assess the heterogeneity of previously published data. We quantified EPCs by flow cytometry on a large sample size of patients with SSc, according to recent recommendations,16 and by counting late outgrowth EPC colony-forming units (CFU).
PATIENTS AND METHODS
Patients
We included consecutive patients with SSc referred to the “Rheumatology A” Department over a 9-month period for systematic follow-up. All patients gave informed consent for all procedures, which were carried out with local ethics committee approval. Three months of stable current treatment were necessary for inclusion, and prednisone use at a dose of less than 10 mg/day was authorised. Vasodilators, including calcium channel blockers and angiotensin-converting enzyme (ACE) inhibitors, had to be withdrawn at least 3 days before inclusion (corresponding to more than five times the drug half-life). Smoking, diabetes or current treatment for dyslipidaemia were exclusion criteria. We carried out a global evaluation of these patients, based on collection of the following data: age, sex, cutaneous SSc subtype as defined by LeRoy et al,19 disease duration (date of first non-Raynaud symptom), duration of Raynaud phenomenon, erythrocyte sedimentation rate (ESR), C-reactive protein (CRP) concentration, digital ulceration (past or current) and prostacyclin use.
Pulmonary fibrosis was assessed by computed tomography (CT) scan and respiratory function tests (forced vital capacity and carbon monoxide diffusion capacity divided by alveolar volume). An echocardiographically estimated systolic pulmonary artery pressure >40 mmHg was used as a screening threshold for pulmonary arterial hypertension (PAH). Additional clinical criteria were DLCO below 50% of predicted in the absence of pulmonary fibrosis and unexplained dyspnoea. Patients identified by the above combination of non-invasive tests and clinical assessments were offered right heart catheterisation. Confirmed PAH was defined as a resting mean pulmonary artery pressure ⩾25 mmHg with a pulmonary capillary wedge pressure of ⩽15 mmHg measured at right heart catheterisation.20 Disease severity was assessed by the Medsger’s severity score.21
Von Willebrand factor antigen and sera VEGF were assayed to provide a marker of endothelial injury.22 Von Willebrand concentration was determined by ELISA (VIDAS von Willebrand, BioMérieux, Marcy l’Etoile, France) and VEGF levels by sandwich ELISA (R&D Systems, Minneapolis, MN, USA).
Blood samples were also collected from 26 healthy non-smokers recruited among hospital staff, free of usual cardiovascular risk factors, matched for age and sex with patients with SSc.
Cell-sorting and flow cytometry quantification
Fifty millilitre samples of heparinised venous blood were taken at rest from the forearm, in the morning, at the same time as samples collected from hospitalised patients for routine analysis. Samples were immediately transported to the laboratory for testing.
We used a validated method to enrich immature mononuclear cells.23 Negative lineage (Lin–) mononuclear cells were obtained by enrichment from 10 ml peripheral blood mononuclear cells using 500 μl of a human progenitor cell enrichment cocktail (RosetteSep, StemCell Technologies, Vancouver, Canada). This antibody cocktail cross-links unwanted Lin+ cells in whole blood to numerous red blood cells to form immunorosettes. This increases the density of the unwanted (rosetted) cells, such that they pellet along with the free red blood cells when centrifuged over the buoyant density medium. The enriched negative lineage mononuclear cells were collected by Ficoll density gradient centrifugation (Pancoll, Dutcher, Brumath, France), then washed and preincubated for 15 min with 50 μl of a FcR blocking reagent (Miltenyi Biotec, Paris, France) to inhibit non-specific binding or specific binding via Fc receptors. These cells were then subjected to triple labelling with 5 μl of each anti-CD133-phycoerythrin (PE, Miltenyi Biotec) and anti-CD34-fluorescein isothiocyanate (FITC, BD Bioscience, Le Pont de Claix, France) antibodies and 20 μl of anti-VEGFR-2 (KDR)-allophycocyanin (APC, R&D Systems) antibodies. Five μl of 7AAD (BD Bioscience) was used for real-time viability staining to identify dead cells 20 min before flow cytometry. Control cells were also prepared by incubation with fluorescence-labelled isotype-matched monoclonal antibodies (Beckman Coulter, Villepinte, France).
The labelled cells were analysed using a fluorescence-activated cell sorter (FACS; four-colour flow cytometry with a FACSCalibur flow cytometer (Becton Dickinson Le Pont de Claix, France)). A large number of events (at least 5×105) was considered for every sample. The same detector sensitivity, compensation setting, and scatter gate set were used to analyse all samples.
