





Abstract
Background COPD and adult-onset asthma (AOA) are the most common noncommunicable respiratory diseases. To improve early identification and prevention, an overview of risk factors is needed. We therefore aimed to systematically summarise the nongenetic (exposome) risk factors for AOA and COPD. Additionally, we aimed to compare the risk factors for COPD and AOA.
Methods In this umbrella review, we searched PubMed for articles from inception until 1 February 2023 and screened the references of relevant articles. We included systematic reviews and meta-analyses of observational epidemiological studies in humans that assessed a minimum of one lifestyle or environmental risk factor for AOA or COPD.
Results In total, 75 reviews were included, of which 45 focused on risk factors for COPD, 28 on AOA and two examined both. For asthma, 43 different risk factors were identified while 45 were identified for COPD. For AOA, smoking, a high body mass index (BMI), wood dust exposure and residential chemical exposures, such as formaldehyde exposure or exposure to volatile organic compounds, were amongst the risk factors found. For COPD, smoking, ambient air pollution including nitrogen dioxide, a low BMI, indoor biomass burning, childhood asthma, occupational dust exposure and diet were amongst the risk factors found.
Conclusions Many different factors for COPD and asthma have been found, highlighting the differences and similarities. The results of this systematic review can be used to target and identify people at high risk for COPD or AOA.
Abstract
This umbrella review provided an overview of nongenetic risk factors for both COPD and adult-onset asthma. Commonly found factors included smoking, BMI, air pollution, early life exposures and occupational exposures. https://bit.ly/3kyeWZL
Background
COPD is one of the most common chronic respiratory disorders, with a prevalence ranging from 3.6 to 10.1% [1, 2] Currently, COPD is the third leading cause of death worldwide [3], with 2–6% of global disability-adjusted life years attributed to COPD in 2015 [4]. Additionally, COPD patients are at an increased risk of developing extrapulmonary manifestations or comorbidities that highly affect disease burden, such as cardiovascular diseases and lung cancer [5, 6, 7]. Besides COPD, another 300 million children and adults globally are estimated to be suffering from asthma [8]. Even though adult-onset asthma (AOA) is less studied than childhood asthma, previous research shows that incidence has been rising over the past two decades [9]. For example, de Marco et al. [10] showed asthma prevalence in Italy to have increased by 38% between 1991 and 2010, irrespective of age. Distinguishing between COPD and asthma can be difficult, especially in older adults, as the predicted forced expiratory volume in 1 s falls to 50% in both asthma and COPD patients over 60 years old [11]. Some patients with asthma develop COPD later in life and some patients with COPD show clinical features commonly observed in asthma [12]. For patients who show characteristics of both COPD and asthma, the label asthma–COPD overlap syndrome (ACOS) is being considered [13]. It has been widely reported that patients suffering from ACOS have worse disease outcomes, such as more exacerbations and a more rapid decline in lung function, than patients suffering from only asthma or COPD [13, 14, 15]. As there is considerable overlap between the two conditions, this could mean overlapping risk factors as well.
As both COPD and AOA have a high disease burden, and there is no curative treatment for COPD [16], early identification and prevention are key. To optimise prevention strategies, a better understanding of especially nongenetic risk factors for developing either condition is needed. Additionally, risk factors for childhood asthma are well established, but it is unclear how those risk factors translate to AOA. Furthermore, previous research has shown similarities in nongenetic risk factors for developing either COPD or AOA, such as smoking and high exposure to air pollution [17]. However, to our knowledge, there is currently no overview comparing risk factors for COPD and asthma. The aim of this systematic umbrella review is to provide an overview and comparison of all nongenetic risk factors for COPD and AOA, identifying similarities as well as differences.
Methods
Search strategy
We conducted an umbrella review, a systematic collection and assessment of multiple systematic reviews and meta-analyses [18]. The review was conducted according to the study protocol, registered in the International Prospective Register of Systematic Reviews (PROSPERO-CRD42021284614) and according to PRISMA guidelines. The full PRISMA checklist can be found in the supplemental material.
PubMed was systematically searched from inception to 1 February 2023 to identify systematic reviews and meta-analyses of studies examining one or multiple nongenetic risk factors for either COPD or AOA. The search strategy consisted of terms on COPD, asthma, epidemiology, aetiology, risk factors and study design (full search strategy in the supplemental material). In addition, reference lists of included papers were screened for additional relevant reviews that might have been missed during the initial search. A first screening was independently done by two researchers (J.C.S.H. and L.D.B.) based on title and abstract. Subsequently, the full text of all relevant articles was assessed for eligibility by one researcher (J.C.S.H.), with an additional researcher (M.E.B.C.) assessing a random 10% of the articles. Initial discrepancies were first discussed amongst the reviewers with a third reviewer (R.J.H.C.G.B.) being available for final decision making in case of disagreement. However, this did not occur.
Inclusion and exclusion criteria
Systematic reviews with or without meta-analyses of observational epidemiological studies, including systematic reviews of Mendelian randomisation studies, in humans that assessed nongenetic risk factors for incidence asthma or COPD were included. Regarding AOA, reviews were included regardless of specifying age of onset. Only studies available in English were included. Studies examining risk factors for either mortality, exacerbations or management of either disease were excluded. Additionally, studies examining the impact of another disease on development of either COPD or AOA were considered noneligible. When multiple analyses or reviews included the same original studies, the most recent one was included.
