





Abstract
The association between current smoking and coronavirus disease 2019 (COVID-19) progression remains uncertain. We aim to provide up-to-date evidence of the role of cigarette smoking in COVID-19 hospitalisation, severity and mortality. On 23 February 2022 we conducted an umbrella review and a traditional systematic review via PubMed/Medline and Web of Science. We used random-effects meta-analyses to derive pooled odds ratios of COVID-19 outcomes for smokers in cohorts of severe acute respiratory syndrome coronavirus 2 infected individuals or COVID-19 patients. We followed the Meta-analysis of Observational Studies in Epidemiology reporting guidelines. PROSPERO: CRD42020207003. 320 publications were included. The pooled odds ratio for current versus never or nonsmokers was 1.08 (95% CI 0.98–1.19; 37 studies) for hospitalisation, 1.34 (95% CI 1.22–1.48; 124 studies) for severity and 1.32 (95% CI 1.20–1.45; 119 studies) for mortality. Estimates for former versus never-smokers were 1.16 (95% CI 1.03–1.31; 22 studies), 1.41 (95% CI: 1.25–1.59; 44 studies) and 1.46 (95% CI 1.31–1.62; 44 studies), respectively. Estimates for ever- versus never-smokers were 1.16 (95% CI 1.05–1.27; 33 studies), 1.44 (95% CI 1.31–1.58; 110 studies) and 1.39 (95% CI 1.29–1.50; 109 studies), respectively. We found a 30–50% excess risk of COVID-19 progression for current and former smokers compared with never-smokers. Preventing serious COVID-19 outcomes, including death, seems the newest compelling argument against smoking.
Abstract
We found an excess risk of progression of COVID-19 of 30–50% for current and ex-smokers compared to never-smokers. Our results suggest that a non-negligible proportion of the 6.2 million deaths worldwide due to COVID-19 are attributable to tobacco smoking. https://bit.ly/3TXLUy8
Introduction
Coronavirus disease 2019 (COVID-19) is an infectious disease caused by severe acute respiratory syndrome coronavirus (SARS-CoV-2), a coronavirus identified in China in December 2019, with similarities to the severe acute respiratory syndrome coronavirus (SARS-CoV) and to the Middle East respiratory syndrome coronavirus (MERS-CoV) [1]. COVID-19 causes no, mild or severe symptoms, but, in some individuals, it can trigger a life-threatening pneumonia [1, 2]. The World Health Organization declared the outbreak of the disease a pandemic on 11 March 2020. Globally, in June 2022, the number of COVID-19 confirmed cases exceeded 537 million and the number of COVID-19 deaths exceeded 6.3 million [3].
Since the beginning of the outbreak, a direct link between tobacco smoking and COVID-19 has been theorised. Several reasons justified this hypothesis and included that 1) tobacco smoking was found to be associated with respiratory infectious diseases, including those caused by similar viruses such as SARS-CoV or MERS-CoV [4, 5], 2) COVID-19 primarily affects the lung, an important target site of tobacco smoking, and 3) early studies from China, as well as subsequent studies, systematically showed that severe forms of COVID-19 or deaths due to the disease were more frequent in people with tobacco-related diseases, including COPD, lung cancer and cardiovascular diseases [1, 2, 6, 7].
Evidence for the relationship between tobacco smoking and incidence of COVID-19 remains uncertain and impaired by a number of case series – i.e. study designs inadequate to derive any causal conclusion – inferring a relatively low smoking prevalence among COVID-19 patients [8]. However, several systematic reviews and meta-analyses suggest a direct association between cigarette smoking and risk of progression of COVID-19 [9–12]. This notwithstanding, the most updated and comprehensive meta-analysis (based on a living systematic review) showed a significant excess risk of COVID-19 severity and mortality only for former compared with never-smokers, whereas for current smokers inconclusive findings were reported [8, 13]. That meta-analysis considered only selected studies meeting strict but arbitrary quality criteria and did not use adjusted odds ratio estimates extracted from each original article but a Bayesian approach to derive the pooled relative risk estimates [8]. It is important to confirm those results by including the same papers but using different study selection criteria and standard and robust meta-analytical approaches.
The present systematic review has been conducted to provide an updated answer to the following research question: are current and former cigarette smokers who test positive for SARS-CoV-2 at higher risk of COVID-19 hospitalisation, severity (including need for intensive care unit (ICU)) and mortality relative to never-smokers or nonsmokers (i.e. never-smokers and former smokers combined)?
