





Figures
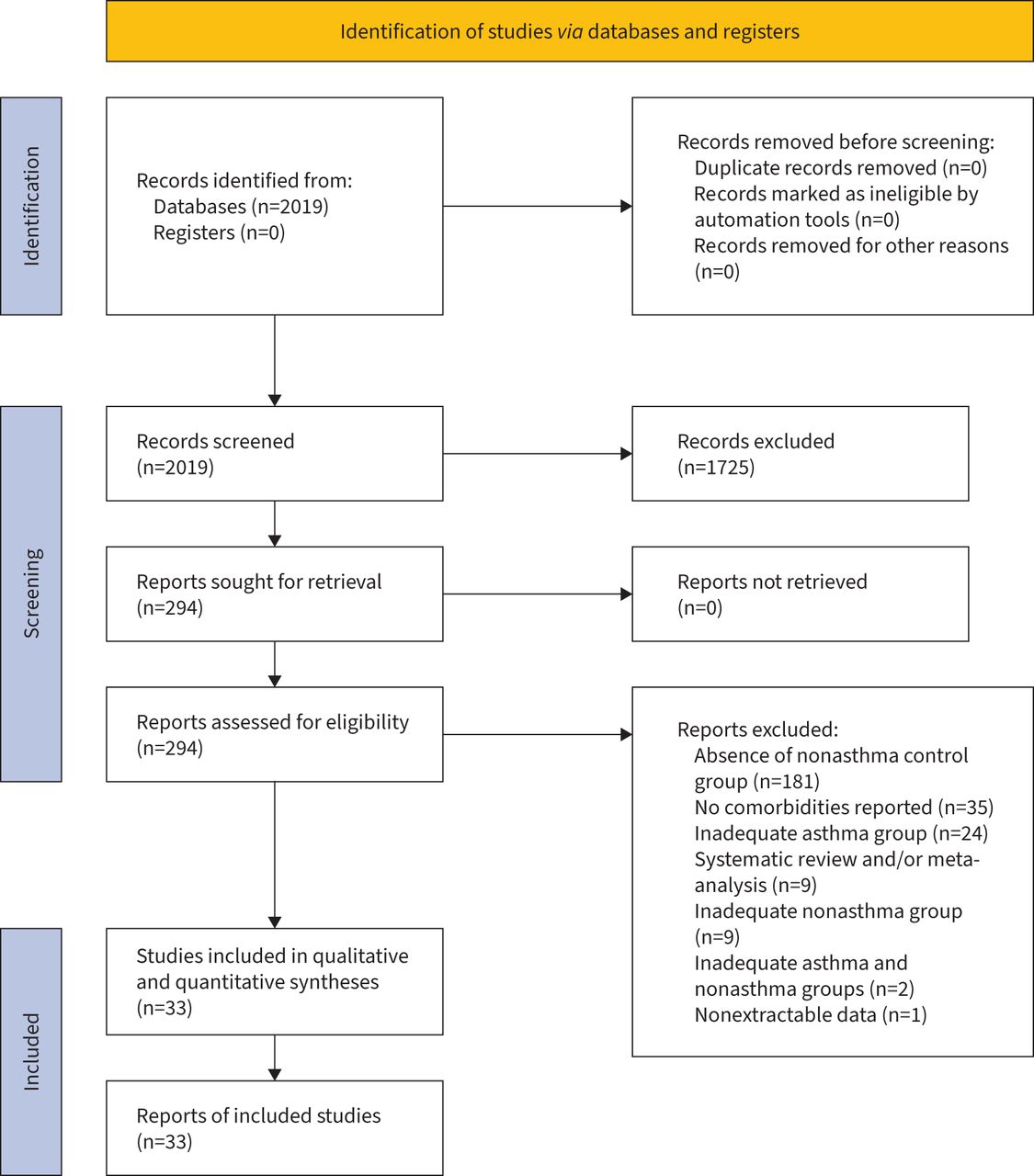
- FIGURE 1
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) 2020 flow diagram for the identification of the studies included in the pairwise meta-analysis.