Data extraction
Data extraction was performed by one reviewer (J.C.S.H.), with a second reviewer (M.E.B.C.) extracting data from a random 10% for quality control purposes. From each eligible article, the authors, year of publication, examined nongenetic risk factor(s), examined outcome, number of epidemiological studies included, the total number of participants per review and the main conclusions were recorded. Additionally, for AOA it was recorded whether age of onset was specified. Study quality and risk of bias of the included reviews was checked by applying the Joanna Briggs Institute (JBI) checklist for systematic reviews and research synthesis [19]. Scores were given for every included aspect, resulting in a score ranging from 1 (poorly conducted) to 11 (well conducted). For studies without a meta-analysis, the maximum score is 10.
Results
Literature review
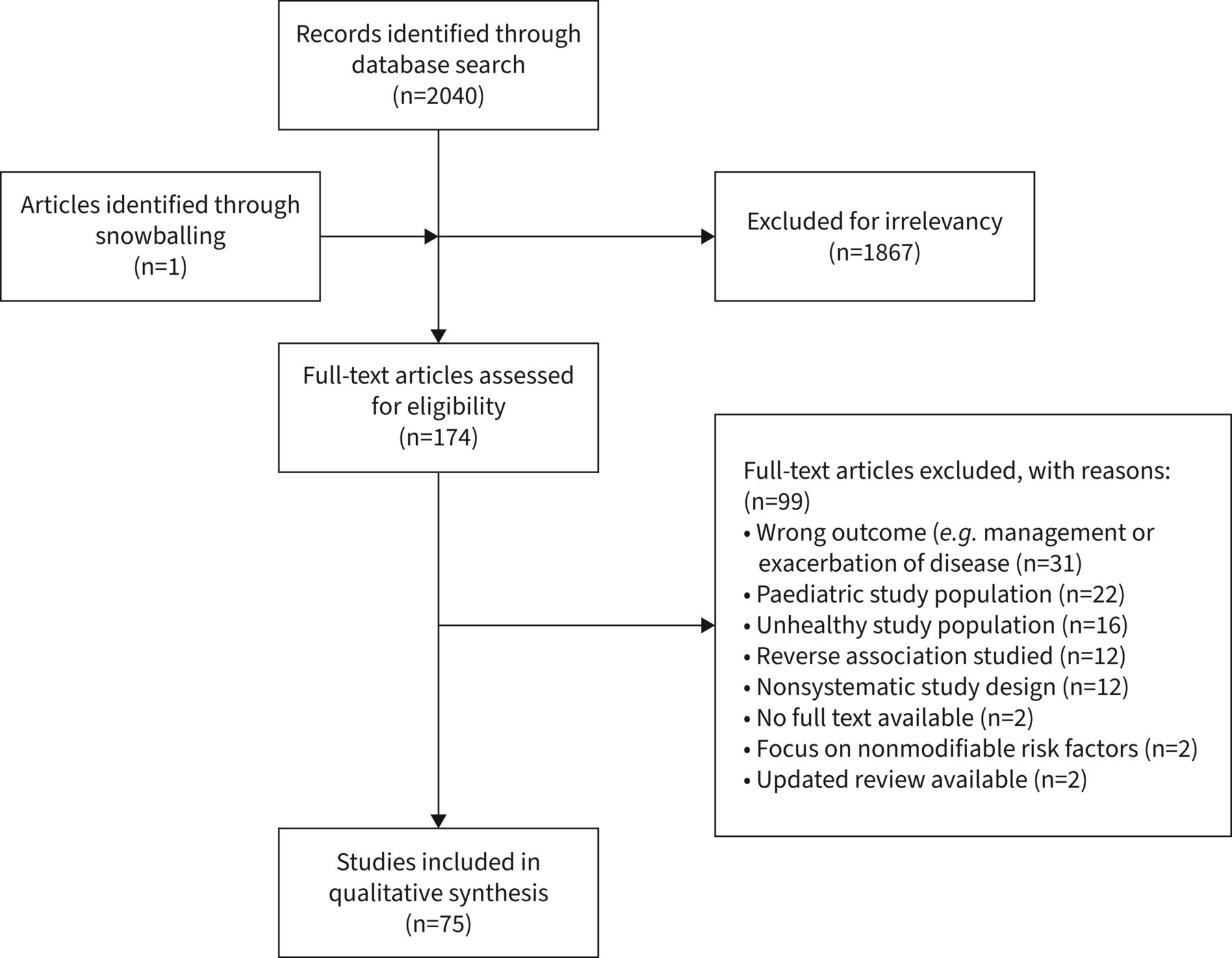
Our literature search identified 2040 publications. Of those, 1867 were excluded following title and abstract review (figure 1), mainly because they focused on genetic risk factors or on exacerbations or management of disease. Additionally, one review was identified through snowballing. Of those, 99 were excluded after reviewing the full texts, resulting in 75 eligible articles included in this umbrella review. Of these, 45 focused on risk factors for COPD, 28 on asthma and two reviews included both COPD and asthma. Out of the 75 included reviews, 45 included a meta-analysis and narrative review, 12 conducted only a meta-analysis but no narrative review and 18 only included a narrative review.

