





Abstract
Endobronchial stenting is an important aspect of the practice of interventional pulmonology. The most common indication for stenting is the management of clinically significant airway stenosis. The list of endobronchial stents available on the market continues to grow. More recently, patient-specific 3D-printed airway stents have been approved for use. Airway stenting should be considered only when all other options have been exhausted. Due to the environment of the airways and the stent–airway wall interactions, stent-related complications are common. Although stents can be placed in various clinical scenarios, they should only be placed in scenarios with proven clinical benefit. The unwarranted placement of a stent can expose the patient to complications with little or no clinical benefit. This article reviews and outlines the key principles of endobronchial stenting and important clinical scenarios in which stenting should be avoided.
Abstract
Endobronchial stenting is a commonly performed procedure within interventional pulmonology and thoracic surgery. Several indications exist. Although useful, endobronchial stenting should be approached with prejudice in certain clinical conditions. https://bit.ly/3ZUtnqT
Introduction
Endobronchial stenting, a component of interventional pulmonology and thoracic surgery, is indicated for various conditions and is integral to patient care. The most unambiguous indication for an endobronchial stent is the relief of obstruction due to malignant central airway disease. The obstruction can be intrinsic, extrinsic or mixed. Endobronchial stenting is usually reserved for either extrinsic or mixed disease. However, endobronchial stenting can be utilised in benign diseases as well. Technological advancement, enhanced post-stent management and a better understanding of stent–airway interactions have improved the practice of endobronchial stenting [1]. Scenarios in which flexible bronchoscopy should be avoided have been described [2]. Airway stenting practices have been showed to vary widely [3]. This article reviews the indications for endobronchial stent placement and the pitfalls of stent placement in specific clinical scenarios (key points are summarised in table 1). In addition, post-stent management, stent removal and training in stent management are discussed.
Summary of key points to consider when evaluating stent placement in specific clinical scenarios
Endobronchial stenting philosophies
In 2018, Folch and Keyes [4] proposed that the ideal stent has specific biomechanical properties: stretch, biocompatibility, stability, migration resistance, ease of deployment and removal, resistance to tumour ingrowth and a degree of flexibility to conform to luminal irregularities. Contemporary opinion is that the ideal stent has yet to be developed. Biomedical advancements have led to the development of patient-specific 3D-printed and biodegradable airway stents [5, 6]. It is unknown whether these products will be the “ideal” stents. In the United States, more than a dozen endobronchial stents are available [1, 7]. General availability and comparatively easy deployment of metallic stents make them valuable tools; however, careful consideration of both anatomical and physiological factors must precede the deployment of an endobronchial stent.
Training in endobronchial stent placement has increased significantly over the past two decades [8, 9]. Although credentialing for specific procedures is determined by each medical centre or governing body, endobronchial stenting is typically within the purview of the interventional pulmonologist. As in other procedural or surgical specialties, it is important that interventional pulmonologists avoid cognitive bias dependence on a familiar tool [10]. Post-stenting vigilance is an essential aspect of care. Although no consensus guidelines exist, repeated follow-up bronchoscopies are generally undertaken to survey or treat stent-related complications [1, 11].
Ideally, endobronchial stenting should occur only if the clinical benefit to the patient outweighs risks and if the necessary technical skill, equipment and ancillary support to deploy, monitor and remove the stent are readily available.
Specific clinical scenarios
Malignant central airway obstruction
Malignant central airway obstruction (MCAO) can be due to lung cancer, metastatic disease, locally advanced nonpulmonary malignancy or a primary airway malignancy such as a tracheal tumour. Approximately 80 000 cases of MCAO are treated every year within the United States [12]. A significant proportion of patients with lung cancer develop MCAO [13]. It is estimated that 13% of all new lung cancer diagnoses have findings of MCAO [14]. Dyspnoea is a common symptom for which therapeutic bronchoscopy can provide quick and effective relief [15]. Patient selection remains critical [16, 17]. Several factors determine the suitability of a patient: mechanism of obstruction, underlying cause, the severity of narrowing and its extent, morphological obstruction of the site and comorbidities of the patient [18]. A commonly used classification of airway involvement is intrinsic, extrinsic or mixed. Intrinsic disease is confined to the endoluminal wall. Extrinsic disease describes compression of the airway by adjacent structures. Mixed disease compromises the airway through both intrinsic and extrinsic processes. If free of confounding factors, purely intrinsic disease can be managed with debulking. Purely extrinsic disease can be managed with endoluminal stenting, and mixed disease may need a combination of both techniques (figure 1) [13].

Purely intrinsic malignant central airway obstruction can be treated with debulking. a) A rigid bronchoscope is used to approach a primary tracheal tumour; b) after mechanical coring with the rigid bronchoscope, debulking with a cryoprobe and argon plasma coagulation to achieve haemostasis, airway patency has been re-established; c) surgical pathology results revealed the tumour to be a tracheal adenoid cystic carcinoma.
The decision to deploy an endoluminal stent should be informed by the patency of the airway and the estimation of luminal compromise contributing to the patient's dyspnoea. Symptoms of dyspnoea typically do not manifest until the airway diameter is reduced to ≥50% of the normal cross-sectional area. It is important to remember the goals of bronchoscopy in this scenario: provide symptomatic relief, improve functional status and obtain a needed diagnosis. Stents should not routinely be deployed in purely intrinsic disease if the airway can be restored to an acceptable degree. Follow-up imaging, bronchoscopy or functional testing may determine whether patients need repeat intervention.
A study assessed therapeutic rigid bronchoscopy (with dilation, neodymium-doped yttrium aluminium garnet laser resection or silicone stent insertion) in patients with MCAO necessitating intensive care unit level care; 15 stents were inserted among 32 patients, of whom 22 had extrinsic compression or combined (intrinsic and extrinsic) disease [19]. Seven patients did not need a stent after debulking. Of the 32 patients, 29 (62.5%) were immediately transferred to a lower level of care after the intervention.