Methods
We conducted a comprehensive systematic review of the literature in PubMed/Medline and Web of Science (WoS). The study followed the Meta-analysis of Observational Studies in Epidemiology reporting guideline. This is an update – focused on the role of cigarette smoking on COVID-19 hospitalisation, severity and mortality – of a broader systematic review with the protocol published in PROSPERO (2020 CRD42020207003). We used the same original and innovative search strategy approach used in other systematic reviews described by the authors of this review [14]. Thus, besides a traditional review, we also conducted an umbrella review (i.e. a review of systematic reviews and meta-analyses [14]) on PubMed/Medline and WoS to identify all the original publications considered in previous systematic reviews.
The search string used in various sources for the conduction of the systematic review is provided in supplementary table 1.
As an exposure variable we considered conventional cigarette smoking; as outcomes, we considered COVID-19 hospitalisation, severity and/or mortality. Publications written in a language other than English (34 from the traditional review and five from the umbrella review) and/or not published in peer-review journals indexed in PubMed/Medline or WoS (e.g. articles posted in pre-print archives only) were excluded both from the narrative review and from the meta-analysis. Studies based on specific subpopulations (e.g. patients with a specific disease and pregnant women) were not included and no restrictions on setting were applied. Publications eligible for the narrative review were articles providing information about the relationship between cigarette smoking (current, former and/or ever-smoking) and COVID-19 hospitalisation, severity or mortality. No restriction on study participants (e.g. age group and sex) were applied. Studies eligible for the meta-analyses were cohorts of SARS-CoV-2-infected individuals or COVID-19 patients providing relative risks, hazard ratios or odds ratios – or tabular data allowing derivation of odds ratios of COVID-19 hospitalisation, severity and mortality for current, former or ever cigarette smokers compared to never-smokers or nonsmokers (i.e. never and former smokers combined). We found duplicate findings from the same cohort study published in multiple articles. In this case, we used the most updated article with the most complete results.
Using our search strategy on 23 February 2022, the umbrella review identified 103 reviews in Pubmed/Medline and 51 reviews in WoS. After deleting duplicates and noneligible publications, 59 systematic reviews and meta-analyses were included (supplementary table 2). One of these reviews [8] was part of a living systematic review, i.e. a review that is updated rapidly as soon as new evidence becomes available [15] with additional updates in Qeios, a pre-print platform. We consequently considered the latest version updated to March 2021 [13]. All the 59 systematic reviews and meta-analyses found through the umbrella review were retrieved and examined. Each original article identified in the reference list of eligible systematic reviews and meta-analyses was collected and screened by two reviewers (M.S. and C.M.J.), resulting in 271 eligible original articles.
The selection of the traditional review was run on 23 February 2022, identifying 765 peer-reviewed publications in PubMed/Medline and 324 peer-reviewed publications in WoS. After deleting duplicates and articles already identified in the umbrella review, a total of 943 articles was obtained. An EndNote library (version: EndNote X7) was created to include all the publications identified by our search strings and by the umbrella review. Titles and abstracts of all the 943 peer-reviewed original publications identified in the traditional review were screened independently by four reviewers (M.S., I.P., M.C.M. and G.C.) to identify publications that met the inclusion criteria of the present review (first screening). The full texts of all the potentially eligible publications were retrieved and independently assessed for eligibility by the same reviewers (second screening), resulting in 96 eligible articles.
Overall, 367 peer-reviewed publications were included in the narrative review (supplementary table 3). Of them, 320 were eligible for meta-analyses, providing data on studies based on SARS-CoV-2-infected individuals or COVID-19 patients: 49 provided data on the risk of hospitalisation, 190 on the risk of COVID-19 severity and 184 on the risk of COVID-19 mortality (figure 1).

Flowchart of the systematic review. For references, see supplementary file 2.
A standardised form in Microsoft Excel was used to extract data. For each publication, the following relevant information was extracted: first author, year of publication, journal, source of identification, study design, country and study name.
For the original articles eligible for the meta-analyses considered within the present systematic review, we further extracted the type of population, the number of individuals, relative risk, hazard ratio or odds ratio, the corresponding 95% confidence interval, and the model used to derive it (with the list of covariates). Overall, 54% of studies did not provide any measure of association, 31% provided odds ratios, 13% provided hazard ratios and 2% provided relative risks. For studies which did not provide any measure of association, a crude odds ratio was derived from tabular data.
Several studies reported in the same article the association between cigarette smoking and different severity outcomes. When more than one outcome was provided, for the meta-analysis stratified by severity outcome, we prioritised them in the following order: 1) composite outcome (i.e. intubation, admission to ICU or death), 2) admission to ICU, 3) intubation, 4) mechanical ventilation, 5) severe disease (e.g. critical, severe, moderate or mild) and 6) other severity outcomes (e.g. length of stay, intensity of medical care, complicated versus noncomplicated). Five studies [16–20] reported data on the association between smoking and symptomatic versus asymptomatic SARS-CoV-2-positive individuals. These studies were included in the meta-analysis of hospitalisation because the study population was the same (i.e. SARS-CoV-2-positive individuals and not COVID-19 patients).
