



Asthma and suicide-related adverse events: a review of observational studies
- *Centre for Paediatric Pharmacy Research, The School of Pharmacy, University of London, #Institute of Child Health, University College London, and ¶Institute of Psychiatry, King’s College London, London, UK. +Dept of Pharmacology and Pharmacy, Li Ka Shing Faculty of Medicine, The University of Hong Kong, Pokfulam, Hong Kong.
- I.C.K. Wong, Dept of Pharmacology and Pharmacy, Li Ka Shing Faculty of Medicine, The University of Hong Kong, Pokfulam, Hong Kong. E-mail: wongick{at}hku.hk
Abstract
Suicide is a major public health concern. There are several risk factors associated with suicide. Chronic illnesses, such as asthma, have been linked to an increased risk of suicide-related events. This study reviews the evidence of an association between asthma and suicide using published epidemiological observational studies.
An electronic search using PubMed and EMBASE was performed. Studies that investigated the association of asthma with suicide-related behaviour were selected. Studies were examined to form a descriptive analysis.
Six observational studies met the selection criteria, of which at least one suicide-related adverse event was studied. Three studies investigated completed suicide, two suicide attempts and four suicide ideation. Two of the studies focused on individuals aged <18 yrs.
Evidence from observational data support the hypothesis of an association between asthma and suicide-related behaviour (ideation, attempts and completion); however, epidemiological studies, with more objective measures and larger sample sizes, adjusting for a wider scope of suicide-related confounding factors (e.g. comorbidities), and with a longitudinal design, are needed for a more conclusive answer.
- Asthma
- attempt
- ideation
- review
- suicide
Suicide is a major public health issue worldwide. The World Health Organization (WHO) reports that nearly one million people die due to suicide each year, with a global mortality rate of 16 deaths per 100,000 or one death every 40 s. It is the 14th leading cause of death worldwide and accounts for 1.5% of all deaths [1]. The suicide rates in the UK in 2009 were recorded as 17.7 and 5.2 per 100,000 in males and females, respectively [2]. In England there is an average of one person dying every 2 h as a result of suicide and it is one of the top three leading causes of death in people aged 15–34 yrs in the UK [3].
In order to decrease the burden and prevent suicides there needs to be an understanding of factors that increase the risk of suicidal behaviour. Several risk factors exist including demographic, psychiatric, psychological and biological factors [4]. Increased suicidal thoughts and behaviour are more common in chronic physical illness, and increased suicidal ideation is associated with conditions such as asthma, even in the absence of depression [5–10].
Asthma is one of the most common chronic diseases among children, with approximately one in 11 children suffering from asthma in the UK [11]. On average, four people per day or one person every 7 h dies from asthma in the UK [12]. The WHO estimates that there are currently 300 million people suffering from asthma and asthma is also estimated to account for ∼250,000 deaths per year worldwide [12, 13]. Asthma can have a significant effect on quality of life, and consequences include sleeplessness, daytime fatigue, reduced activity levels, school and work absenteeism, and mental health problems [14–16]. It is hypothesised that asthma is a risk factor associated with suicidal behaviour. The question of whether such an association exists is particularly important because of recent concerns about the possible effects of some types of asthma treatment on suicide risk [17, 18]. The aim of this article is to systematically search, identify and review evidence in the literature of an association between asthma and suicidal behaviour (suicide ideation, attempt and completion) in the general population.
METHODS
Two investigators (N. Iessa and M.L. Murray) carried out an electronic search of bibliographic databases. The search strategy included the following terms: Suicide OR suicidal OR self harm AND Asthma OR cough OR respiratory disease OR wheez*. This strategy was inputted into PubMed (Medline 1966 to March 2011) EMBASE (1980 to March 2011) and International Pharmaceutical Abstracts (1970 to August 2010). No limits relating to language, age, type of article or date were imposed. The search was last updated on February 18, 2011. The study criteria included all epidemiological observational studies (cohort, cross-sectional and case controlled) for all population groups (adults and children). The outcome measures for suicidal behaviour were defined as suicide ideation, suicide attempts, self-injury and death by suicide. Studies that did not investigate asthma and suicide specifically were excluded.