Viable cells were identified by gating on forward/side scatters and as the 7AAD– population. The expression of CD133 and VEGFR-2 by gated viable CD34+ cells was assessed. The EPC population was identified as Lin–/7AAD–/CD34+/CD133+/VEGFR-2+ cells. Data were analysed with WinMDI software. Results were expressed as the number of EPCs per million Lin– mononuclear cells.
Concordance correlation coefficient was used to assess reproducibility of the FACS analysis,24 on eight samples, with two measures at 48 h intervals.
Endothelial progenitor cell quantification by late outgrowth colony-forming unit assay
We used a method of culture suitable for obtaining late outgrowth EPC-derived colonies (fig 1).18 The blood mononuclear cell fraction was collected by Ficoll (Pancoll) density gradient centrifugation and was resuspended in complete EGM-2 medium (Cambrex, Ermerainville, France). Cells were then seeded on to separate wells of a 12-well tissue culture plate precoated with type I rat tail collagen (BD Biosciences) and stored at 37°C, under 5% CO2, in a humidified incubator. After 24 h of culture, non-adherent cells and debris were aspirated, adherent cells were washed once with phosphate-buffered saline 1×, and complete EGM-2 medium was added to each well. Medium was changed daily for 7 days and then every other day until the first passage. Colonies of endothelial cells appeared between 8 and 26 days of culture and were identified as well-circumscribed monolayers of cells with a cobblestone appearance. EPC cell colonies were counted visually under an inverted microscope (Olympus, Paris, France) and the delays before their appearance in patient and control samples were compared.

To further validate our method for quantification of late outgrowth EPCs, we determined the proliferation capacity of these cell in patients with SSc (n = 5), healthy controls (n = 5) and human umbilical vein endothelial cells (HUVECs). At each passage, cells were counted for calculation of a growth curve. The number of divisions was estimated using the following equation: (Ln(number of cells counted/number of cells at the beginning of the assay)/Ln2).
Statistical analysis
All data are presented as median (range), unless stated otherwise. The χ2 test was used to compare categorical variables. Correlations between EPC levels and various quantitative SSc disease variables were assessed using Spearman’s rank correlation test. Comparison between any two groups was by non-parametric Mann–Whitney and Kruskal–Wallis test. A probability value <0.05 was considered statistically significant.