{kind=link}
Results of the searches, screening and data extraction.
Regarding AOA, 47 of the included studies mentioned COPD, addressing 45 different risk factors. A selection of characteristics of the included articles are described in tables 1 and 2 for AOA and COPD, respectively. Full characteristics are shown in tables S1 and S2. A summary of the found risk factors and their corresponding effect sizes is shown in tables 3 and 4, respectively. For both AOA and COPD, the JBI scores ranged between 5 and 11. For AOA, age of onset was not clear for all papers, with only seven specifying AOA. An additional four compared exposed versus nonexposed individuals within occupational settings, implying adult-onset. All were included, but this uncertainty was noted. When a meta-analysis was conducted, the meta-results are given as opposed to single-study results.
Characteristics of 30 included systematic reviews for adult-onset asthma, ranked by Joanna Briggs Institute (JBI) score
Characteristics of 47 included systematic reviews for COPD, ranked by Joanna Briggs Institute (JBI) score
Overview of the identified risk factors for adult-onset asthma, and their corresponding effect sizes
Overview of the identified risk factors for COPD and their corresponding effect sizes
Asthma
Air pollution and chemical exposures
Eight reviews identified either chemical exposures or air pollution as risk factors for asthma [21, 27, 31, 38, 43, 46, 47, 49]. Sio and Chew [31] identified exposure to several types of air pollution, including nitrogen dioxide (NO2), particulate matter and ozone as risk factors for AOA, with included pooled odds ratios (ORs) ranging between 1.03 and 1.22. Yu et al. [21] reported that high indoor residential formaldehyde exposure (>22.5 µg·m−3) was associated with an increased risk of asthma as compared to low exposure (≤22.5 µg·m−3), with a meta OR (mOR) of 1.81 (95% CI 1.18–2.78). Moreover, Nurmatov et al. [27] reported that domestic exposure to volatile organic compounds (VOCs), i.e. aromatic VOCs, chlorinated hydrocarbons, propylene glycol and glycol ethers, alkanes, alcohols, aldehydes, ketones, and terpenes, increased asthma risk. Doust et al. [46] reported both occupational and nonoccupational pesticide exposure to increase asthma risk. However, there was variation in pooled estimates for pesticide exposure, ranging from 0.41 (95% CI 0.15–1.11) to 3.67 (95% CI 1.19–11.30) for exposed versus nonexposed, with inconsistent reporting on the type of pesticide examined. Jaakkola and Knight [47] found a high exposure to phthalates, such as heated polyvinyl chloride fumes, increased asthma risk, with an mOR of 1.55 (95% CI 1.18–2.05). Canova et al. [43] found that domestic paint use was associated with asthma, with one study providing an OR of 1.60 (95% CI 1.00–2.50). The final two reviews did not find either consistent or significant results. Vincent et al. [49] did not find significant associations between exposure to cleaning products and an increased risk of asthma. The review by Kakutani et al. [38] did not show arachidonic acid intake to be consistently associated with asthma.
Early life exposures
Four reviews identified early life factors as risk factors for asthma later in life [26, 29, 41, 45]. First, a review by Flaherman and Rutherford [45] identified that both a high weight during middle childhood (body mass index (BMI) ≥85th percentile for age and gender) (mOR 1.32, 95% CI 0.82–2.40) and high birth weight (≥3.8 kg) (mOR 1.26, 95% CI 0.88–1.82) could increase the risk of asthma. Jaakkola et al. [41] identified pre-term delivery as a possible risk factor, with ORs of included studies ranging between 1.86 (95% CI 0.23–12.00) and 1.14 (95% CI 0.92–1.40). However, these results were not statistically significant. Mu et al. [29] reported low birth weight to be a risk factor, with a birth weight of <2500 g to be associated with a higher risk of asthma (mOR 1.25, 95% CI 1.12–1.40) as compared to babies with a birth weight between 2500 and 4000 g. Lastly, Shen et al. [26] studied early life vitamin D deficiency and risk of asthma later in life, but found no statistically significant association (mOR 0.57, 95% CI 0.35–0.93).
Nutrition and weight status
Four reviews focused on nutritional or weight-related risk factors [23, 31, 40, 42]. Beuther and Sutherland [40] found that compared to a healthy BMI, overweight and obese participants had mORs of 1.38 (95% CI 1.17–1.62) and 1.92 (95% CI 1.43–2.59) for developing asthma, respectively. This is in accordance with Sio and Chew [31], who found an mOR of 2.02 (95% CI 1.63–2.50) for participants with a BMI of ≥30 kg·m−2. Additionally, Mikkelsen et al. [42] found a meta risk ratio (mRR) of 1.05 (95% CI 1.03–1.07) per kg·m−2 increase in BMI. Chen et al. [23] identified lower zinc and selenium plasma levels as possible risk factors for asthma, with a standardised mean difference (SMD) between asthma patients and healthy controls of −0.26 (95% CI −0.40–−0.13) for zinc and −0.06 (95% CI −0.13–0.02) for selenium. However, they did not provide which unit they standardised to.