In the AQuIRE Registry, 1115 procedures were performed on 947 patients with airway obstruction: intrinsic 549 (49.2%), extrinsic 161 (14.4%) or mixed 485 (43.5%). Since a patient could have multiple disease locations and multiple types of obstruction, the tracked data were not mutually exclusive. Of the 646 extrinsic or mixed obstruction cases, only 406 stents were placed. Thus 240 (37.5%) of patients with extrinsic or mixed disease were treated without the need for stenting. Stent insertion is not benign. Although causality cannot be established from registry data, upon univariate analysis, patients having their first therapeutic bronchoscopy who received a stent were more likely to die within 30 days than those who did not receive a stent (22.4% versus 9.7%) [16].
Endoluminal stenting practices vary significantly. In an observational study of 65 patients with MCAO, airway stenting occurred in 47 (56.5%) patients [15]. Airway debulking or mechanical airway dilation before stent deployment was performed in only seven patients. Among the 65 patients with MCAO, 24 (36.9%) had lung cancer and 12 (18.4%) had primary tracheal cancer. The type of airway involvement is unknown, and it is unclear why only seven patients underwent debulking or airway dilation before stent deployment. In contrast, a retrospective study evaluated 77 patients who underwent rigid bronchoscopy to manage MCAO. Stenting was not required in 51.9% of cases [20].
The most crucial aspect of endobronchial therapy for MCAO is the goal of care, which is most often palliative. Although bronchoscopic management of MCAO has been shown to improve quality of life and performance status to allow for chemotherapeutic interventions, no definitive data have proven that airway stenting itself portends a survival benefit [20]. In a randomised controlled trial, the deployment of silicone stents in symptomatic patients with malignant airway obstruction without extrinsic compression, stenting did not affect survival curves [21]. However, improvement in dyspnoea scores persisted longer, and the need for repeat therapeutic bronchoscopy was reduced in patients who received a silicone stent.
Fibrosing mediastinitis
Fibrosing mediastinitis is a rare disease heralded by compression of mediastinal structures secondary to local proliferation of invasive fibroinflammatory tissue [22]. Like vascular structures, airways can be compressed due to disease. Due to vascular congestion, airways are often hyperaemic, oedematous and bleed upon touch [23]. Vascular stents can relieve fibrosing mediastinitis related central vascular obstruction [24, 25].
Few reports discuss airway stenting in fibrosing mediastinitis. In one case series of seven patients with fibrosing mediastinitis who underwent airway stenting secondary to fibrosing mediastinitis, “bleed on touch” phenomena were noted in most patients. One patient in this series had bleeding from a minor mucosal injury secondary to balloon dilation and stent placement; the bleeding lasted 30 min. Repeat bronchoscopies were common. Among the seven patients, 32 bronchoscopies were required per year for stent maintenance. All patients in this cohort had silicone stents placed. Patients in this series did not have concomitant vascular obstruction, which may increase the risk of bleeding with bronchoscopy.
In most instances, airway obstruction in patients with fibrosing mediastinitis is funnel-shaped, which increases the risk of silicone stent migration. At the same time, ongoing inflammation may lead to excessive granulation tissue formation around self-expanding metallic stents (SEMS).
Excessive dynamic airway collapse and tracheobronchomalacia
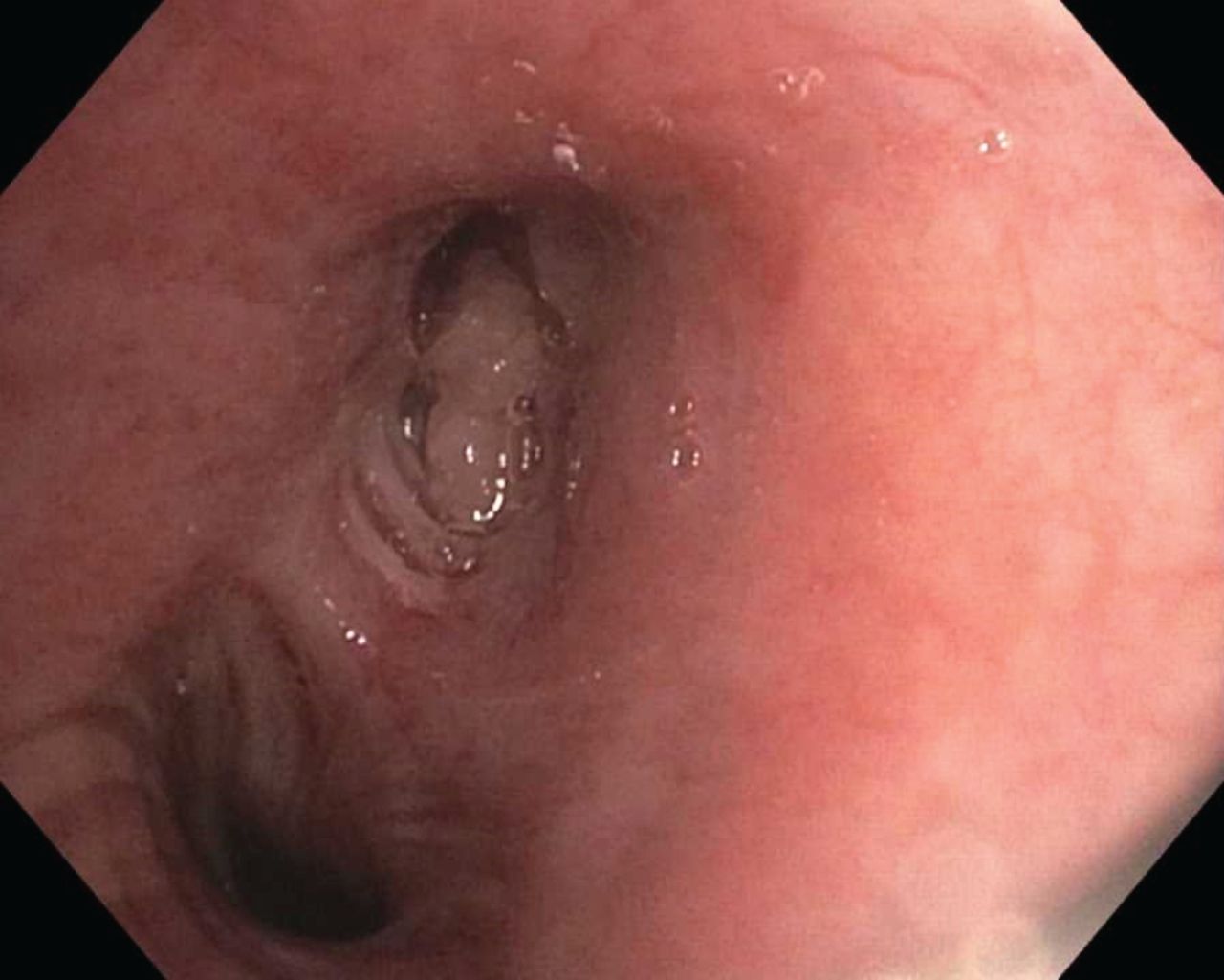
Excessive dynamic airway collapse (EDAC) and tracheobronchomalacia (TBM) are nonmalignant disorders of the central airways that can cause dyspnoea, cough and respiratory failure [26]. Both disorders result from excessive central airway collapse (ECAC). They are pathologically different processes: EDAC is a disorder of the posterior membranous wall, and TBM is a disorder of the airway's cartilaginous support structure (figure 2) [18]. There is no evidence to suggest that invasive treatments are warranted for managing EDAC.