In an attempt to provide a single estimate for progression of disease in COVID-19 patients, we derived the meta-analysis of severity and mortality combined. Several studies reported in the same article the association between cigarette smoking and different outcomes. When more than one outcome was provided, following the relevance of the outcomes according to their seriousness, we prioritised them in the following order: 1) mortality, 2) composite outcome of severity (i.e. intubation, admission to ICU or death), 3) admission to ICU, 4) intubation, 5) mechanical ventilation, 6) severe disease (e.g. critical, severe, moderate or mild) and 7) other severity outcomes (e.g. length of stay, intensity of medical care, complicated versus noncomplicated COVID-19).
Statistical analysis
We considered the odds ratios as the main end-point. For the few studies providing hazard ratios and relative risks only, the measures were assumed as proxies of odds ratios. We used random-effects meta-analytic approaches to derive summary estimates of the odds ratios of 1) COVID-19 hospitalisation, 2) severity, 3) mortality and 4) progression of the disease (i.e. severity and mortality combined), for ever- versus never-smokers, current versus never-smokers, current versus never-smokers or nonsmokers (i.e., never and former smokers combined; for those studies providing estimates for both current versus never-smokers and current versus nonsmokers, we considered the estimate for current versus never-smokers) and for former versus never-smokers. When necessary, we computed estimates of odds ratio by pooling the odds ratios for various categories of smoking status, using the method described by Hamling et al. [21].
In order to assess heterogeneity among studies, we used the I2 statistic, which expresses the percentage of the total observed variability due to heterogeneity rather than sampling error, with higher values denoting a greater degree of heterogeneity (0–40%: little heterogeneity; 30–60%: moderate heterogeneity; 50–90%: substantial heterogeneity; 75–100%: considerable heterogeneity, according to the Cochrane Collaboration) [22].
For those studies providing the odds ratio estimates adjusted at least for age, we compared those estimates for the association between current and former cigarette smoking and COVID-19 hospitalisation, severity and mortality with the corresponding crude odds ratio estimates derived by us from tabular data.
All statistical analyses were performed using the software SAS (version 9.4) and R (version 4.0.5). Two reviewers (C.M.J. and M.C.M.) independently assessed study quality for a specific subset of the identified studies (i.e. those cohorts analysing the association with COVID-19 progression for current versus never-smokers) using the Newcastle Ottawa Assessment Scale for cohort studies adapted for this specific issue in another systematic review [12]. Any disagreement between the two reviewers was resolved by discussion.
To evaluate publication bias, we visually examined the funnel plots [23] and applied Egger's test for funnel plot asymmetry [24].
We additionally conducted a specific meta-analysis of cohort studies based on the general population providing data on the association between smoking and COVID-19 mortality, thus analysing the effect of smoking on COVID-19 incidence and mortality combined.
Results
Summary estimates of the risk of COVID-19 hospitalisation, severity, mortality and progression according to cigarette smoking are provided in table 1. Out of 49 eligible publications linking smoking history to the risk of hospitalisation among SARS-CoV-2-positive patients, 33 studies provided data on the risk of hospitalisation for ever- versus never-smokers. The pooled odds ratio was 1.16 (95% CI 1.05–1.27; figure 2). The pooled odds ratio of hospitalisation was 0.98 (95% CI 0.85–1.12; 23 studies) for current versus never-smokers, 1.08 (95% CI 0.98–1.19; 37 studies) for current versus never- or nonsmokers (supplementary figure 1) and 1.16 (95% CI 1.03–1.31; 22 studies) for former versus never-smokers (supplementary figure 2).
Odds ratios and corresponding 95% confidence interval of coronavirus disease 2019 (COVID-19) hospitalisation, severity, mortality and progression for conventional cigarette smoking

Forest plot of study-specific and pooled odds ratios for hospitalisation among severe acute respiratory syndrome coronavirus (SARS-CoV-2) positive patients for cigarette ever-smokers (ES) versus never-smokers (NS). For references, see supplementary file 2.
Out of 190 publications that investigated the relationship between cigarette smoking and COVID-19 severity, 110 studies provided data on the risk of a severe form of COVID-19 for ever- versus never-smokers. The pooled odds ratio was 1.44 (95% CI 1.31–1.58) based on more than 18 000 cases. Stratifying by severity outcome, the pooled odds ratio for ever- versus never-smokers was 1.73 (95% CI 1.30–2.30) for composite outcome, 1.32 (95% CI 1.10–1.59) for ICU admission, 1.14 (95% CI 1.01–1.27) for intubation, 1.02 (95% CI 0.85–1.22) for mechanical ventilation, 1.44 (95% CI 1.22–1.69) for a severe disease and 2.57 (95% CI 1.55–4.26) for other severity outcomes (figure 3). The pooled odds ratio of COVID-19 severity was 1.35 (95% CI 1.09–1.69; 46 studies) for current versus never-smokers, 1.34 (95% CI 1.22–1.48; 124 studies) for current versus never- or nonsmokers (supplementary figure 3) and 1.41 (95% CI 1.25–1.59; 44 studies) for former versus never-smokers (supplementary figure 4).