RESULTS
Study population
We included 50 consecutive patients with SSc with a mean age of 55 (16) years and mean disease duration of 9 (9) years. None of these patients was taking immunosuppressive drugs. Detailed characteristics of patients with SSc are provided in table 1. Controls were matched for age (53 (19) years) and sex (77% women).
Circulating endothelial progenitor cell levels in systemic sclerosis
The Lin– progenitor population was analysed by flow-cytometric analyses for CD133 and VEGFR-2 labelling on gated CD34+ and 7AAD– cells. Samples from representative participants are shown in fig 2(A,B).
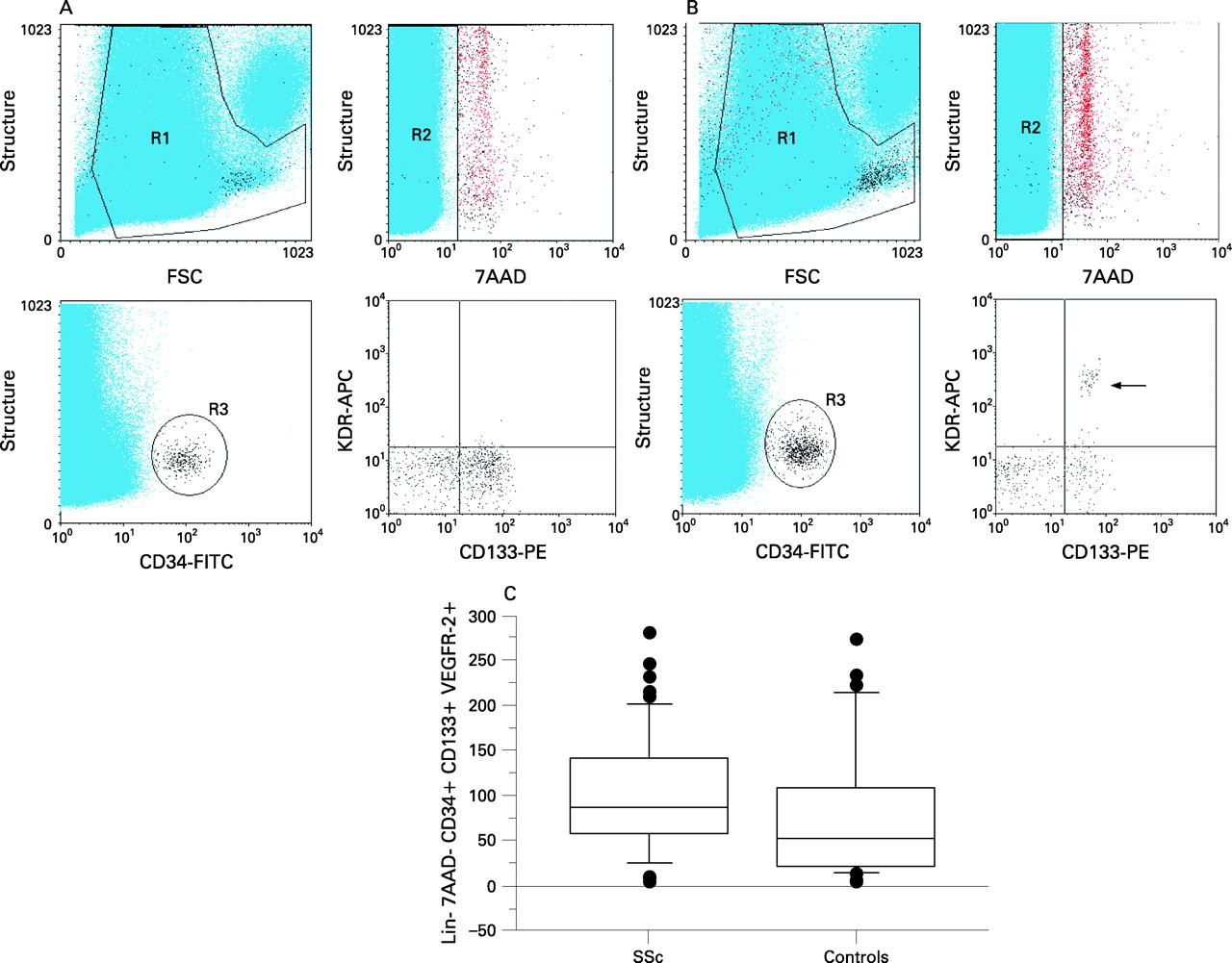
EPC levels (Lin–/7AAD–/CD34+/CD133+/VEGFR-2+) were significantly higher in patients with SSc than in healthy controls (median: 86; range: 5–282 vs median: 51; range: 5–275 EPCs per million Lin– mononuclear cells; p = 0.01) (fig 2C).
The numbers of circulating Lin–/7AAD–/CD133+/VEGFR-2+ and Lin–/7AAD–/CD34+/VEGFR-2+ cells were also significantly higher in patients with SSc (table 2), whereas the number of circulating Lin–/7AAD–/CD34+/D133+ and Lin–/7AAD–/CD34+ cells did not differ significantly between patients with SSc and controls.
Reproducibility of flow cytometry analysis
In order to validate our method, we assessed its reproducibility. The concordance correlation coefficient determined on eight different samples, with two measures at 48 h intervals, was 0.85.
Disease phenotype association of circulating endothelial progenitor cell levels
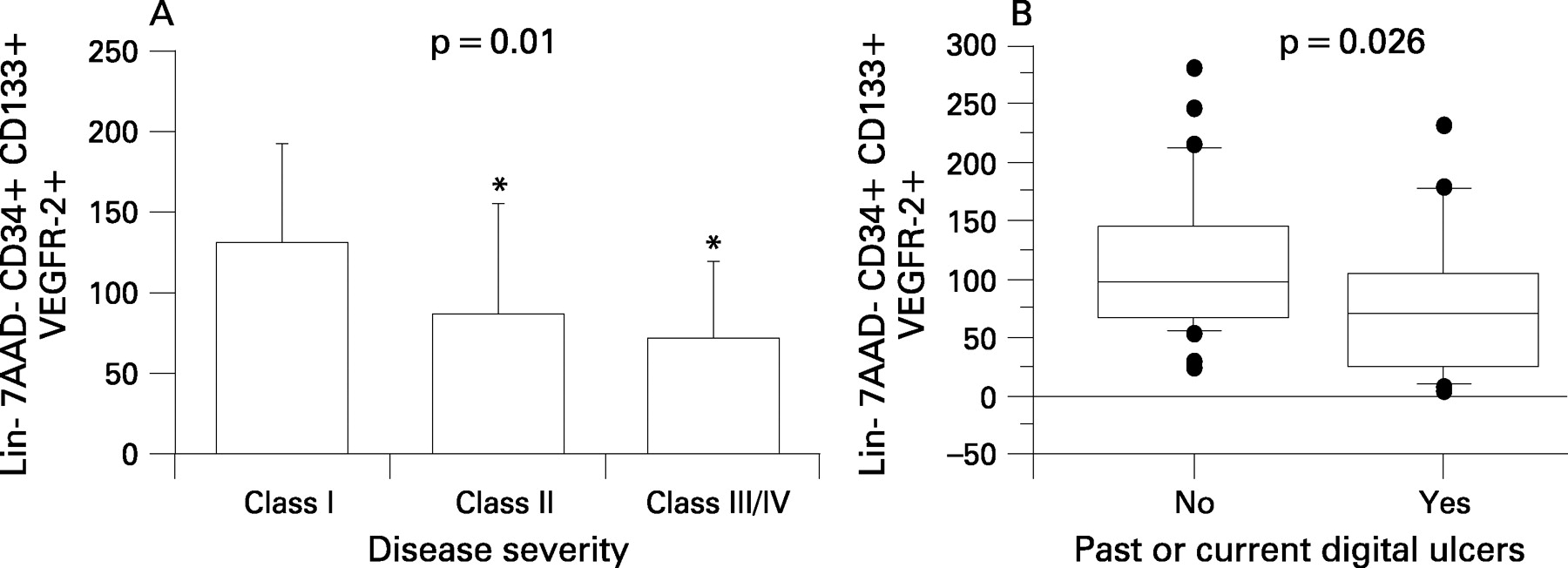
EPC levels were found to be lower in patients with SSc with the higher Medsger’s severity score; the median value was 129.5 (54–282) in class I (n = 16), 85 (10–248) in class II (n = 19) and 71 (5–180) in class III–IV (n = 15), p = 0.01 (Kruskal–Wallis test) (fig 3A). Low EPC counts in patients with SSc were also associated with the presence of past and/or current digital ulcers (median 70 (5–233) vs 97 (25–282); p = 0.026) (fig 3B). Patients with PAH had lower EPC values (median 71 (3–25)) than patients without (median 92 (5–282)), but the difference was not significant (p = 0.19).

Quantification of late outgrowth endothelial progenitor cell colony-forming units