There is some ambiguity with defining terms related to suicide and suicidal behaviour, making it difficult to compare studies and conduct a meta-analysis [19]. Most clinicians and researchers distinguish suicidal behaviour from non-suicidal self-injury, i.e. self-injury in which a person has no intention of dying. A suicide plan is the formulation of a specific method through which one intends to die and suicide attempt refers to engagement in potentially self-injurious behaviour in which there is at least some intent to die.
Articles generated from the search were combined using a reference tool (Reference Manager® 11.0; Thomson Researchsoft, New York, NY, USA). Duplicates were removed and titles and abstracts of articles were screened for relevance by two reviewers (N. Iessa and M.L. Murray). Potentially relevant articles were obtained in full and further screened to determine if they met inclusion criteria. Data from the articles were summarised in terms of study population, outcome measures, settings, and data collection and limitations to form a descriptive analysis.
RESULTS
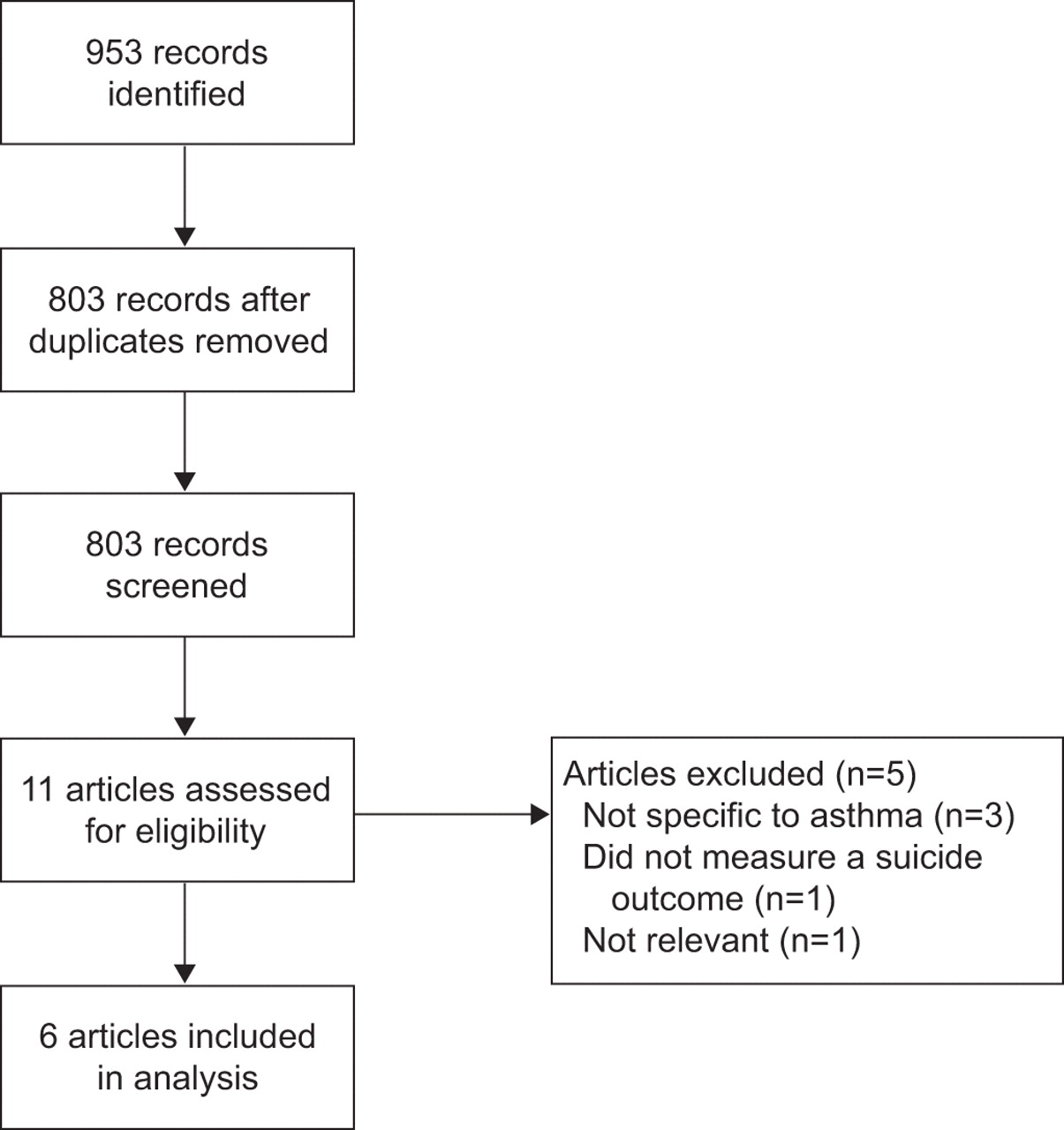
After removal of duplicate articles a total of 803 articles were generated by the electronic search (fig. 1).