Occupational exposures
Six reviews examined occupational risk factors for asthma [20, 25, 30, 34, 44, 48]. Romero Starke et al. [20] focused on healthcare workers exposed to cleaning products with an mRR of 1.67 (95% CI 1.11–2.50) among nurses exposed to different types of cleaning products compared to unexposed nurses. Folletti et al. [48] also reported cleaning workers to be at an increased risk, with ORs of the included studies ranging between 1.50 and 3.00. Baur et al. [44] reported exposure to workplace irritants, such as chloride, led to an increased asthma risk. Wiggans et al. [34] reported wood dust exposure in wood workers to increase asthma risk, with only one study providing a risk ratio of 1.53 (95% CI 1.25–1.87) as compared to the general population. Furthermore, Zhang et al. [25] identified exposure to organic dust when compared to healthy individuals to increase asthma risk in different occupations. They found associations with paper/wood dust (mOR 1.62, 95% CI 1.38–1.90), flour/grain (mOR 1.48, 95% CI 1.11–1.97) and textile dust (mOR 1.50, 95% CI 1.08–2.09). Lastly, Macan et al. [30] found that exposure to persulphates, such as hair bleach, was associated with asthma in hairdressers.
Physiological, personal and socioeconomic characteristics
Of the included reviews, 11 studied either physiological, personal, or socioeconomic risk factors [22, 24, 28, 31–33, 35–37, 39, 42]. Wang et al. [22] examined exposure to greenness as a risk factor for asthma, but found contradicting results, with one of their included studies finding an increased asthma risk, one finding exposure to greenness to be a protective factor and one not showing an association. Etminan et al. [24] found acetaminophen use was associated with an increased risk of asthma when compared to nonexposed individuals (mOR 1.63, 95% CI 1.46–1.77). Four studies focused on aspects of the home environment [28, 31, 32, 39]. The first, by Rodriguez et al. [32], compared participants living in urban environments to participants in rural environments and found people living in urban areas to have an increased asthma risk (mOR 1.89, 95% CI 1.47–2.41). The second, by Sharpe et al. [28], reported that exposure to indoor fungi from the Penicillium, Aspergillus and Cladosporium species, could increase asthma risk when compared to individuals with lower exposure. However, an OR was only given for one of the included studies (1.25, 95% CI 0.99–1.58). The third, by Takkouche et al. [39], examined having furry pets indoors as a risk factor for asthma and found an mOR for exposure to any pet of 1.58 (95% CI 0.99–2.54). The fourth, by Sio and Chew [31], found household factors such as mould to be associated with asthma, with ORs of the included studies ranging between 1.43 and 1.73. Cong et al. [33] investigated the effect of ambient temperature drops on asthma risk, per 1°C decrease, but found no significant results (mOR 1.00, 95% CI 0.93–1.08). Furthermore, Uphoff et al. [35] found a lower socioeconomic status (SES) to be associated with increased asthma risk (mOR 1.38, 95% CI 1.37–1.39). Tan et al. [36] reported that participants with late-onset asthma were more likely to be female (58–75%) and smokers (56%), while Sio and Chew [31] found males to be at an increased risk (mOR 1.30, 95% CI 1.23–1.38). Both Mikkelsen et al. [42] and Sio and Chew [31] examined smoking as a risk factor, with the former finding it a protective factor (risk ratio 0.97, 95% CI 0.96–0.99) and the latter finding an association with an increased asthma risk (mOR 1.66, 95% CI 1.44–1.90). However, Mikkelsen et al. [42] only included two papers on smoking, with the other included paper finding smoking to be associated with an increased asthma risk. Additionally, Sio and Chew [31] found an association with second-hand smoke exposure (mOR 1.44, 95% CI 1.30–1.60) [31]. Mikkelsen et al. [42] found early as compared to average age at puberty to be a risk factor (mRR 1.37, 95% CI 1.15–1.64), where late versus average age at puberty was found to be a protective factor (mRR 0.93, 95% CI 0.90–0.96) [42]. Lastly, Lieberoth et al. [37] found a younger age at menarche to be associated with asthma risk (mOR 1.37, 95% CI 1.15–1.64).
COPD
Air pollution and chemical exposures
We identified 19 reviews, studying six different risk factors [46, 54, 57, 60, 61, 64, 69, 70, 72, 76, 77, 79, 81–83, 85, 86, 93, 94]. Park et al. [60] found an association between exposure to ambient fine particulate matter (PM2.5) and COPD (meta hazard ratio (mHR) 1.18, 95% CI 1.13–1.23) per 10 μg·m-3 increase, which was also found by Chen et al. [72] (mOR 1.73, 95% CI 1.16–2.58). Additionally, they found significant associations between NO2 and COPD, which was also found by Zhang et al. [82], with a 10 μg·m-3 increase in NO2 being associated with an mHR of 1.07 (95% CI 1.00–1.16) [60] and an mRR of 1.02, respectively. Indoor air pollution caused by indoor biomass burning was found to be a risk factor for COPD in several reviews [54, 57, 61, 69, 70, 72, 76, 77, 79, 81, 83, 85, 86, 93, 94]. Found mORs ranged between 1.52 (95% CI 1.39–1.67), found by Njoku et al. [61] and 3.16 (95% CI 1.82–5.49), found by Kamal et al. [69], when compared to unexposed controls. Doust et al. [46] identified both occupational and nonoccupational pesticide exposure as a possible risk factor, with ORs of the included studies ranging from 1.05 (95% CI 0.74–1.51) to 4.10 (95% CI 2.20–6.30) for exposed versus nonexposed individuals, with inconsistent reporting on the type of pesticide examined. Yang et al. [57] reported living in polluted areas, defined as areas with high levels of outdoor air pollution, as a risk factor for COPD, with an mOR of 1.63 (95% CI 1.20–2.21). Lastly, Ryu et al. [64] reported being exposed to vapours, gases, dusts and fumes to increase COPD risk (mOR 1.43, 95% CI 1.19–1.73).