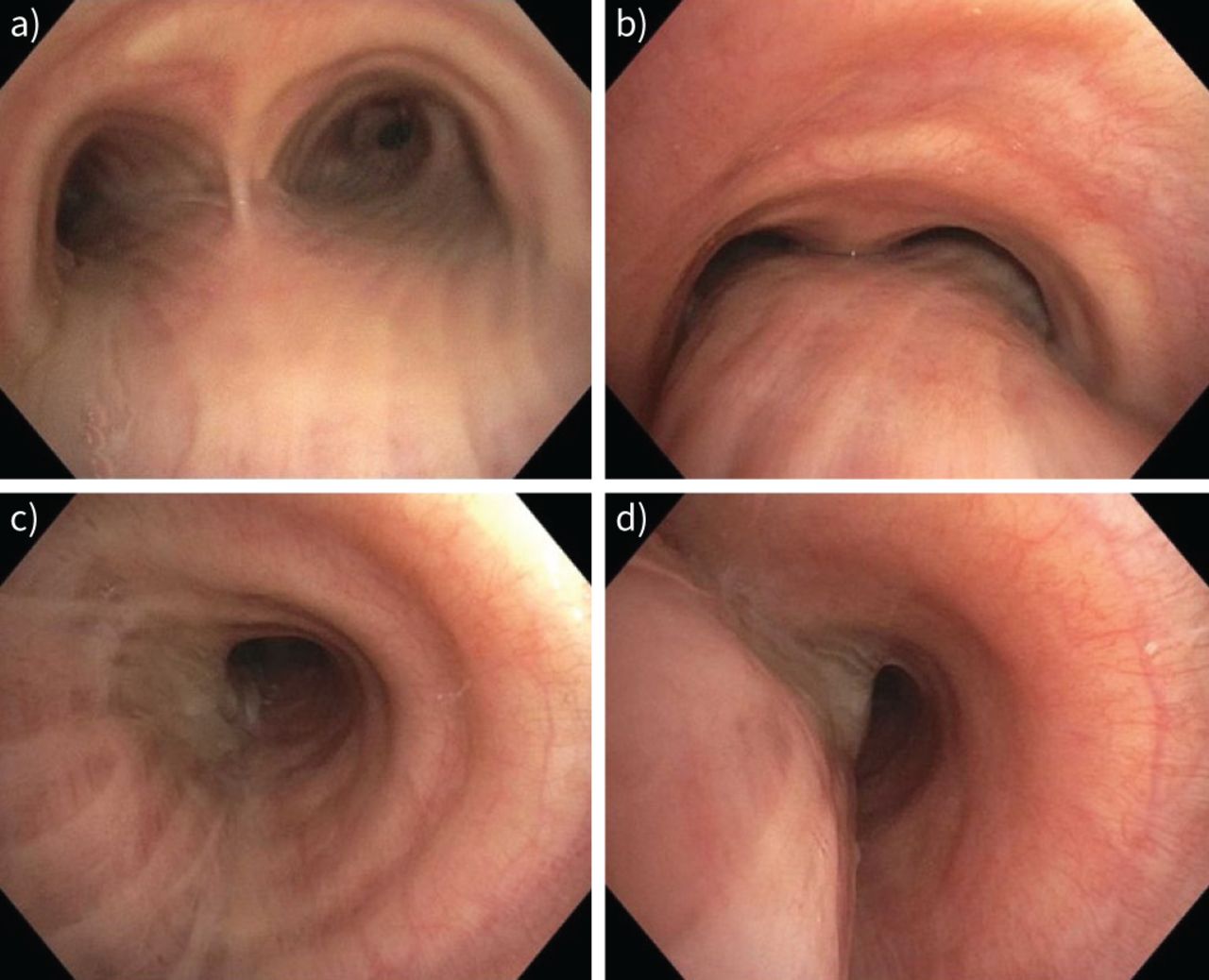
Excessive dynamic airway collapse (EDAC) is a type of excessive central airway collapse. EDAC is heralded by an exaggerated collapse of the posterior membrane of the central airways. This difference is notable when comparing a, c) inspiratory (a) distal trachea, c) left mainstem) and b, d) expiratory cross-sectional diameters endoscopically or via dynamic imaging.
EDAC is common in patients with obstructive airway disease and obesity. Due to obstructed peripheral airways, a significant pressure rise is noted during exhalation. In addition, expiration in those with obstructed airways or obesity generates increased transpulmonary pressure. These pressures result in the collapse of the weakest point, the posterior membrane [27].