{kind=link}
Results of electronic search.
Selection of studies
After screening abstracts and titles, 11 articles were identified as potentially relevant and full texts were obtained. Three articles were excluded because they were not specific to asthma as an exposure [7, 8, 20]. One article was excluded as it did not measure suicide as an outcome and another article consisted of a series of cases where asthma was speculated to be a tool to commit suicide [21, 22]. Six articles met the inclusion criteria [5, 10, 23–26]. Table 1 summarises data extracted from the studies and compares methodology, outcomes and limitations of each of the studies.
Summary of studies included
Study population
Three studies were carried out in adults aged >18 yrs [5, 24, 25]. Two studies were conducted in youths aged 9–17 yrs [23] and 11–16 yrs [10], and one study with both adults and children [26].
Outcome measures, measurements and data collection
Adults
Clarke et al. [24] list the two main outcomes of interest as suicide ideation and suicide ideation with suicide attempt. Other variables measured were socio-demographics and history of depression, anxiety, alcohol abuse and nicotine dependence. Goodwin and Eaton [5] used suicide ideation and attempts as primary outcomes at two time-points (waves) 1 yr apart, followed by deaths due to suicide and depression at the third time-point at 15 yrs follow-up. In another study by Goodwin et al. [25], the primary outcomes included suicide ideation as well as major depression, panic attacks, generalised anxiety disorder, alcohol and drug use disorder.
Adults and youths
The study conducted by Qin et al. [26] used completed suicide as an outcome measure obtained from the danish cause of death registry.
Youths
A study carried out in Taiwan by Kuo et al. [10] had death due to suicide as its primary outcome. Other outcomes included natural death and cause of deaths. Suicide ideation and attempts were not measured. In a study by Goodwin and Marusic [23], suicide ideation was the primary outcome assessed through questioning, other measures included; information on child psychiatric diagnosis; psychotropic medication use and mental health treatment; general functioning; family history of psychopathology; medication use and environmental risk and protective factors; physical health; social competence; educational aspiration; parental relationships; adverse life events; and socioeconomic status.
Suicide ideation
Suicide ideation was mainly assessed through interview questions. Clarke et al. [24] determined suicide ideation through data obtained from the National Comorbidity Survey-Replication (NCS-R). The NCS-R survey was a national survey of people aged ≥18 yrs carried out in 2001–2003. It was a fully structured interview that was administered face to face by trained lay interviewers. It assessed 12-month occurrence of suicide ideation from baseline.
Suicide attempt
Two studies measured suicide attempt; Goodwin and Eaton [5] interviewed patients asking “have you ever attempted suicide?” and Clarke et al. [24] used the NCS-R survey results.
Completed suicide
Three studies included completed suicide as an outcome measure. Goodwin and Eaton [5] linked patients to the National Death Index in the USA, Kuo et al. [10] used the Department of health death certification system (National Mortality Database) in Taiwan and Qin et al. [26] identified deaths using the Danish cause of death registry.
Setting and study design
Five of the studies used large population data [5, 10, 24–26] and one recruited patients prospectively from a primary care clinic [23]. The majority of studies gave a cross-sectional overview with the exception of two studies. One study was based on the entire population to perform a nested case–control design [26] and the second observed suicide ideation, attempts and deaths longitudinally in addition to cross-sectionally [5].
Four out of the six studies were carried out in the USA [5, 23–25], one was carried out in Taiwan [10] and one in Denmark [26].