Early life exposures
12 reviews identified risk factors in early life [50, 52, 57, 68, 70, 72, 80, 85, 92, 93, 94]. Six of these focused on respiratory problems in early life and COPD risk [50, 57, 72, 85, 93, 94], with found mORs ranging between 2.23 (95% CI 1.63–3.07) [50] and 3.44 (95% CI 1.33–8.90) [72]. Additionally, Duan et al. [50] identified childhood asthma (mOR 3.45, 95% CI 2.37–5.02), maternal smoking during both pregnancy and childhood (mOR 1.42, 95% CI 1.17–1.72), child maltreatment, e.g. physical abuse (mOR 1.30, 95% CI 1.18–1.42), and low birth weight (mOR 1.58, 95% CI 1.08–2.32) as risk factors for COPD. They did not find statistical significant associations for childhood environmental tobacco smoke exposure (mOR 1.30, 95% CI 0.83–1.61), which is in accordance with results found by Lee et al. [92] (mRR 0.88, 95% CI 0.72–1.07), or premature birth (mOR 1.17, 95% CI 0.87–1.58) [50]. Childhood asthma was found to be a risk factor by Sutradhar et al. [70], Ali [80] and Asamoah-Boaheng et al. [52], with, respectively, an OR of 6.90 (95% CI 4.90–9.50), an mOR of 3.00 (95% CI 2.25–4.00) and an mOR of 7.87 (95% CI 5.40–11.45). Lastly, Ma et al. [68] found childhood wheeze to increase the risk of COPD later in life (mRR 5.31, 95% CI 1.03–27.27).
Nutrition and weight status
10 reviews identified nutritional factors or weight-related aspects as risk factors for COPD [51, 57, 63, 72–74, 76, 78, 79, 85], of which five studies identified having a low BMI as a risk factor for COPD [57, 72, 74, 76, 85]. The found mORs ranged from 1.96 (95% CI 1.78–2.17), found by Zhang et al. [74], to 3.83 (95% CI 2.22–6.60), found by Yang et al. [57]. Additionally, Zhang et al. [74] found an association between COPD and overweight (mOR 0.80, 95% CI 0.73–0.87) and obese (mOR 0.86, 95% CI 0.73–1.02) participants, but found it to be a protective factor, which was also found by Adeloye et al. [85] (mOR 0.90, 95% CI 0.80–0.90). Chen et al. [72] found an mOR of 0.96 (95% CI 0.76–1.22) for participants with a BMI >28 kg·m−2.
Both van Iersel et al. [73] and Zheng et al. [63] identified a Western-style diet, characterised by a high intake of refined grains, red and processed meat, saturated fats, sweets, and desserts, as a risk factor for COPD, with the latter providing an mOR of 2.12 (95% CI 1.64–2.74) [63]. Parvizian et al. [51] studied unhealthy dietary patterns, i.e. Western diets and diets high in carbohydrates, but the results were not statistically significant (mOR 1.22, 95% CI 0.84–1.76). Additionally, they found a healthy dietary pattern, i.e. high in fruit and vegetables, to reduce COPD risk (mOR 0.88, 95% CI 0.82–0.94)) [51]. Bellou et al. [79] found vitamin D deficiency to be a risk factor for COPD (mOR 1.77, 95% CI 1.18–2.64). Chen et al. [72] identified drinking history as a risk factor and found an mOR of 0.82 (95% CI 0.54–1.23). Drinking history was not further defined. Lastly, both van Iersel et al. [73] and Salari-Moghaddam et al. [78] identified high consumption of red and processed meat as a risk factor for COPD, with the latter finding an mHR of 1.08 (95% CI 1.03–1.13) for every 50 g increase per week in intake.
Occupational exposures
11 reviews identified occupational exposures associated with an increased risk of COPD [44, 56–58, 66, 67, 71, 79, 84, 88, 93]. Eight of those studies found that workers exposed to dust as compared to nonexposed had an increased risk of COPD [56–58, 66, 71, 79, 84, 93], with found mORs ranging from 0.97 (95% CI 0.68–1.39) by Bellou et al. [79] to 1.79 (95% CI 1.15–2.79), found by Yang et al. [57]. Both Guillien et al. [67] and Fontana et al. [88] found an association between COPD and agricultural work, with only the former providing an mOR of 1.77 (95% CI 1.50–2.08) [67]. Lastly, Baur et al. [44] found an association between workplace irritants, such as chloride or welding fumes, and COPD.