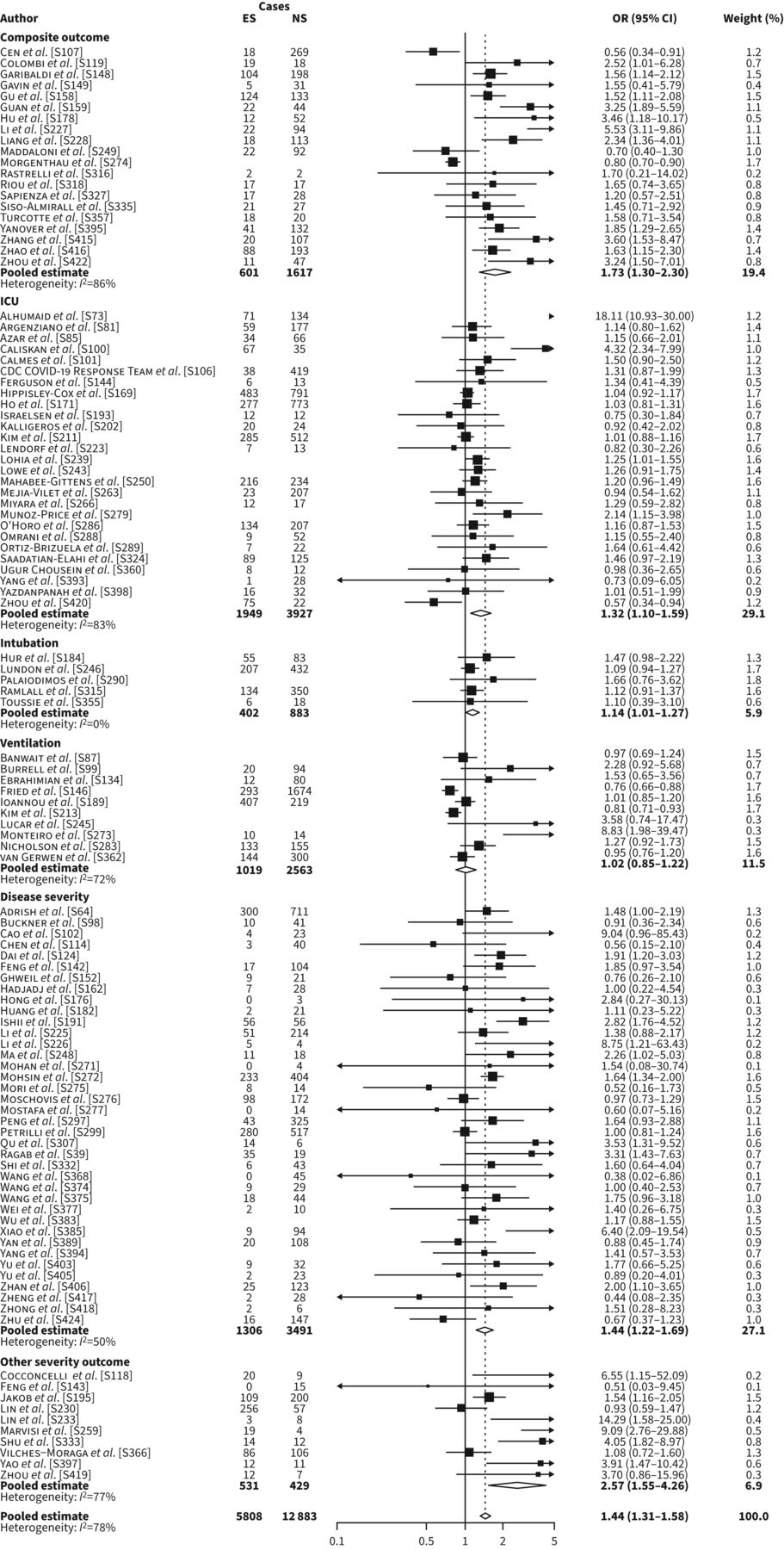
Forest plot of study-specific and pooled odds ratios of having a severe form of coronavirus disease 2019 (COVID-19) for cigarette ever-smokers (ES) versus never-smokers (NS), overall and stratified by severity outcome. For references, see supplementary file 2.