Identifying EDAC on bronchoscopy should prompt a workup for the aetiology of flow limitations. The presence of EDAC does not mean it is the cause of flow limitation. Healthy people may have findings of EDAC. In one study, 78% of patients with normal spirometry exceeded the pre-defined threshold of diagnostic criteria (>50% expiratory reduction in cross-sectional area) [28]. Data suggest that EDAC may improve with concurrent small airways disease treatment. In a retrospective study, eight bilateral lung transplant recipients with COPD had pre-transplant evidence of EDAC (defined as >50% expiratory reduction in cross-sectional areas of the central airways (trachea or mainstem bronchi) by chest computed tomography (CT)). Seven of the eight patients had resolution of EDAC assessed by bronchoscopy or CT [29].
Stenting in EDAC and TBM remains controversial. Present data are limited to case series [18]. In a retrospective study of 33 patients with ECAC, uncovered self-expanding metallic stents were used to assess clinical improvement [30]. Improvements in dyspnoea and cough were noted in 88% and 70% of patients, respectively. All stents were removed at 3–21 days of insertion, with a median stenting duration of 7 days. In a small case series of 15 patients with TBM who underwent bronchoscopic treatment, 10 had silicone stents placed [31]. Seven of these stents were removed due to complications, including early migration and obstruction. In a prospective study of 58 patients with severe TBM who received endobronchial stents, stent placement was associated with increased short-term and long-term complications [32]. Similar stent-related complications in the follow-up period were noted in a smaller study that assessed silicone Y-stent placement to treat severe COPD and ECAC [33]. Murgu and Colt [34] reported that silicone stent insertion in 15 patients with ECAC immediately improved functional status, but was associated with a high stent-related complication rate.
Although the data for ECAC stent placement are limited, most studies report an increased stent-related complication rate. Limited evidence precludes firm conclusions regarding stenting in this patient population. One commonly accepted conservative practice is to reserve stent insertion only for patients with severe TBM not responding to therapy with positive pressure ventilation.
Tracheo-oesophageal fistula and dual stenting
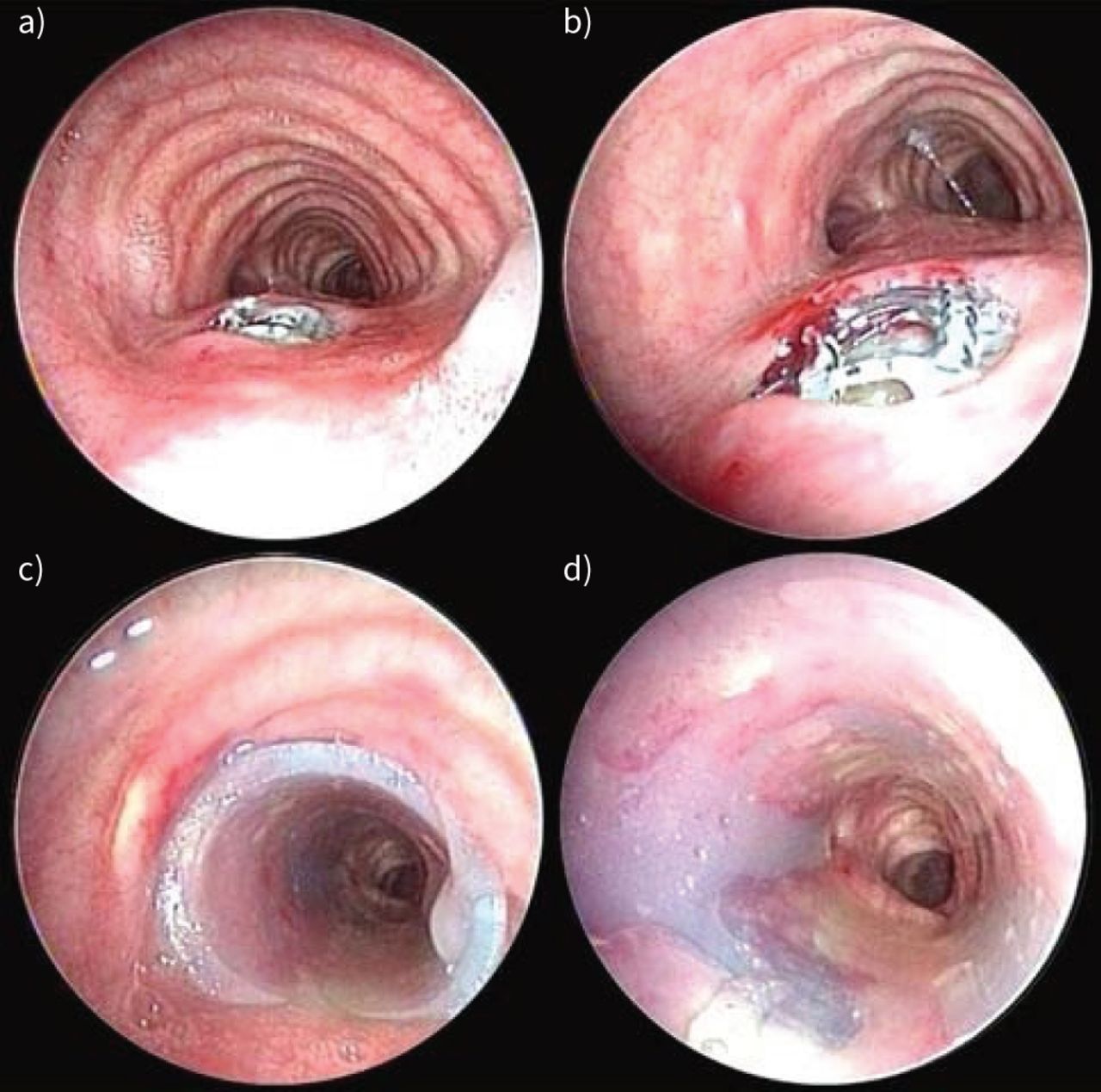
Dual stenting is the placement of stents in the airway and the gastrointestinal tract. It is considered a treatment modality for tracheo-oesophageal fistula (TOF), a type of aerodigestive tract fistula (ADF). In theory, both stents work in tandem to seal the fistula. However, managing a TOF with dual stenting in clinical practice is complex. Most of these fistulae occur in the setting of malignancy; thus, a local substrate for the healing of healthy tissue is absent. Additionally, stent-on-stent pressure can cause additional damage to surrounding tissues and enlarge the fistula. Both silicone and metallic stents offer various combinations of dual stenting (figure 3).