Physiological, personal and socioeconomic characteristics
Physiological, personal and socioeconomic risk factors for COPD were examined by 20 reviews [53–55, 57, 59, 61, 62, 65, 70, 72, 75, 76, 79, 85–87, 89–91, 93]. 12 reviews identified active smoking as the main risk factor for COPD [54, 55, 57, 61, 70, 72, 79, 85–87, 89, 90] and six identified second-hand smoking to be a risk factor [72, 79, 85, 92–94]. Regarding active smoking, found mORs ranged from 2.89 (95% CI 2.63–3.17), found by Forey et al. [90], to 5.50 (95% CI 4.20–7.20), found by Sutradhar et al. [70]. Regarding second-hand smoke exposure, found risk estimates range from an mRR of 1.20 (95% CI 1.08–1.34) found by Lee et al. [92], to an mOR of 1.56 (95% CI 1.40–1.74) [79]. Sutradhar et al. [70] found women who chewed tobacco to be at an increased risk for COPD (OR 12.90, 95% CI 3.40–49.40) [70]. Bellou et al. [79] identified waterpipe smoking as a risk factor (mOR 3.18, 95% CI 1.25–8.09).
Five studies identified having a low SES as a risk factor [57, 62, 76, 85, 93], with an mOR of 1.61 (95% CI 1.21–2.15) found by Yang et al. [57], using an education level of ≤9 years as a proxy for low SES, and ORs ranging from 0.80 (95% CI 0.50–1.30) to 3.70 (95% CI 1.90–7.00) in included studies in the review by Gershon et al. [62], using measures such as education, occupation and income as proxies for SES.
Additionally, four reviews identified older age as a risk factor [54, 70, 75, 85]. The first, by Sutradhar et al. [70], found that compared to 40–49-year-old participants, participants aged 50–59 and 60–69 years have an OR of 2.20 (95% CI 1.60–3.00) and 4.70 (95% CI 3.50–6.40), respectively. The second, by Gan et al. [75] found that with age, female smokers have a greater incline in lung function. The third, by Adeloye et al. [85] found that under the age of 50 years, COPD risk increased with an mOR of 1.50 (1.30–1.50) per 10-year increase, as well as an increased risk in participants aged 50–59 (mOR 2.10, 95% CI 1.80–2.60) and older than 60 (mOR 4.2, 95% CI 3.10–5.60).
Two reviews identified biomarkers as risk factors [53, 91]. Chaudhary et al. [91] found an association between elevated serum homocysteine and COPD risk (mean difference 3.05) as compared to healthy controls, with elevated serum homocysteine being associated with cigarette smoking. Su et al. [53] found several inflammatory markers to be associated with COPD risk. Elevated C-reactive protein compared to regular levels had an SMD of 1.21 (95% CI 0.92–1.50), leukocytes SMD 1.07 (95% CI 0.25–1.88), interleukin (IL)-6 SMD 0.90 (95% CI 0.48–1.31), IL-8 SMD 2.34 (95% CI 0.69–4.00) and fibrinogen SMD 0.87 (95% CI 0.44–1.31). They did not find a significant relationship between COPD and tumour necrosis factor-α levels.
Xiong et al. [59] identified living at high altitudes (>1500 m) as a possible risk factor for COPD, but it was noted it was not an independent risk factor (mOR 1.18, 95% CI 0.85–1.62). Bellou et al. [79] identified traffic intensity as a possible risk factor and found an mOR of 1.30 (95% CI 0.92–1.82) per 5000 vehicles per day increase on the nearest road and an mOR of 1.26 (95% CI 0.95–1.70) for traffic load on major roads within 100 m per 500 000 vehicles per day increase. However, results were not significant. Adeloye et al. [85] identified living in both rural (mOR 1.40, 95% CI 1.30–1.60) and urban (mOR 1.20, 95% CI 1.00–1.50) areas as a risk factor; however, only the results for living in rural areas were significant.
Yang et al. [57] reported males to be at an increased risk for COPD (mOR 1.47, 95% CI 1.10–1.96), which is in accordance with results from Adeloye et al. [85] (mOR 2.10, 95% CI 1.90–2.30) and Chen et al. [72] (mOR 1.70, 95% CI 1.31–2.22)). They also reported poor housing ventilation, e.g. poor kitchen ventilation (mOR 3.99, 95% CI 1.24–12.82), to increase COPD risk [57]. Yang et al. [57] also found recurrent respiratory infections to increase the risk of COPD (mOR 15.02, 95% CI 4.54–49.68). Bellou et al. [79] identified a history of rheumatoid arthritis (mOR 1.99, 95% CI 1.61–2.45) or psoriasis (mOR 1.45, 95% CI 1.21–1.73) as risk factors for COPD. Four studies identified previous tuberculosis as a risk factor for COPD [61, 85, 93, 94], with mORs of 2.80 (95% CI 1.90–4.00) [85] and 5.98 (95% CI 4.18–8.56) [61].
Lastly, four reviews identified an increased risk of COPD when one of the parents has the condition as well [57, 65, 72, 85], with found mORs ranging from 1.57 (95% CI 1.29–1.93) [65] to 2.07 (95% CI 1.47–2.92) [57], respectively.
Discussion
To the best of our knowledge, this is the first umbrella review that provides an overview and comparison of nongenetic risk factors for COPD and asthma. We identified 43 risk factors for AOA and 45 for COPD. Risk factors were grouped into different categories.