Diagnosis of asthma
Goodwin et al. [25] used physician-based diagnosis obtained from billing records to identify patients with asthma. Other studies obtained information from the patients and/or parents of patients (among the youths) by means of interviews or through a video and written questionnaire. Examples of interview questions were as follows: “Have you ever had asthma?” and “Do you have asthma now?” [5]; “Did a doctor or other health professional ever tell you that you had asthma?” [24]; and “Has your child ever had asthma?” [22]. In the study by Qin et al. [26], the Danish General Hospital Registry was used to retrieve personal history of hospital contacts with allergic illness as a primary diagnosis. Under this umbrella, asthma codes were used to detect patients with allergic rhinitis and bronchial asthma [26].
Risk factors for analysis
All studies were adjusted for socio-demographic factors such as age, race, ethnicity and sex. Other comorbidities were also measured in different studies. Clarke et al. [24] measured lifetime depression, anxiety, alcohol abuse, nicotine dependence and smoking status. Goodwin and Marusic [23] measured child psychiatric diagnosis, psychotropic medication use and mental health treatment, general functioning, family history of psychotropic medication use and mental health treatment, family history of psychopathology environmental risk and protective factors. Kuo et al. [10] measured cigarette smoking of family members and allergic rhinitis. The studies by Goodwin and co-workers [5, 25] measured major depression and mental disorders, respectively. Qin et al. [26] measured whether patients had a history of mood disorder. The authors also made adjustments for mood disorders in allergic patients, but not for the strata of patients with asthma and allergy.
Association between asthma and suicide
All studies showed an association with the suicide-related outcome measured and asthma, even after adjusting for potential confounders. Clarke et al. [24] showed that asthma was significantly (p<0.001) associated with suicide ideation and attempts but not with suicide ideation alone. This remained statistically significant after adjusting for smoking, depression, panic disorder and alcohol abuse. In the study by Goodwin and Eaton [5], asthma significantly increased the odds of suicide ideation (OR 2.33, 95% CI 1.03–5.25) and suicide attempt (OR 3.54, 95% CI 1.4–8.99). Asthma increased the likelihood of suicidal ideation (OR 1.9, 95% CI 1.03–3.4) after controlling for comorbid disorders in another study by Goodwin et al. [25]. In youths, Kuo et al. [10] showed that the incidence rate of suicide mortality in participants with current asthma to baseline was more than double that of those without asthma (11.0 versus 4.3 per 100,000 person-yrs). Qin et al. [26] showed an incidence rate ratio (IRR) of 1.66 (95% CI 1.46–1.89) in those who that had allergy rhinitis with bronchial asthma and who were in-patients. However, outpatients did not show a significant IRR. Goodwin and Marusic [23] showed that asthma was associated with a significantly increased likelihood of suicide ideation (OR 3.25, 95% CI 1.04–10.1), compared with youths without asthma.
DISCUSSION
The studies suggest an association between asthma and suicide ideation and attempts in adults, suicide ideation in children, and completed suicide in both adults and children. This association remained evident after adjusting for socio-demographic factors in all studies. For studies that made adjustments for confounding by comorbidities such as major depression, mental disorders and environmental factors such as smoking, the association was reduced, but remained significant, indicating an independent association between asthma and suicidal behaviour.
The reasons for an association between suicidal behaviour and asthma are not clear. Possible factors include mood changes and anxiety that result from the disability and discomfort associated with asthma. Individuals might have frequent thoughts of death with increasing severity because they have a potentially life-threatening disease [14]. Other explanations include a link to the production of pro-inflammatory cytokines during the allergy process [29]. Expression of these cytokines can result in inhibition, sexual behaviour and food intake [30, 31]. In addition, activation of T-helper type 2-related cytokines can lead to insomnia and sleep loss.
Although all six studies have provided evidence of an association between a form of suicidal behaviour and asthma, more evidence is needed. The studies varied in the categorisation of measured outcomes (death by suicide, suicide attempt and ideation). Only one study, that reported by Goodwin and Eaton [5], attempted to include all three outcomes within a single study. This included completed suicides, although the size of the study population and consequent number of deaths by suicide were too small to provide a conclusive association. Hence, more studies with a larger population size are needed to address the incidence of completed suicide and asthma. In youths, suicide ideation and deaths have been examined but no studies have addressed suicide attempts.