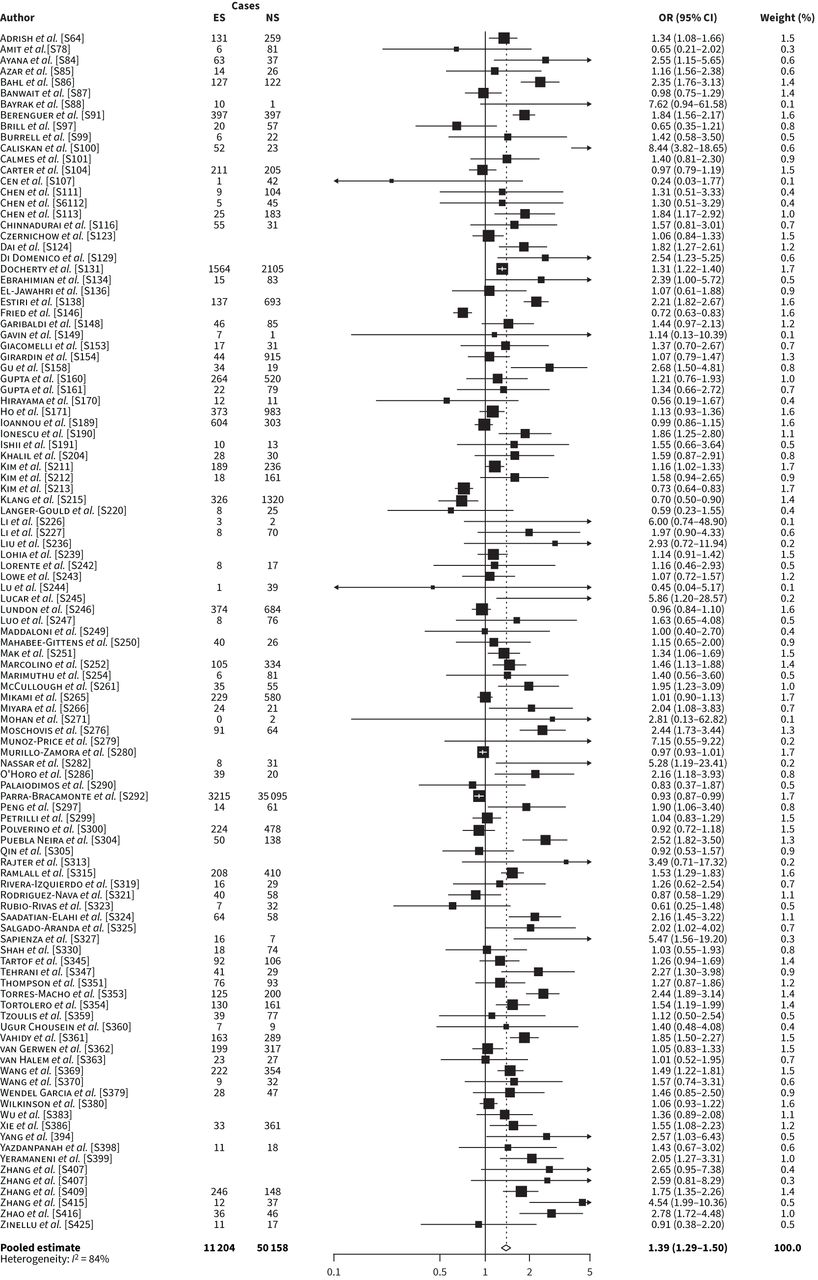
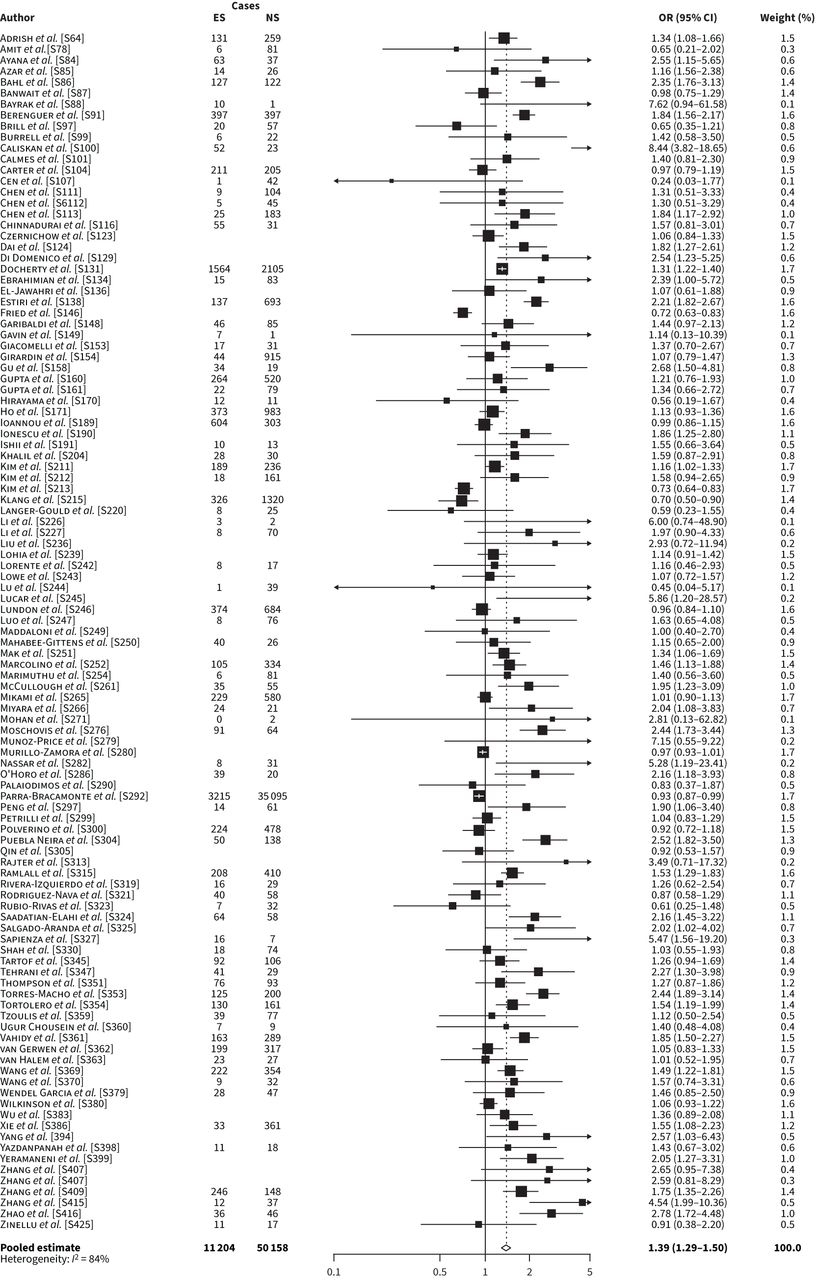
Out of 184 publications focusing on mortality among COVID-19 patients, 109 studies provided data on the odds ratio of mortality for ever- versus never-smokers. The pooled odds ratio of mortality was 1.39 (95% CI 1.29–1.50) based on more than 60 000 cases (figure 4). The pooled odds ratio of mortality for COVID-19 was 1.24 (95% CI 1.09–1.40; 46 studies) for current versus never-smokers, 1.32 (95% CI 1.20–1.45; 119 studies) for current versus never- or nonsmokers (supplementary figure 5) and 1.46 (95% CI 1.31–1.62; 44 studies) for former versus never-smokers (supplementary figure 6).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plot of study-specific and pooled odds ratios of coronavirus disease 2019 (COVID-19) mortality for cigarette ever-smokers (ES) versus never-smokers (NS). For references, see supplementary file 2.
The pooled odds ratio of COVID-19 severity and mortality combined was 1.45 (95% CI 1.35–1.54; 175 studies) for ever- versus never-smokers (supplementary figure 7). The pooled odds ratio for progression was 1.32 (95% CI 1.15–1.52; 75 studies) for current versus never-smokers (supplementary figure 8), 1.33 (95% CI 1.24–1.43; 199 studies) for current versus never- or nonsmokers (supplementary figure 9) and 1.50 (95% CI 1.37–1.65; 72 studies) for former smokers versus never-smokers (supplementary figure 10).