AOA
Two reviews reported wood dust workers to be at an increased risk for asthma [25, 34], which was also one of the workplace irritants included by Baur et al. [44]. This indicates the importance of occupational factors in asthma development, which is supported by the asthma-specific job exposure matrix developed by Kennedy et al. [95]. Additionally, the lowest JBI score was six out of 10, indicating no major issues. Second, a strong association was found between a higher BMI and increased asthma risk [31, 40, 42]. The association was found for both overweight and obese participants, compared to participants with a healthy BMI. Female sex was also associated with late-onset asthma [36] in a review specifically examining AOA. They stated the underlying mechanism was unclear, but that it could be related to lifetime changes in female sex hormones and gender-specific differences in allergic sensitivities [36]. However, male sex was also identified as a risk factor in one review [31]. Lastly, several chemical exposures were associated with asthma, such as formaldehyde [21], VOCs [27], pesticides [46] and phthalates [47]. Three reviews [31, 36, 42] focused on smoking as a risk factor, of which two specified age of onset [36, 42]. Two showed an association with AOA [31, 36]. The third, not showing an association with an increased risk, only included two papers on smoking in total with contradicting results. One found a protective effect and one showed an increased risk [42]. We did not differentiate between allergic and nonallergic asthma as this was not clearly stated in each review, but since we are focusing on adult asthma, most are likely nonallergic cases.
COPD
12 reviews [54, 55, 57, 61, 70, 72, 79, 85–87, 89, 90] stated active smoking, as compared to nonsmokers, to be the main risk factor for COPD. 15 reviews [54, 57, 61, 69, 70, 72, 76, 77, 79, 81, 83, 85, 86, 93, 94] identified indoor biomass burning as a risk factor for COPD. Even though most of those studies were performed in lower income countries, it highlights the importance of particulate matter exposure, and the need for proper ventilation and the use of less damaging fuels indoors (e.g. natural gas, electric instead of solid fuels). Four reviews [57, 60, 72, 82] found ambient PM2.5 and NO2 concentrations to increase COPD risk. According to the World Health Organization (WHO), 99% of the global population lives in places where air pollution levels exceed the WHO requirements [96]. This highlights the need for concrete policies to reduce emissions. Several studies identified early life exposures [50, 52, 57, 68, 70, 72, 80, 85, 92, 93, 94], such as childhood asthma and respiratory problems, as risk factors for COPD. This shows the importance of prioritising children's respiratory health, as the consequences might linger into adulthood.
Three reviews reported a western, unhealthy diet to increase COPD risk [51, 63, 73] and five studies identified low BMI as a risk factor [57, 74, 76]. A proposed biological pathway has been oxidative stress, which is associated with COPD development, and certain foods could have a protective role [97]. This shows how efforts of prevention could take advantage of this protective effect by including lifestyle measures, beyond smoking cessation, and include nutritional counselling. Eight reviews [56–58, 66, 71, 79, 84, 93] identified occupational dust as a risk factor, indicating efforts should be made to reduce dust exposure in the workplace and/or provide workers with protective equipment to mitigate the risk. Lastly, four reviews identified parental COPD as a risk factor independent of having specific genetic variations [57, 65, 72, 85], possibly making it easier to identify people at risk early on.
Differences and similarities
A second aim of this review was to identify both differences and similarities between risk factors for COPD and asthma. One of the main differences is BMI, with a high BMI being a risk factor for asthma, as opposed to a low BMI being a risk factor for COPD, and a high BMI being a protective factor. Second, both male and female sex were found to be risk factors for AOA, while males had a higher risk of COPD. However, Yang et al. [57] mention that currently COPD prevalence in males and females is close to equal, due to changes in smoking behaviour. Furthermore, even though most found risk factors differed, they were not contradicting.
We also found several similarities. First, for both diseases a low birth weight and pre-term delivery were implied as risk factors, even though pre-term delivery was not statistically significant for either. Second, occupational dust exposure was found in multiple reviews for both conditions, indicating an area for prevention. Third, active and passive smoking are important risk factors for both COPD and AOA. Even though the number of included reviews specifically focusing on smoking is limited, most studies adjusted for smoking. Fourth, ambient air pollution, in the form of NO2 and particulate matter, was found to be a risk factor for both COPD and AOA. Finally, both pesticide exposure and exposure to workplace irritants such as chloride, were identified as risk factors for both AOA and COPD.
Strengths and limitations
There were several strengths. First, we conducted a comprehensive search on two highly prevalent diseases and provided an overview of nongenetic risk factors. This could help further develop prevention strategies and aid in the correct classification of both. Second, multiple authors did a partial screening and extraction of data, to limit errors in inclusion and data extraction. Last, because of the design, we were able to include most nongenetic risk factors for both asthma and COPD, which could have been unfeasible otherwise.