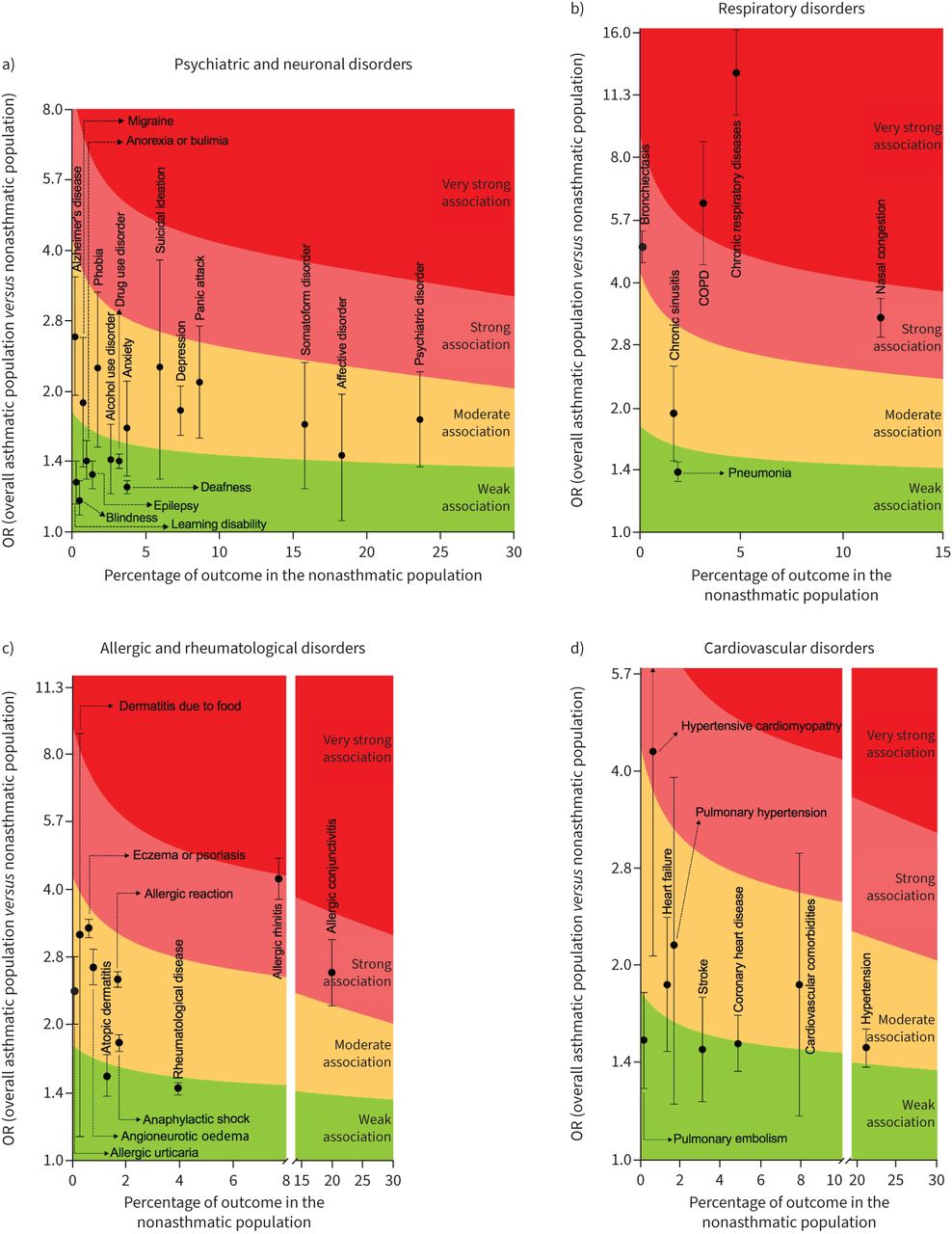
- FIGURE 2
Analysis of the strength of association of specific a) psychiatric and neuronal disorders, b) respiratory disorders, c) allergic disorders and d) cardiovascular disorders with asthma.