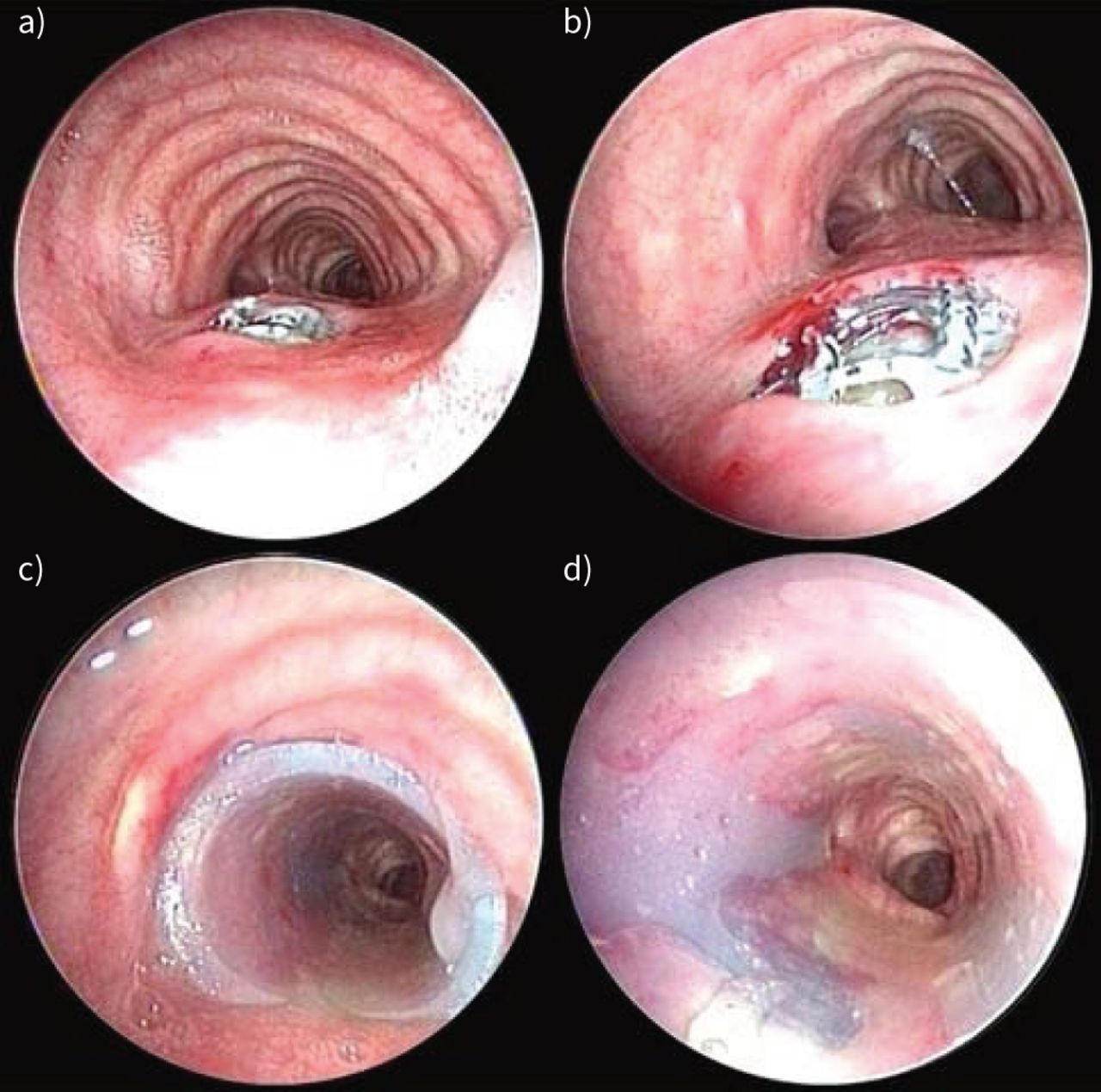
A mid-tracheo-oesophageal fistula is noted on airway examination. a, b) The oesophageal stent is eroding into the airway; c) a silicone stent is placed to cover the defect; d) the approximation of the two stents seals the defect.
In a study of 30 patients who underwent dual stenting for large ADF, the mean survival time in the dual stenting group was longer (110 days) compared to the airway stent group (24 days) [35]. Although the absolute number looks promising, the authors clearly state the implicit bias: patients receiving an airway stent may have been more ill, as these patients had advanced disease precluding the placement of an oesophageal stent.
In another study assessing patients with malignant ADF, 10 patients had both airway and oesophageal stents inserted [36]. Median survival was noted to be lower in the airway stent group (182 days) when compared to the oesophageal stent group (249) or the dual stent group (245). The authors hypothesised that patients receiving only airway stents probably had more advanced disease. A small series of eight patients with malignant ADF reported increased complications [37]. Two patients developed fistulae after dual stent placement, and two patients had a recurrence of fistulae symptoms from fistula enlargement after dual stent placement. In summary, four (50%) out of eight patients with dual stenting developed a new fistula or experienced enlargement of an existing fistula.
Some evidence suggests that dual stenting achieves improved palliation. A study that assessed double stenting for palliation in 70 patients with oesophageal cancer noted improvements in dyspnoea, dysphagia and performance status [38].
In practice, concerns often arise regarding the sequence of dual stenting. The hypothetical risk of stenting the oesophageal side first is loss of the airway. Data are equivocal. In the study by Roseira et al. [38], 41 (59%) out of 70 patients had oesophageal stents placed first with no reports of airway compromise. Conversely, in a case series of eight patients with combined oesophageal and tracheobronchial stenosis, data suggested that stents should be placed in the airway first [37]. Two of the eight patients experienced respiratory distress after oesophageal stent placement.
Nonetheless, dual stenting for TOF should be considered very carefully based on the pathology, fistula size, prior treatments, local anatomy and overall prognosis.