Late outgrowth EPC-CFU were obtained from 24 (48%) patients with SSc and 13 (50%) controls. The lag before colony appearance and the number of CFU did not differ between patients with SSc and controls. The formation of colonies and a delay before colony appearance <15 days were associated with higher levels of circulating EPCs detected by FACS in patients with SSc (respectively p = 0.02 and 0.006) (fig 4A). Moreover, the number of colonies positively correlated with levels of EPCs (R = 0.73, p = 0.0004) defined as Lin–/7AAD–/CD34+/CD133+/VEGFR-2+ cells in patients with SSc (fig 4B). No association was found between the number of CFU and count of other putative EPC populations (Lin–/7AAD–/CD133+/VEGFR-2+ and Lin–/7AAD–/CD34+/VEGFR-2+). There was also no association between the number of CFU and disease features in patients with SSc.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
The proliferation potentials of EPC-derived cells from patients with SSc and controls were greater than HUVECs (respectively 32 vs 20 population doublings under the same culture conditions).
Discussion
We validated herein an accurate, reliable and reproducible method of EPC quantification. Our data support high levels of circulating EPCs in SSc, defined as Lin–/7AAD–/CD34+/CD133+/KDR+ cells. Furthermore, lower EPC number were associated with hand vascular lesions and high severity score.
EPCs are rare in adult peripheral blood (0.0001%). Thus, detection and quantification of circulating EPCs by flow cytometry are complex tasks from technical and biological viewpoints.16 EPCs must be shown to be distinct from other angiogenic cells, including mature circulating endothelial cells. Therefore, rigorous detection of these cells requires an accurate set of markers and the avoidance of non-specific staining caused by debris, dead cells and binding via Fc receptors. To improve assays for these rare events, we followed recent recommendations for the detection of EPCs by flow cytometry:16 we sorted cells to enrich the lineage-negative population; we used a real-time viability staining to exclude dead cells and a specific blocking serum to decrease non-specific binding via Fc receptors; and we acquired a large number of events. These methodological points may account for discrepancies observed between the herein study and previous analyses performed on whole blood14 15 and also for some of the different results obtained by Kuwana et al.13 The latter enriched CD34+ cells from peripheral blood mononuclear cells with an immunomagnetic technique, which may change the validity of the quantification as it has been shown that some putative EPCs populations may be CD34–.25 Moreover, these authors did not use real-time viability staining and FcR-blocking serum.