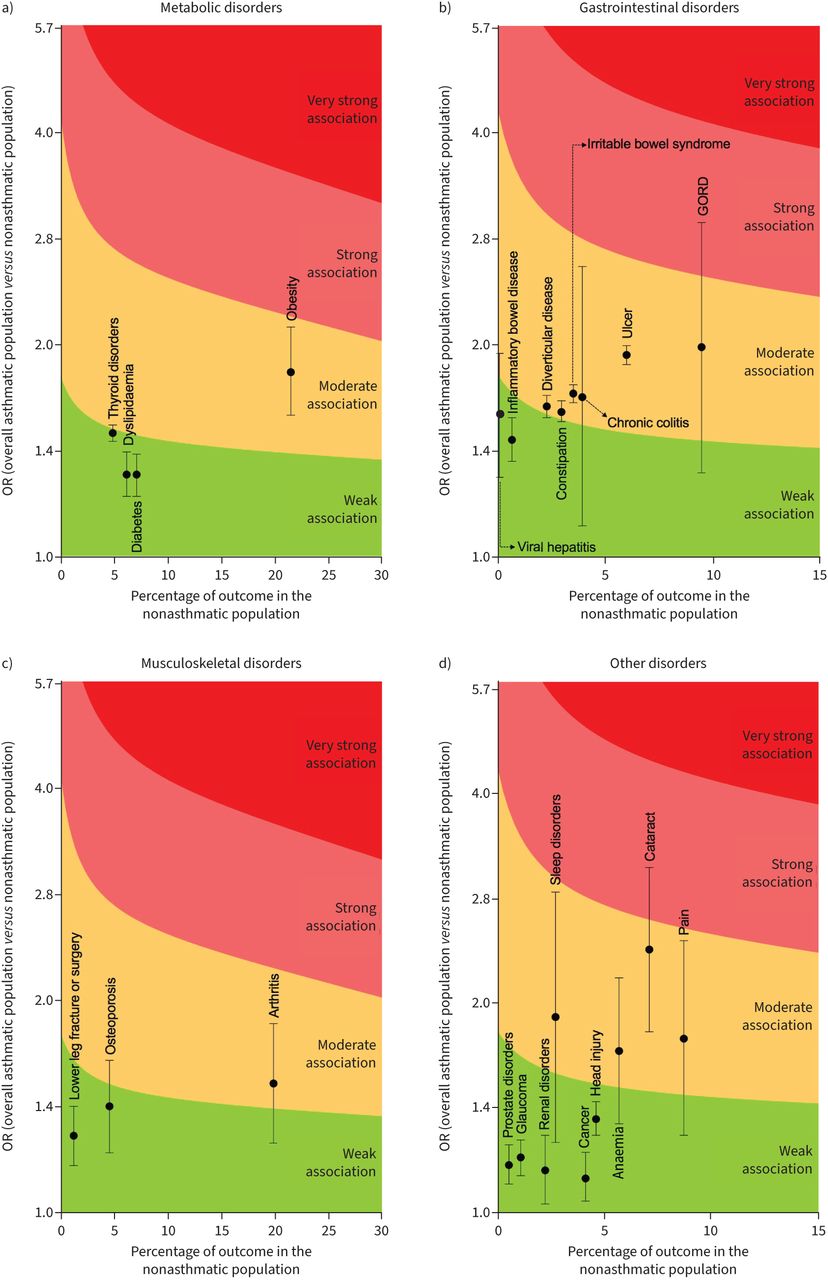
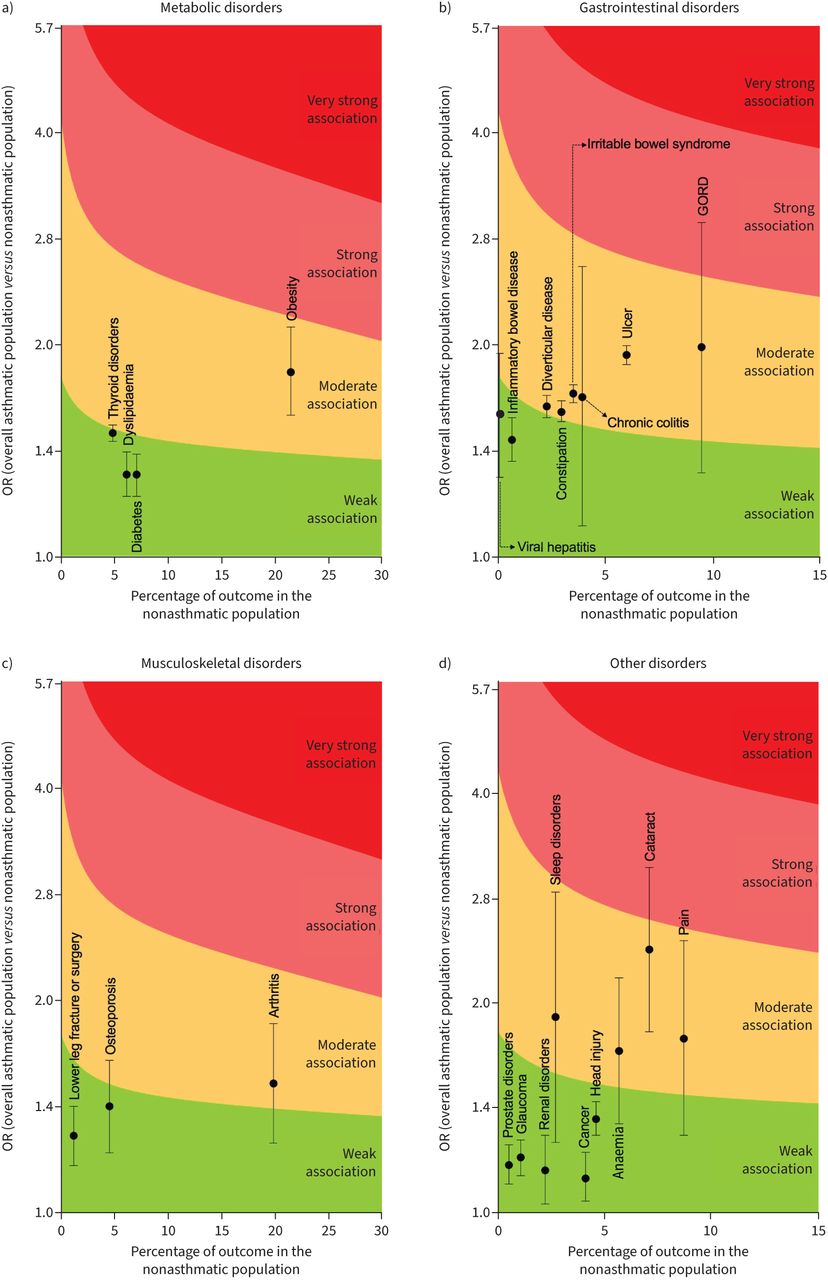
- FIGURE 3
Analysis of the strength of association of specific a) metabolic disorders, b) gastrointestinal disorders, c) musculoskeletal disorders and d) other disorders with asthma. GORD: gastro-oesophageal reflux disease.
- FIGURE 4
Analysis of the strength of association of specific a) psychiatric and neurological disorders, b) respiratory and allergic disorders, c) cardiovascular disorders, d) metabolic disorders and e) other disorders with severe asthma.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Tables
- TABLE 1
Main characteristics of the observational studies included in the pairwise meta-analysis. When necessary, age, sex and smoking habit were reported as weighted arithmetic mean between asthma and nonasthma populations
First author, year [ref.] Country Study characteristics Duration of observation (years) Subjects analysed Asthmatic subjects Groups of comparison Subjects’ characteristics Age (years) Male (%) Diagnosis of asthma Current smokers (%) NOS quality assessment JBI checklist tool+ Selection Comparability Outcome#/exposure¶ Total Chalitsios, 2021 [49] UK Population-based, retrospective, longitudinal, cohort study 13 658 749 138 123 (21.0) Asthma versus nonasthma control Subjects selected from the UK Clinical Practice Research Database 51.8 41.0 Read codes for asthma 20.4 **** ** ** 8 Landré, 2020 [50] France Retrospective, cohort study 26 12 345 372 (3.0) Asthma versus nonasthma control Subjects selected from the French GAZEL cohort of community-dwelling adults 69.8 74.0 Diagnosis defined by questionnaire 7.0 *** § ƒ 3 Carter, 2019 [54] UK Retrospective, cohort study ≈12 362 544 60 424 (16.7) Asthma versus nonasthma control Subjects admitted to NHS hospitals in the UK 48.6 26.5 Diagnostic ICD-10 and OPCS-4 disease codes NA *** § ** * ƒ 6 Kim, 2019 [55] Korea Population-based, retrospective, longitudinal, cohort study ≈11 226 118 113 059 (50.0) Asthma versus nonasthma control Subjects randomly selected from the Korean National Health Insurance Service Database ≥20.0 37.3 Asthma or status asthmaticus diagnostic ICD-10 codes: J45 or J46 of a physician diagnosis NA *** § ** * ƒ 6 Kim, 2019 [40] US Population-based, retrospective, cross-sectional survey ≈4 643 885 44 420 (6.9) Asthma versus nonasthma control Representative sample of civilian, non-institutionalised subjects of USA selected from the National Health Interview Survey ≥18.0 48.0 Diagnosis defined by questionnaire 16.0 High bias Bourdin, 2019 [63] France Population-based, retrospective, case–control study 3 2760 690 (25.0) Severe asthma versus nonasthma control Subjects randomly selected from a French representative claims database 