Four out of the six studies limited their investigations to cross-sectional data, which does not provide information on the sequence of the onset of disorders. The study by Goodwin and Eaton [5] consisted of three time waves providing a follow-up in order to provide a longitudinal prospective. This approach showed a link between suicide ideation and attempts; however, this link was not statistically evident and varied in strength with differing time-periods. The authors attribute this to a small sample size. Qin et al. [26] used population data found in hospital registries. This provided a longitudinal insight; however, data was only available only from when the registry data became available, hence the whole lifetime data for older subjects were not obtained. The cross-sectional design of the other studies did not allow the sequence of outcomes in relation to exposure dates to be measured.
All studies made adjustments for socio-demographic factors, but they varied in adjustments for other confounding effects. Mental disorders, the presence of major depression and smoking were the main confounders considered. Goodwin and Eaton [5] considered asthma treatment and investigated whether treatment of asthma was associated with increased likelihood of suicide ideation and attempt. However, information on specific forms of asthma treatment, as well as frequency and timing of treatment initiation, was limited. Not all studies had measured baseline depression and anxiety. Conclusions regarding the impact of medication use on the risk of suicide ideation and attempts could not be drawn from the data.
Asthma varies in severity and can often lead to hospitalisation. It is thought that depression, anxiety and other adverse psychological factors increase with asthma severity, particularly if the patient is admitted to hospital [24, 32–34]. Qin et al. [26] attempted to address different severities of asthma and allergies by examining completed suicides in patients in both outpatient and in-patient settings. There was no evidence of a significant risk of suicide in patients with allergy rhinitis and bronchial asthma who had outpatient appointments. In the other studies, evidence in the literature does not account for different severities of asthma when examining an association with suicidal behaviour, which is a potential confounder. Other possible confounders not accounted for include genetic and environmental factors, such as the occurrence of an adverse life event. The possible relationship between conditions such as attention deficit hyperactivity disorder and atopic diseases (asthma and rhinitis eczema) is another potential factor to consider in studies investigating suicide-related adverse events [35–39]. Asthma may potentially affect the quality of life experienced by youths and adults in several ways: psychological (self-esteem, social participation or parental over protection); growth and development (short stature or delayed puberty); comorbidity with clinical levels of anxiety and depression [40].
Methodological limitations of previous studies
Lack of standard definitions for suicide-related behaviour remains a methodological problem when comparing studies, despite attempts to form a consensus. “Suicidality” is not thought to be clinically useful and more specific terminology, such as suicide ideation or suicide attempts, are preferred [41]. In the studies identified in this review, there was no indication of how investigators diagnosed and measured suicide ideation. The questions with regard to suicide asked by interviewers varied between studies. Despite advancements in the definition and nomenclature of suicide-related behaviours, limitations exist due to measurement variability.
All studies were limited by their method of data collection. Asthma diagnosis was determined by self-reporting made by subjects and/or their parents with the exceptions of the studies by Goodwin et al. [25] and Qin et al. [26], in which asthmatic diagnosis was obtained from data recorded as International Classification of Diseases codes for the purpose of billing patients and a hospital database, respectively. No objective respiratory measures or data on lung function (e.g. spirometry) were taken. Self-reporting of asthma diagnosis may provide a source of recall bias. However, Goodwin and Marusic [23] comment that the method used to determine international prevalence rates of asthma is widely used and accepted, making it comparable to other national and cross-national studies.
Data of deaths by suicide were collected by linking patients to the Department of health death certification system in Taiwan and the National Death Index in the USA in the studies by Kuo et al. [10] and Goodwin and Eaton [5], respectively. A limitation of this is that other causes of death (e.g. accidental) may have been substituted for suicide in records to avoid any potential stigma associated with suicide.
This review highlights the need for further well-designed epidemiological studies that investigate the association of asthma and suicide-related adverse events. The use of databases with anonymised electronic patient records can provide large datasets, often representing the general population, and thus is suitable for detecting rare events such as suicide.
Conclusion
Studies investigating the association between suicide behaviour and asthma support the hypothesis of an association. However, studies with more objective measures adjusting for a wider variety of confounders including medication, measuring all suicide-related outcomes and varying exposure levels (severity of asthma), and taking into account the sequence of diagnosis (longitudinal design) are needed for a more conclusive answer. More evidence with larger population sizes is needed to investigate the association of death by suicide and asthma.
Footnotes
Provenance
Submitted article, peer reviewed.
Statement of Interest
None declared.
- Received June 8, 2011.
- Accepted June 24, 2011.
- ©ERS 2011