Conditions involving distal airways
Distal airway stenting is controversial within interventional pulmonology and thoracic surgery. Endoluminal stents are available in various sizes, including small stents that can be placed into lobar orifices [18]. Some vascular stents have been placed into small airways [39]. Physiological benefit of placing stents in the lobar bronchi remains unproven (figure 4).
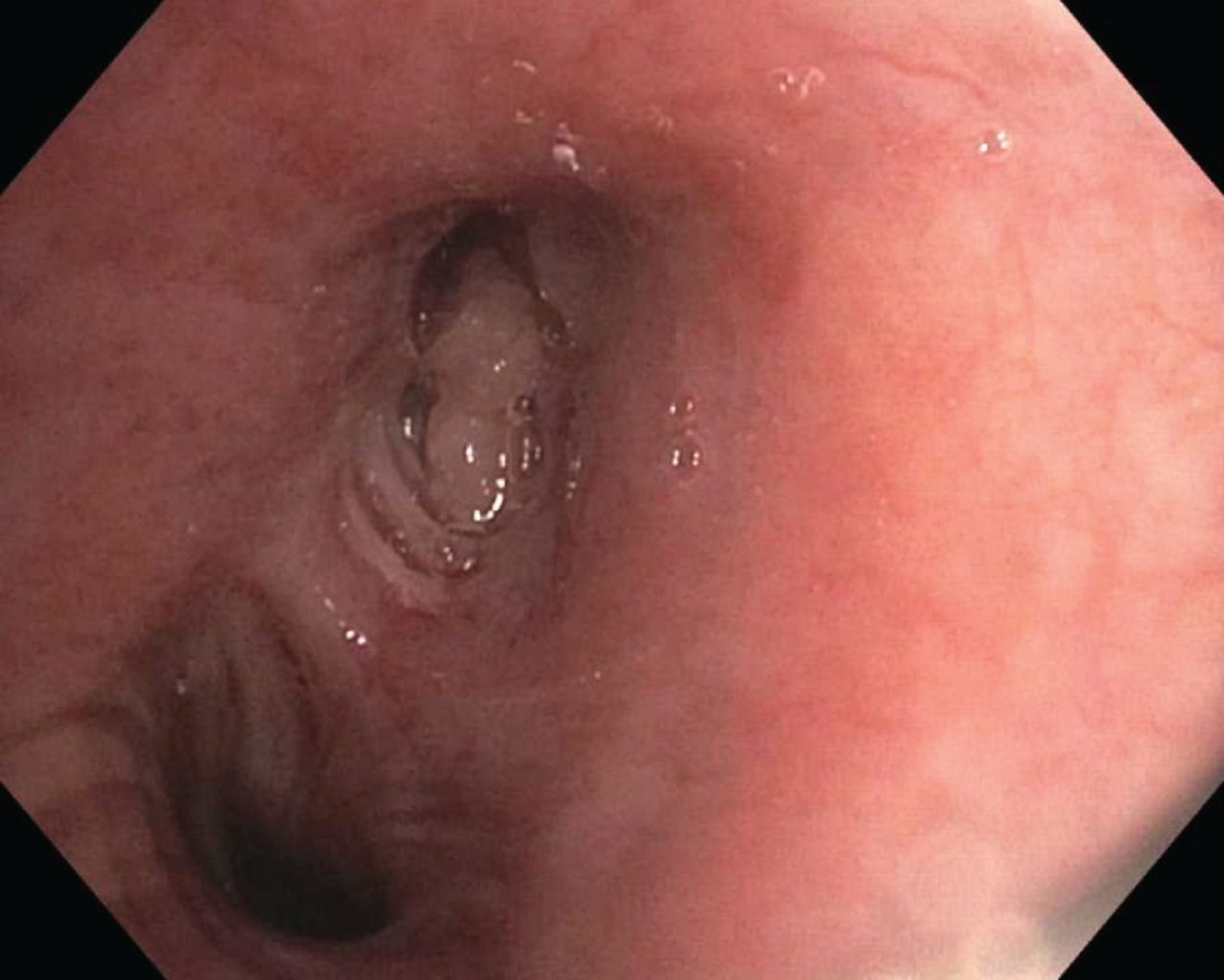
Lobar salvage has questionable physiological benefit, which is probably more pronounced in the setting of malignant airway disease. The left upper lobe bronchus was noted to be fully occluded; concurrent endobronchial ultrasound needle aspiration showed metastatic disease with poorly differentiated adenocarcinoma. The patient underwent local radiation and systemic chemotherapy; endobronchial therapeutic intervention was not undertaken due to the lack of central airway involvement and the malignant nature of the airway disease.
In a study by Sethi et al. [39], 122 stents (iCAST; Atrium, Hudson, NH, USA) were deployed in 38 patients with lobar bronchial stenosis, 55% with benign disease (figure 5). 95% of patients reported symptomatic improvement upon follow-up between 6 and 12 weeks post-intervention. The assessment metric was unspecified and focused on quality of life. Thus, symptom improvement may have resulted from stent placement or other factors. Pre- and post-stent radiographic evaluation was available for 34 patients, 75% of whom had radiographic improvement (resolution of lobar atelectasis and improvement or the resolution of lobar infiltrates). Pre- and post-procedure pulmonary function tests were available for 16 patients, 14 of whom were lung transplant recipients. 15 of the 16 patients demonstrated an average forced expiratory volume in 1 s (FEV1) improvement of 12.3%. Modifications in transplant care for these patients (a majority of whom were transplant recipients) were not reported. Although a minimal clinically important difference has been established for patients with COPD, a metric for lobar stenosis has not been established [40].

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
An iCAST is a vascular stent applied to manage bronchial stenosis. An iCAST stent is being deployed under fluoroscopic guidance in a patient with lobar stenosis. Fluoroscopically visible markers (such as paper clips) can assist in marking the proximal and distal stent landing points.
A retrospective study assessed therapeutic bronchoscopy for patients with distal airway stenosis. Five of the 11 patients were treated with stents. When the stented group was compared to the nonstented group, no improvements in the stented group were noted in lung function, the number of bronchoscopies per month or airway patency [41]. A variety of stents were used for the patients in this study. Interestingly, the never-stented patients had a greater average increase in their change in FEV1 (28%) than the stented patients (−25%).