61.0 34.3 Diagnosis based on GINA recommendations (severe asthma patients received ≥1 dispensing for OMA and/or ≥10 dispensings of a medium or high dose of ICS+LABA) NA *** ** ** 7 Toppila-Salmi, 2019 [64] Finland Population-based, retrospective, case–control study 1 2890 1118 (38.7) Asthma (includes severe asthma) versus nonasthma control Subjects randomly selected from the Finnish Drug Reimbursement Register 53.0 37.0 Drug reimbursement decision of diagnosed asthma granted by prior physician's certificate, which includes background information, clinical examination results, lung function test results and findings and conclusions after asthma treatment test for 6 months NA *** ** * 6 Varsano, 2017 [39] Israel Population-based, retrospective, cross-sectional study 1 39 991 19 991 (50.0) Nonsevere and severe asthma versus nonasthma control Subjects selected from an Israeli population present in a national electronic healthcare insurance provider database 42.2 23.8 Asthma diagnostic ICD-9 CM code of a physician's diagnosis of bronchial asthma 20.0 Low bias Weatherburn, 2017 [38] UK Population-based, retrospective, cross-sectional study NA 1 424 378 84 505 (5.9) Asthma versus nonasthma control Representative sample of the Scottish population selected from the UK NHS database of primary care practice ≥18.0 49.1 Primary-care physician's diagnosis 24.5 Moderate bias Bozek, 2016 [37] Poland Population-based, retrospective, cross-sectional study 1 2099 1023 (48.7) Asthma versus nonasthma control Representative population of all regions of Poland randomly selected from patient databases 67.9 46.4 Diagnosis based on clinical criteria according to GINA recommendations and a positive reversibility test after salbutamol according to the ATS/ERS criteria 6.9 Moderate bias Peng, 2015 [56] Taiwan Nationwide, retrospective, population-based, cohort study ≈3 63 855 12 771 (20.0) Asthma versus nonasthma control Subjects randomly selected from the National Health Insurance Research Database of Taiwan 53.7 45.8 Asthma diagnostic ICD-9 CM code: 493 NA *** § ** * ƒ 6 Van den Bemt, 2016 [57] The Netherlands Dynamic historical, longitudinal, cohort study ≈20 2385 795 (33.3) Asthma versus nonasthma control Subjects selected from the Continuous Morbidity Registration Nijmegen database 33.3 41.1 Physician's diagnosis NA **** ** ** 8 Yao, 2016 [58] China Population-based, retrospective, longitudinal, cohort study 6 84 474 28 158 (33.3) Asthma versus nonasthma control Subjects randomly selected from the National Health Insurance Research Database of Taiwan 54.5 46.3 Asthma diagnostic ICD-9 CM code: 493; subjects who had ≥1 hospitalisation or ≥3 visits for outpatient medical services for asthma NA *** § ** * ƒ 6 Cheng, 2015 [59] Taiwan Nationwide, retrospective, longitudinal, cohort study 11 52 275 10 455 (20.0) Asthma versus nonasthma control Subjects randomly selected from the National Health Insurance Research Database of Taiwan 59.8 41.3 Asthma diagnostic ICD-9 CM code: 493; diagnosis by pulmonologist or rheumatologist on clinical judgement or pulmonary function test NA *** § ** * ƒ 6 Alcázar Navarrete, 2015 [36] Spain Cross-sectional study NA 57 40 (70.2) Asthma versus nonasthma control Outpatients in an ambulatory setting 60.8 31.6 Previous physician diagnosis of bronchial asthma 7.0 Moderate bias Chung, 2014 [60] Taiwan Nationwide, retrospective, population-based, cohort study 6 156 513 31 356 (20.0) Asthma versus nonasthma control Subjects randomly selected from the National Health Insurance Research Database of Taiwan 38.9 49.0 Asthma diagnostic ICD-9 code: 493 from ambulatory case visits or admission records NA *** § ** * ƒ 6 Chung, 2014 [61] Taiwan Nationwide, retrospective, population-based, cohort study 11 72 587 14 518 (20.0) Asthma versus nonasthma control Subjects randomly selected from the National Health Insurance Research Database of Taiwan 52.1 45.7 Asthma diagnostic ICD-9 CM code: 493 NA *** § ** * ƒ 6 Steppuhn, 2014 [48] Germany Population-based, retrospective, cross-sectional survey 2 43 189 2242 (5.2) Asthma versus nonasthma control Adults randomly selected for the national telephone health interview survey in Germany 49.0 48.6 Self-reported physician's diagnosis 29.8 Low bias Huang, 2014 [65] Taiwan Nationwide, prospective, population–based, case–control study (comorbidities were assessed retrospectively) 3 140 344 35 086 (25.0) Asthma versus nonasthma control Subjects randomly selected from the National Health Insurance Research Database of Taiwan 47.7 44.1 Diagnosis by board-certified internist, clinical immunologist, pulmonologist or other medical experts NA **** ** ** 8 Chen, 2014 [62] Taiwan Nationwide, retrospective, longitudinal, population-based, cohort study 11 55 150 11 030 (20.0) Asthma versus nonasthma control Subjects randomly selected from the National Health Insurance Research Database of Taiwan 60.9 41.7 Asthma diagnostic ICD-9 CM code: 493 NA *** § ** * ƒ 6 Sundbom, 2013 [47] Sweden Population-based, retrospective, cross-sectional survey 1 25 610 1830 (7.1) Asthma versus nonasthma control Subjects randomly selected for the 2008 GA2LEN survey 43.7 49.0 Diagnosis defined by questionnaire 13.8 Moderate bias Marcon, 2013 [66] Italy Population-based, retrospective, multi-case–control study ≈3 662 360 (54.4) Mild asthma versus nonasthma control Subjects randomly selected from the general population belonging to the Italian Study on Asthma in Young Adults cohort and to the Italian