All the pooled estimates of the risk of COVID-19 hospitalisation, severity, mortality and progression according to cigarette smoking showed substantial to considerable heterogeneity; the I2 ranging between 55% and 90%. Overall, 18 studies provided odds ratios from multivariable analysis, adjusted at least for age, and tabular data allowing us to derive crude odds ratio estimates. Compared to never-smokers, the pooled crude odds ratio for current smokers was 1.05 (95% CI 0.90–1.24) and the pooled adjusted odds ratio was 1.22 (95% CI 0.97–1.53). The corresponding estimates for former smokers were 1.73 (95% CI 1.46–2.05) and 1.16 (95% CI 1.02–1.31) (supplementary table 4).
Following the Newcastle Ottawa Assessment Scale on those studies describing current versus never-smokers, we found 21 good-quality articles (28.0%), 0 (0.0%) fair- and 54 poor-quality articles (72.0%). The pooled odds ratios for hospitalisation, severity and mortality were 1.01 (95% CI 0.80–1.27, nine studies), 1.22 (95% CI 0.94–1.57, 11 studies) and 1.24 (95% CI 1.04–1.49, 17 studies) in good-quality studies and 0.93 (95% CI 0.85–1.12, 14 studies), 1.34 (95% CI 0.97–1.85, 35 studies) and 1.23 (95% CI 1.01–1.49, 29 studies) in poor-quality studies, respectively.