Our method was validated by testing reproducibility, which was not assessed in previous studies, and by the finding of a positive correlation in patients with SSc between the number of late outgrowth colonies and levels of circulating EPCs detected by flow cytometry and defined as Lin–/7AAD–/CD34+/CD133+/VEGFR-2+ cells. The absence of the association between other putative EPC populations (Lin–/7AAD–/CD133+/VEGFR-2+ or Lin–/7AAD–/CD34+/VEGFR-2+ cells) and formation/number of late outgrowth colonies suggests that the Lin–/7AAD–/CD34+/CD133+/VEGFR-2+ combination should be considered as the most suitable for EPC detection by flow cytometry. Thus, this EPC definition may allow the use of EPCs as reliable biomarkers and facilitates further studies.
Moreover, these findings strengthen the hypothesis that late outgrowth EPCs are “real” EPCs,17 referring to the population detected by FACS. The results of population doublings analyses argue in favour of the isolation of progenitor cells in our samples of EPCs regarding their high proliferative capacity.
Our data, performed on a large sample size of patients with SSc, according to recent recommendations, revealed higher levels of circulating EPCs defined as Lin–/7AAD–/CD34+/CD133+/VEGFR-2+ cells compared with controls. Levels of CD133+/VEGFR-2+ and CD34+/VEGFR-2+ cells, also considered in previous studies as putative EPCs,25 26 were significantly higher in patients with SSc as well, highlighting the robustness of our main conclusion. However, levels of Lin–/7AAD–/CD34+/CD133+ cells in patients with SSc and controls did not differ; thus, there was no evidence of impaired haematopoiesis in patients with SSc13 and only cells with endothelial phenotype (expressing the surface marker VEGFR-2) seem to be increased.
These high EPC levels are consistent with an increased EPC mobilisation from bone marrow during the disease. We also found that low EPC number was associated with the higher Medsger’s severity score and the presence of past and/or current digital ulcers. EPC levels were also lower in patients with PAH, but the difference was not significant. The limited number of patients with PAH (n = 3/50) in this study may account for this absence of significance. Thus, further analysis with a larger sample size is warranted to confirm this association. Taken together, these data suggest their recruitment in ischaemic tissues and sites of injury during active vascular lesion or severe disease. These data should not be regarded as in contradiction with those of Kuwana et al. who reported depletion of circulating EPCs13 in 11 patients with SSc, many of whom with active and severe disease. Our results also support previous findings suggesting EPC depletion in other vascular diseases, as atherosclerosis.27 28 Taken together, these results suggest that SSc could be associated with EPC mobilisation, but, in active or severe stages, EPC may be recruited at injured sites and thus decrease in the circulation.
SSc is characterised by tissue hypoxia and chronic ischaemia8 and is associated with major disturbances in the vascular system. Prognosis depends mostly on the severity of vascular lesions,29 and endothelial cells seem to be an initial target of the disease.30 31 Work with animal models has shown that endothelial cell apoptosis could be a primary event in the pathogenesis of SSc.32 33 In humans, only dermal microvascular cell anomalies34 have been described because of the difficulty of accessing human tissues; therefore, preventing rigorous analysis of endothelial cells. Thus, SSc EPCs may offer a potential cellular model to investigate endothelial biology. Further analyses are now warranted to study the differentiation ability toward mature endothelial cells and the functional characteristics of late outgrowth-EPCs in SSc.
Subsequently, if EPCs are shown to be functional, EPCs may offer potential therapeutic approaches involving EPC mobilisation by granulocyte colony stimulating factor,35 statins36 or erythropoietin,37 38 or reparative therapy, as observed in diabetic ulcers.35 Moreover, it was recently highlighted that human blood-derived EPCs displayed in vivo vasculogenic potential.39 This may allow the use of EPCs in SSc to form vascular networks in ischaemic tissues.
Conclusions and perspectives
We investigated EPCs in patients with a disease characterised by major vascular disturbances. Flow cytometry analysis performed according to recent recommendations allowed the identification of a population of circulating EPCs associated with the emergence and number of late outgrowth EPC-derived colonies, defining a new reliable biomarker. We found high EPC levels in SSc and an association between EPC number and disease severity, suggesting their general mobilisation but increased homing during severe disease. Further dedicated investigations are now required to evaluate their predictive value as a biomarker. As endothelial cell disturbances are crucial in SSc; isolated late outgrowth EPC-derived endothelial cells may provide a cellular model for further investigations of endothelial biology.
REFERENCES
Footnotes
Funding: Société Française de Rhumatologie, Institut SERVIER, Association des Sclérodermiques de France, Groupe Français de Recherche sur la Sclérodermie, Fondation pour la Recherche Médicale, Institut National de la Santé Et de la Recherche Médicale, Fond d’Etude et de Recherche du Corps Médical des Hôpitaux de Paris
Competing interests: None.