branch of the European Community Respiratory Health Survey cohort 43.8 49.0 Diagnosis defined by questionnaire and lung function tests 22.4 **** * 5 Lu, 2013 [46] Singapore Population-based, retrospective, cross-sectional survey 1 2809 106 (3.8) Asthma versus nonasthma control Adults randomly selected from the Singapore National Mental Health Survey 20.0–59.0 38.2 Self-report of a doctor's diagnosis NA Low bias Traister, 2013 [51] USA Retrospective, cohort study ≈6 160 59 (36.9) Asthma versus nonasthma control Outpatients selected by random computer-generated sequence 44.6 33.7 Asthma diagnostic ICD-9 CM code: 493 and spirometry tests 35.1 *** § ƒ 3 Patel, 2013 [45] USA Population-based, retrospective, cross-sectional survey 8 22 172 2873 (13.0) Asthma versus nonasthma control Representative sample of civilian, non-institutionalised subjects of USA selected from the National Health and Nutrition Examination Survey 46.7 48.1 Self-report of a physician's diagnosis NA Moderate bias Iribarren, 2012 [52] USA Prospective, cohort study (comorbidities were assessed retrospectively) 13 407 190 203 595 (50.0) Asthma versus nonasthma control Adults selected from the Kaiser Permanente Northern California healthcare plan 44.6 34.0 Medical records of hospitalisation with primary discharge code ICD-9 CM 493.00−493.99 or ≥1 secondary code for asthma with a principal ICD-9 code for acute asthma-related respiratory conditions, or outpatient or ED visits for asthma 17.4 *** § ** * ƒ 6 Luyster, 2012 [44] USA and UK Retrospective, cross-sectional study NA 282 222 (78.7) Nonsevere asthma and severe asthma versus nonasthma control Participants selected from the retrospective multicentre Severe Asthma Research Program cohort study 31.5 47.4 Evaluation and classification according to the ATS definition of refractory asthma; diagnosis of severe asthma required continuous oral corticosteroid use or high-dose ICS use and ≥2 of the 7 minor criteria [67] 0.0 Moderate bias Cazzola, 2011 [6] Italy Population-based retrospective, cross-sectional study 1 909 638 55 500 (6.1) Asthma versus nonasthma control Subjects selected from the Health Search Database of the Italian College of General Practitioners >14.0 47.3 Asthma diagnostic ICD-9 CM code: 493 NA Low bias Hakola, 2011 [53] Finland Prospective, cohort study (comorbidities were assessed retrospectively) 1–4 64 951 2196 (3.4) Persistent asthma versus nonasthma control Finnish public sector employees selected from national registers 44.1 20.0 Physician's diagnosis confirmation by the Social Insurance Institution of Finland 18.3 *** § * ƒ 5 Ng, 2007 [43] Singapore Population-based, retrospective, cross-sectional survey 1 1092 61 (5.6) Asthma versus nonasthma control Older adults