No evidence of publication bias emerged regarding hospitalisation for ever-smokers, either from visual inspection of the funnel plots or from Egger's test (p=0.90; supplementary figure 11); evidence for publication bias was found for severity and mortality for ever-smokers (p<0.01; supplementary figures 12 and 13).
Three cohorts based on the general population provided data on the association between smoking and COVID-19 mortality. The pooled age and sex-adjusted odds ratio for COVID-19 mortality was 1.73 (95% CI 0.97–3.08) for current versus never-smokers, 1.42 (95% CI 1.29–1.57) for former versus never-smokers and 1.45 (95% CI 1.25–1.70) for ever- versus never-smokers. Using the fully adjusted models, i.e. after further allowance for many comorbidities, the pooled odds ratio was 1.42 (95% CI 0.84–2.40) for current versus never-smokers 1.23 (95% CI 1.13–1.34) for former versus never-smokers and 1.25 (95% CI 1.07–1.45) for ever- versus never-smokers.
Discussion
In this comprehensive systematic review on the association between tobacco smoking and COVID-19 outcomes among SARS-CoV-2-positive individuals or COVID-19 patients we found that, compared to never-smokers, ever-smokers had a 16% higher risk of being hospitalised, a 44% higher risk of having a more severe form of the disease, a 39% higher risk of COVID-19 mortality and a 45% higher risk for progression.
These findings update and confirm results from previous meta-analyses systematically showing an excess risk of progression of diseases for current and former smokers combined compared to never-smokers [8, 10–12, 25, 26].
Current smokers had a 34% excess risk for COVID-19 severity (based on 124 studies) and 32% excess risk for mortality (based on 119 studies). For current versus never-smokers, Simons et al. [13] found an inconclusive increased relative risk of 1.26 (95% credible interval (CrI) 0.92–1.73; based on 11 studies) for severity and 1.12 (95% CrI 0.84–1.47; based on 19 studies) for mortality. Discrepancies between our results and those by Simons et al. [13] are likely due to the differences in the selection criteria of the two meta-analyses. In their analysis, Simons et al. [13] considered both peer-reviewed and pre-print publications and selected studies based upon defined quality indexes while the present systematic review considered only studies published in peer-reviewed journals. To maximise the comprehensiveness of the systematic review, it was decided not to select studies on the basis of defined quality indexes but consider aspects such as sample size and the use of adjustment to conduct stratified analyses in our meta-analysis. This decision likely results in an increased heterogeneity – all our pooled estimates showed substantial to considerable heterogeneity – that may be compensated by the increased statistical power. Another point of difference is the statistical methodologies employed, Simons et al. [8] used statistical methods based on a Bayesian approach while this study used classical meta-analytical methods.
Whereas Simons et al. [8] found a direct association with severity and mortality for former smokers, using classic analytical methods we did not observe major differences in the risk of disease progression between current and former smokers. The excess risk found by their analysis for former smokers is likely due to the residual excess risk in terms of morbidity and mortality due to previous smoking history, which can persist for several years [27, 28]. This may also be due to the fact that former smokers may have quit because of health problems, thus the health status of former smokers may be generally worse as compared to that of current smokers [29].
Only four reports analysed longitudinal studies based on the general population to quantify the effect of smoking status on the combination of COVID-19 incidence and mortality [30–33]. Excluding the report by Elliott et al. [30] that analyses the same cohort used in the report by Clift et al. [31], the pooled estimates showed a statistically significant 45% excess risk of COVID-19 mortality in ever-smokers compared to never-smokers. The point estimate for current smokers versus never-smokers was even higher, although the relatively limited number of current smokers did not allow us to reach a statistically significant excess risk. We strongly encourage the dissemination of data from these cohorts based on the general population (and not on COVID-19 patients). Such cohorts are unlikely to suffer from selection or sampling biases. Using fully adjusted models, including in particular smoking-related diseases (such as chronic respiratory conditions), the risk estimates did not substantially decrease. As well discussed by Williamson et al. [32], adjusting for these comorbidities does not capture the causal effect of smoking, since these comorbidities are likely to mediate the effect of smoking on COVID-19-related death [32]. Actually, various comorbidities in the fully adjusted model act as intermediate variables on a causal pathway between exposure (tobacco smoking) and outcome (COVID-19 death). This represents a well-established over-adjustment bias [34].