In another study, 21 stents (iCAST™) were placed among 18 patients with malignant or benign airway disease. Only three stents were placed in nonlobar locations (one in the right mainstem, one in the left mainstem and one in the trachea). Significant improvements in the modified Medical Research Council dyspnoea scale were noted (grade 2, improvement from grade 3). Improvements in self-reported respiratory symptoms were noted in 78% of patients, and radiographic improvement in 83% of patients [42].
More data are now available for lobar stenting in patients who have received a lung transplant. In a single-centre retrospective study of 376 stents placed among 50 transplant recipients, 70 (19%) stents were placed in lobar airways [43]. Only two major complications were noted; neither involved a stent placed into a lobar airway.
Shepherd [44] has raised valid concerns regarding lobar stenting. More distal placement inherently makes retrieval more challenging; fluoroscopy may have to be used. Additionally, stent crushing from coughing (without re-expansion), mucus plugging due to the placement of the stent in smaller airway diameters, and migration are also concerns [44]. A physiological benefit of lobar salvage has not been proven. Furthermore, the placebo effect has not been evaluated.
A specific clinical scenario regarding lobar stenting warrants discussion: lobar stenting in the allograft of a single-lung transplant recipient. Airway complications post-transplantation are common. For example, bronchial stenosis affects 4–25% of lung transplant recipients [45–48]. The management of lobar stenosis with stent placement in a single-lung transplant patient risks the development of stent-related complications in a patient with a heavily diseased contralateral lung. In a series of 54 lung transplant patients who underwent endobronchial stenting, 36 were single lung transplant recipients [11]. Although a subgroup analysis of single-lung transplant recipients was not performed, the overall incidence of stent-related complications was comparable to previously reported studies (3–27%) [11, 48, 49]. Current data do not support single lung transplant as a contraindication to the stenting of a distal airway. However, the additional challenges of stent-related complications must be considered before stent deployment.
Subglottic stenosis
Subglottic stenosis has several causes [50]. The definitive treatment is tracheal reconstruction. However, sometimes patients are not fit for surgery or decline surgical intervention. Therefore, a bronchoscopic intervention should be considered only in these special circumstances or for emergent airway obstruction.
In a pivotal study by Gelbard et al. [51], patients with idiopathic subglottic stenosis experienced a higher recurrence rate with endoscopic dilation than with cricotracheal resection. To mitigate the possibility of stent dislodgement, external stent fixation can be considered [52, 53]. Suturing the stent to the anterior neck is thought to prevent it from dislodging. Six cases of post-operative infection at the external fixation site were noted in one case series of seven patients with subglottic stenosis who received straight silicone stents with external fixation [54]. However, no stent dislodgements were noted. Treatment for subglottic stenosis includes stents and Montgomery T-tubes [55, 56].
Due to the documented risk of excessive and possibly obstructive granulation tissue, uncovered metallic stents or partially covered metallic stents are not ideal for managing idiopathic subglottic stenosis [57]. Fully covered metallic stents and silicone stents have also been used, yet data are insufficient to support the selection of one over another [50].
Relapsing polychondritis
Relapsing polychondritis (RP) is a rare immune-modulated condition heralded by the inflammation of cartilaginous structures, including the respiratory tract. Laryngotracheal involvement is estimated to affect >50% of patients, with airway strictures affecting almost 25% [58]. In a series of 295 patients, ∼70% of patients had airway involvement [59]. Chest CT can reveal diffuse thickening of the trachea, with sparing of the posterior membrane. Clinical manifestations can vary based on the affected organs, including dyspnoea, cough, stridor and hoarseness in patients with laryngotracheal involvement [60]. In a case series by Ernst et al. [60], malacia, subglottic stenosis and focal bronchial stenosis were the most common airway manifestations. Medical management is the cornerstone of treatment. Bronchoscopic dilation and stenting can provide symptomatic relief [61]. However, due to the inflammatory nature of the disease, airway stenting must be approached with caution.
In a case series of five patients with severe airway RP managed with airway stenting, 17 self-expandable metallic stents were placed [62]. One patient died 1 week after the stent placement, suspected to be due to respiratory failure secondary to persistent airway collapse distal to the stent. Long-term follow-up data are not available. However, several case reports cite immediate clinical improvement with stenting in patients with RP-related airway disease [63, 64]. The most extensive case series of airway stenting in this patient population included 27 patients [65]. A total of 58 uncovered metallic stents were placed. During follow-up, respiratory adverse events were noted in 16 (59.3%) patients. However, most of these were not serious, including cough or the development of a foreign body sensation. In addition, haemoptysis was noted in five (18.5%) patients, and stent fractures in four (14.8%) patients.
In summary, the data supporting airway stenting in patients with RP are limited to case series without long-term follow-up. Additionally, the question of whether the interaction of the stent with actively inflamed airways increases the risk of stent-related complications remains unanswered.
Post-stent management
Regardless of the indication for stent placement, post-stent management is essential. Unlike stents in vascular structures, the urinary tract or biliary tree, stents in the gastrointestinal tract and respiratory tract are constantly exposed to the environment. Recognised stent complications include displacement, mucus plugging, granulation tissue formation and fracturing.
Stent management is not standardised. It often combines humidifying agents and mucolytics to prevent thick secretions that cannot be easily cleared. Post-stent bronchoscopy may detect complications before they become clinically apparent. In a retrospective study by Lee et al. [66] that assessed 134 patients who had airway stents placed, the presence of stent complications noted on follow-up bronchoscopy was not associated with the patient's symptom status. 94 patients in this cohort had a follow-up bronchoscopy performed, 35% of which were asymptomatic. The odds ratio for the presence of any stent-related complications and the presence of any symptoms was 1.88 (95% CI 0.79–4.45).
Some patients live far away from centres experienced in airway stenting or cannot adhere to stent maintenance recommendations, which limits comprehensive stent care. If the availability of post-stent management is uncertain, alternative options to endobronchial stenting should be considered.