selected from the National Mental Health Survey of Elderly of Singapore ≥60.0 NA Self-report of a doctor's diagnosis NA Low bias Adams, 2006 [42] Australia Population-based, retrospective, cross-sectional household telephone interview survey 1 7443 834 (11.2) Asthma versus nonasthma control Adults selected from the Collaborative Health and Well-being Survey ≥18.0 50.9 Self-report of a doctor's diagnosis NA High bias Goodwin, 2003 [41] USA Retrospective, cross-sectional study ≈2 998 176 (17.6) Asthma versus nonasthma control Primary care patients 18.0–70.0 25.1 Asthma diagnostic ICD-9 CM code: 493 of a primary-care physician's diagnosis NA Moderate bias Goodwin, 2003 [35] Germany Population-based, retrospective, cross-sectional, core survey 1 4181 236 (5.6) Nonsevere and severe asthma versus nonasthma control Representative community sample of adults 41.1 41.0 Questionnaire and physician's diagnosis NA Moderate bias Data are presented as n or n (%), unless otherwise stated. NOS: Newcastle–Ottawa Scale; JBI: Joanna Briggs Institute; NHS: National Health Service; ICD: International Statistical Classification of Diseases and Related Health Problems; OPCS: Office of Population Censuses and Surveys Classification of Interventions and Procedures; NA: not available; GINA: Global Initiative for Asthma; OMA: omalizumab; ICS: inhaled corticosteroids; LABA: long-acting β2-adrenoceptor agonists; CM: Clinical Modification; ATS: American Thoracic Society; ERS: European Respiratory Society; ED: emergency department. #: cohort studies could not be assigned a star for the outcome item “adequacy of follow-up of cohorts”, as outcomes of interest were all assessed retrospectively and there was no mention of losses; ¶: case–control studies could not be assigned a star for the exposure item “non-response rate”, as outcomes of interest were all assessed retrospectively; +: each of the eight items of the JBI tool was rated as “yes” (1 point) and “no” or “not applicable” (0 points). The score for each cross-sectional study was calculated on the proportion of “yes” responses for the possible maximum score and rated as high, moderate or low risk of bias according to the achieved score expressed as percentage (high bias: ≤49.0%; moderate bias: 50.0–69.0%; low bias ≥70.0%); §: no star could be assigned for the selection item “demonstration that outcome of interest was not present at start of study”, as outcomes of interest were already present at baseline; ƒ: no star could be assigned for the outcome item “was follow-up long enough for outcomes to occur”, as outcomes of interest were already present at baseline.
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Supplementary material ERR-0202-2022.SUPPLEMENT