The review also has several limitations, which need to be considered. First, only seven out of the 30 studies that examined risk factors for asthma specified AOA, as opposed to asthma in adults. Four more only imply adult onset, as they investigate asthma development since starting work in certain occupational groups, but it is not explicitly specified that this is the case. As we were specifically interested in AOA and not asthma developed early in life, this might have impacted our results. This could be because risk factors for childhood asthma, lingering on into adulthood, are not the same as risk factors for developing asthma at a later age. Additionally, only a few studies confirmed asthma diagnosis by means of specific symptoms in combination with airway reversibility, the other studies did not specify the diagnosis which may result in the inclusion of patients with airway symptoms due to other diseases. Second, asthma studies including only adults were scarce. For most studies, the main focus was on asthma in children, leading to small sample sizes when excluding the population younger than 18 years of age. This lack of studies makes it difficult to draw firm conclusions. Third, for both asthma and COPD, not every review included a meta-analysis and/or provided a quantitative outcome measure or pooled estimates. This made comparing the results more difficult and could have led to some findings being over- or under-represented. However, as we did a risk of bias assessment, with JBI scores ranging between five and 11, this risk might be limited, as none indicated a high risk of bias. Fourth, we included every review regardless of quality and did not distinguish between the different JBI scores when interpreting results. Last, since we focused on incidence, we might have missed risk factors that become more apparent when taking mortality and exacerbations into account, such as ozone.
Implications
As our review provides an overview of risk factors of asthma and COPD, this provides possible targets for early identification and prevention. Since the costs of chronic diseases, both for healthcare and for individual health are high, this might result in significant financial savings and reduce the loss of quality of life [98]. Further, the Global Burden of Disease Study currently calculates risk based on six risk factors for COPD (smoking, second-hand smoke, household air pollution, ambient particulate matter, ozone and occupational particulates) and two for asthma (smoking and occupational asthmagens, e.g. occupational wood dust and cleaning materials) [4]. As this review identified many more risk factors, the burden of disease might currently be underestimated. Additionally, our review has highlighted the differences in risk factors for COPD and AOA, meaning interventions need to be targeted to the specific population at risk.
Our review has also highlighted areas in which more research is needed. Few reviews focus on asthma in adults and even fewer focus on AOA. As research has shown AOA is less atopic and has a worse prognosis than childhood asthma [9], more research into this specific population is needed.
Conclusions
In this umbrella review, we provided an overview of nongenetic risk factors for COPD and AOA. Importantly, both diseases share several known lung-damaging and nongenetic factors such as smoking and occupational exposures. There are also some notable differences, such as BMI and air pollution. More research specifically on AOA should be performed to better understand these risk factors. Overall, the results of this review could help in differentiating between these diseases when diagnosing, as well as more targeted and earlier identification of cases, by identifying people at risk.
Supplementary material
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Supplementary material ERR-0009-2023.SUPPLEMENT
Footnotes
Provenance: Submitted article, peer reviewed.
Conflict of interest: A.H. Maitland-Van der Zee is the PI of P4O2 (Precision Medicine for more Oxygen) public–private partnership sponsored by Health Holland involving many private partners who contribute in cash and/or in kind. Partners in the Precision Medicine for more Oxygen (P4O2) consortium are the Amsterdam UMC, Leiden University Medical Center, Maastricht UMC+, Maastricht University, UMC Groningen, UMC Utrecht, Utrecht University, TNO, Aparito, Boehringer Ingelheim, Breathomix, Clear, Danone Nutricia Research, Fluidda, MonitAir, Ncardia, Ortec Logiqcare, Philips, Proefdiervrij, Quantib-U, RespiQ, Roche, Smartfish, SODAQ, Thirona, TopMD, Lung Alliance Netherlands (LAN) and the Lung Foundation Netherlands (Longfonds). The consortium is additionally funded by the PPP Allowance made available by Health Holland, Top Sector Life Sciences & Health (LSHM20104; LSHM20068), to stimulate public-private partnerships and by Novartis. A.H. Maitland-Van der Zee has received grants from Boehringer Ingelheim, Vertex Innovation Award, Dutch Lung Foundation, Stichting Asthma Bestrijding, and Innovative Medicine Initiative (IMI). A.H. Maitland-Van der Zee has received consulting fees from AstraZeneca and Boehringer Ingelheim. A.H. Maitland-Van der Zee has received GSK honarium for a lecture. A.H. Maitland-Van der Zee is the chair of DSMB SOS BPD study and advisory board member of the CHAMP study. A.H. Maitland-Van der Zee is the president of the federation of innovative drug research in the Netherlands (FIGON) and president of the European Association of systems medicine (EASYM). The remaining authors have no conflicts to declare.
Support statement: Partners in the Precision Medicine for more Oxygen (P4O2) consortium are the Amsterdam UMC, Leiden University Medical Center, Maastricht UMC+, Maastricht University, UMC Groningen, UMC Utrecht, Utrecht University, TNO, Aparito, Boehringer Ingelheim, Breathomix, Clear, Danone Nutricia Research, Fluidda, MonitAir, Ncardia, Ortec Logiqcare, Philips, Proefdiervrij, Quantib-U, RespiQ, Roche, Smartfish, SODAQ, Thirona, TopMD, Lung Alliance Netherlands (LAN) and the Lung Foundation Netherlands (Longfonds). The consortium is additionally funded by the PPP Allowance made available by Health Holland, Top Sector Life Sciences & Health (LSHM20104; LSHM20068), to stimulate public-private partnerships and by Novartis. Funding information for this article has been deposited with the Crossref Funder Registry.
- Received January 9, 2023.
- Accepted February 27, 2023.
- Copyright ©The authors 2023
This version is distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0. For commercial reproduction rights and permissions contact permissions{at}ersnet.org
References