Stent removal is an important aspect of post-stent management that warrants specific mention. If not undertaken carefully, disastrous complications can occur [67, 68]. In general, stenting should be utilised to maintain airway patency, while additional treatment options with direct therapeutic benefit are engaged. The impact on life expectancy may be lower in patients with airway obstruction due to malignant disease than in those with benign central airway obstruction. Malignant central airway obstruction can be caused by a lung cancer tumour of stage 2 or greater, primary malignancy of structures surrounding the airway, or metastatic disease. In benign disease, the airway obstruction itself could arise from a localised process that has little impact on the patient's life expectancy, such as idiopathic subglottic stenosis. Regardless of aetiology, the goal is to remove the stent as soon as possible.
A variety of airway stents are currently on the market. Depending on design and size, some can be placed via flexible bronchoscopy. With a few exceptions, silicone stents are exclusively placed via a rigid bronchoscope [69]. The use of a rigid bronchoscope allows for airway patency and control and the deployment of the tools necessary for stent removal. In a series that documented the removal of 19 SEMS, rigid bronchoscopy was used for all but one stent removal [70].
In most scenarios, stent placement is more straightforward than stent removal. Stent care requires continuous vigilance and continual reassessment for stent removal. In an ideal scenario, a stent should be removed as soon as possible. Some data suggest that uncovered self-expanding metallic stents can be removed safely within 6–8 weeks of placement. In a series that assessed patients with life-threatening bronchial dehiscence post-lung transplantation, five out of seven patients had their stents removed 21–390 days after stent placement. It should be noted that in three of the patients, the stent had to be removed piecemeal while the surrounding ingrowth of granulation tissue was treated with a laser [71].
Stent technology continues to advance. In the past, Y-stents could only be placed via rigid bronchoscopy or direct laryngoscopy [4]. Recently, a self-expanding covered metallic Y-stent has been deployed in the United States, and which is now available for use [72]. As new stents become available, post-market surveillance data must be tracked carefully.
Training
Endobronchial stenting should be done only by trained interventional pulmonologists, thoracic surgeons or, in isolated trachea disease, otorhinolaryngologists. Interventional pulmonology training standards are established by local, regional and national authoritative bodies. Competence standards have been published in both Europe and North America. An interventional pulmonology training syllabus has been introduced, which detailed a core training curriculum [73]. Nearly 40 accredited interventional pulmonology fellowships are offered in North America [74]. The Multisociety Interventional Pulmonology Fellowship Accreditation Committee recommends a minimum institutional volume of 50 rigid bronchoscopies and 20 endobronchial stenting procedures for an interventional pulmonology fellowship to be accredited [75]. The document also states “The determination of competence to practice independently as an interventional pulmonologist remains the responsibility of the interventional pulmonology fellowship programme director and faculty, interventional pulmonology board certification process, and institutional credentialing committees”. At the time of writing, 448 American Association for Bronchology and Interventional Pulmonology board-certified physicians are in practice [73]. In 2022, the Accreditation Council for Graduate Medical Education approved the accreditation of interventional pulmonology as a subspeciality [76].
Customised patient-specific stents
Customised patient-specific printed airway stents are believed to have a better stent–airway conformation than pre-manufactured airway stents in generic sizes [77]. The stent is created from a mould derived from the patient's airway. The first placement of a customised patient-specific stent was in France in 2017 [78]. Multiple experiences, series and perspectives with customised patient-specific printed airway stents have since been published [5, 78, 79]. A 10-patient clinical trial that assessed the safety and efficacy of custom stents in patients with complex airway stenosis showed a high rate (90%) of great stent–airway congruence evaluated by single post-deployment CT scans [80]. In 2020, customised patient-specific printed airway stents were approved by the United States Food and Drug Administration [81]. Customised patient-specific printed airway stents may be the next generation of endobronchial stents. However, long-term data are pending. The niche field of biodegradable customised patient-specific airway stents (4D: time dimension) is also being studied [82]. Therefore, at this time, it is unclear whether these custom stents will become the ideal stent.
Points for clinical practice
Endobronchial stenting is a commonly performed procedure within interventional pulmonology and thoracic surgery.
The maintenance of airway patency in patients with malignant central airway obstruction is one of the most common indications for endobronchial stenting.
Not all cases of malignant central airway obstruction require endobronchial stenting.
Caution or even avoidance of endobronchial stenting should be exercised in certain pathologies: fibrosing mediastinitis, excessive central airway collapse, TOF, lobar stenosis, subglottic stenosis and relapsing polychondritis.
Conclusions
Endobronchial stenting has a rightful place within interventional pulmonology and thoracic surgery. Stents are valuable tools in the management of airway stenosis; they serve as a framework to maintain airway patency. The tenet of airway stenting is simple: it is not a treatment, but a temporary measure to permit effective treatment. Stent placement should be carried out only by a well-trained interventional pulmonologist in a setting with all desirable stent sizes and designs readily available. Equally important, the equipment and expert personnel for stent removal and management of stent-related complications must be available when needed, including collaborators in thoracic surgery, otorhinolaryngology, interventional radiology and anaesthesiology. A post-stent management plan that the patient can execute is a necessity. Finally, caution should be exercised before deploying stents in situations with a high risk-to-benefit ratio.
Acknowledgements
The authors thank Linda Conry (Arkansas, USA) for editorial assistance in preparing this manuscript, and Otis B. Rickman (Vanderbilt University Medical Center, Vanderbilt University School of Medicine, Nashville, TN, USA) and Benjamin P. Young (University Hospitals, Case Western Reserve University School of Medicine, Cleveland, OH, USA) for providing figures.
Footnotes
Provenance: Submitted article, peer reviewed.
Conflict of interest: S.K. Avasarala has consulted for VisionAir Solutions (Cleveland, OH, USA). H. Dutau is a consultant for Novatech SA (La Ciotat, France). A.C. Mehta has no conflicts of interest to disclose.
- Received October 4, 2022.
- Accepted January 13, 2023.
- Copyright ©The authors 2023
This version is distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0. For commercial reproduction rights and permissions contact permissions{at}ersnet.org
References