Studies show that age is by far the main characteristic influencing COVID-19 severity and, to an even greater extent, mortality [35]. Accordingly, the COVID-19 case fatality rate approximately triples for each decade of age. Among COVID-19 patients, current smokers are on average younger than former smokers. For example, in an Italian multicentric study based on 1406 COVID-19 patients, the mean age of current smokers was 57.7 years, that of never-smokers was 63.8 years and that of former smokers was 66.9 years, respectively [36, 37]. Considering crude risk estimates – not adjusted, among other covariates, by age – could provide highly misleading results on the association between smoking status and COVID-19 mortality. Overall, 18 studies provided odds ratios from multivariable analysis, adjusted at least for age. To evaluate the effect of covariates in odds ratio estimates, we computed the crude odds ratios for those studies. Indeed, compared to never-smokers, the adjusted odds ratio of current smokers was consistently lower and that of former smokers consistently higher than their corresponding crude estimates. This means that the crude odds ratio estimates for current smokers are likely underestimated and those for former smokers overestimated. Given that most included studies (60% to 70% of all studies) do not provide adjusted estimates, current evidence is likely biased with a strong underestimate of odds ratios for current and an overestimate of odds ratios for former smokers. Our findings are therefore compatible with a higher risk for current versus never-smokers than for former versus never-smokers.
It is worth noting the large limitations of the studies conducted to date, including: in all the available cohort studies, smoking data are secondary, i.e. no study has been designed with the primary aim to quantify the association between smoking and COVID-19 outcomes; none of the studies report biochemically verified smoking status; time since quitting has never being taken into account, thus no smoking in the last few days might be misreported as being a former smoker; missing data on smoking status; odds ratio is time-point dependent and changes in follow-up across studies will introduce heterogeneity and problems in interpretation of the summary result; and, finally, the large majority of available studies did not provide adjusted risk estimates.
Among the limitations of the present systematic review, we provided quality assessment only for studies focusing on current versus never-smokers. However, no substantial differences have been found between good-quality studies compared to others, leading us not to perform such sensitivity analyses on other classes. Excluding publications based on languages might be considered as a limitation of the present systematic review. However, out of the 39 non-English publications excluded, only nine would have been eligible for full-text screening and most of them were of limited quality. We are therefore confident that our results are not affected by this exclusion criterion.
The original methodology used to identify eligible articles in the scientific literature is a major strength of the present systematic review. This strategy, first described by the authors of this review [14], involves the further conduction of an umbrella review, which allowed us to include 187 articles (51% of all eligible articles) that would not have been otherwise included if we would have done a traditional review only. Overall, we found 367 eligible articles, approximately tripling the number of papers found by the most comprehensive systematic reviews available so far [7, 12, 13].
For future research, we strongly recommend using large longitudinal cohort studies to quantify the association between time since stopping smoking and COVID-19 outcomes. Currently, scant, if any, information is available on the association between intensity and duration of smoking and COVID-19 progression; future studies should also provide these estimates in order to evaluate dose–risk relationships. All the studies should provide results necessarily from multivariate analyses, with relative risks estimated, at least, after adjustment for age and sex. For a correct interpretation of results, further adjustment for smoking-related comorbidities should be considered as a sensitivity analysis
In conclusion, although some degree of uncertainty should not be ruled out due to the heterogeneity of results, our comprehensive review is compatible with a 30–50% excess risk of progression of COVID-19 (severity and mortality) for current and former smokers versus never-smokers.
In this scenario, preventing serious COVID-19 complications, including mortality and disease progression, appears to be the newest good reason to avoid smoking. These results suggest that a non-negligible proportion of the 6.2 million deaths worldwide due to COVID-19 are attributable to tobacco smoking. These deaths should be added to the estimated 20 million deaths attributable to smoking that occurred since the beginning of the COVID-19 pandemic.
Points for clinical practice
Our results might suggest smoking as a salient predictor of COVID-19 outcomes. For this reason, national and international authorities should take advantage of the results of this systematic review to suggest to nonsmokers to remain free from cigarette smoking and current smokers to seek help to quit smoking to reduce serious complications of COVID-19.
Supplementary material
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Supplementary figures ERR-0191-2022.SUPPLEMENT1
Supplementary tables and references ERR-0191-2022.supplement2
Acknowledgements
We thank Elisa Borroni (Department of Clinical Sciences and Community Health, University of Milan, Milan, Italy) for her contribution to the broader systematic review. We thank Stanton Glantz (Center for Tobacco Control Research and Education, University of California, San Francisco, USA) and Ivan Berlin (Department of Pharmacology, Hôpital Pitié-Salpêtrière-Sorbonne Université, Paris, France) for their thoughtful comments in reviewing the manuscript.
Footnotes
Provenance: Submitted article, peer reviewed.
Conflict of interest: None declared.
Support statement: This research was commissioned by the World Health Organization (WHO) to S. Gallus and A. Lugo. This systematic review is an update of a broader systematic review on the possible link between tobacco and e-cigarette use and COVID-19, commissioned by the WHO to S. Gallus, A. Lugo, L. Clancy, E. Fernandez and G. Gorini.
- Received October 11, 2022.
- Accepted November 21, 2022.
- Copyright ©The authors 2023
This version is distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0. For commercial reproduction rights and permissions contact permissions{at}ersnet.org
References










