





Figures
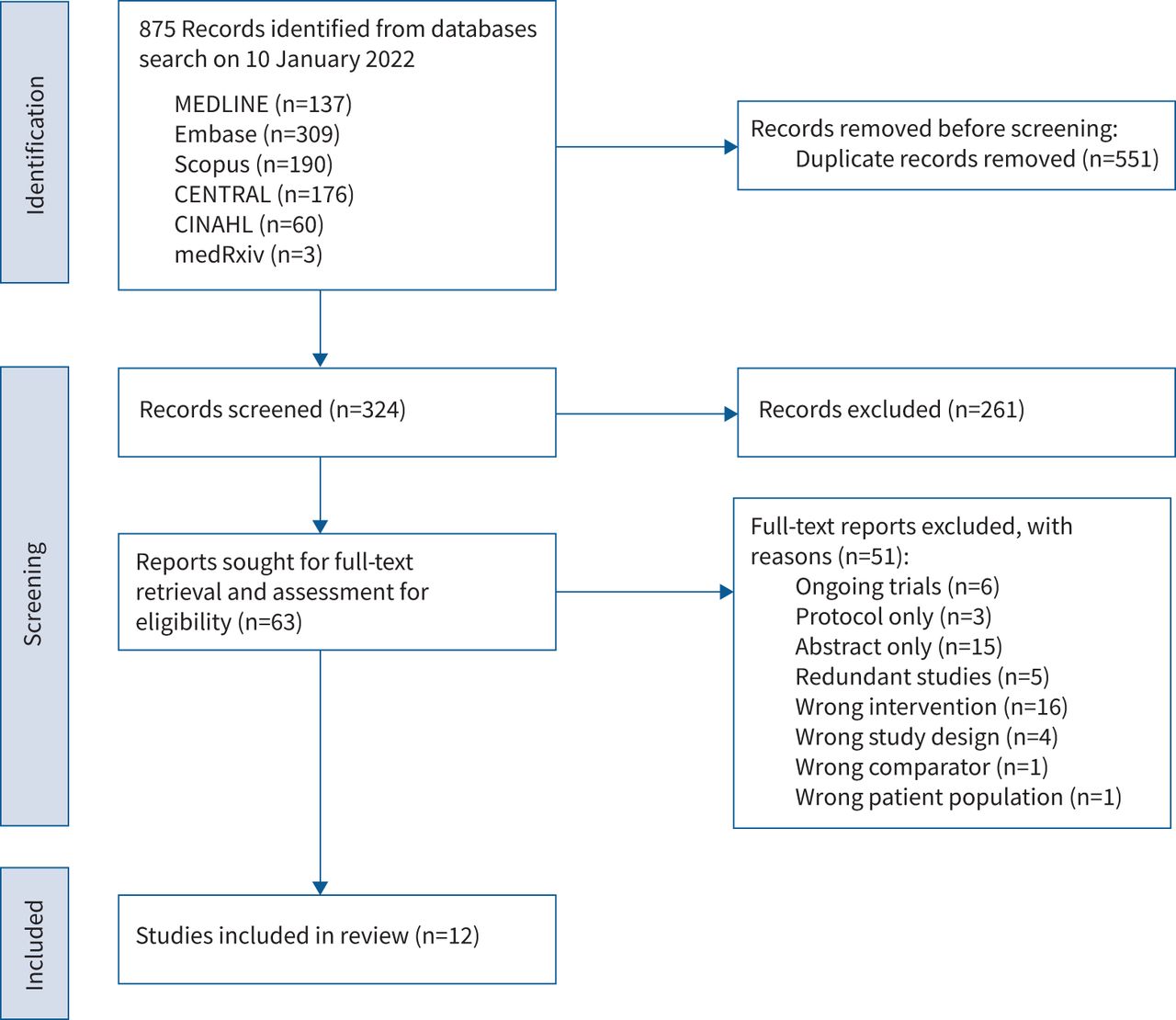
- FIGURE 1
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram of the records identified and assessed during the study selection process. CENTRAL: Cochrane Central Register of Controlled Trials; CINAHL: Cumulative Index to Nursing and Allied Health Literature.
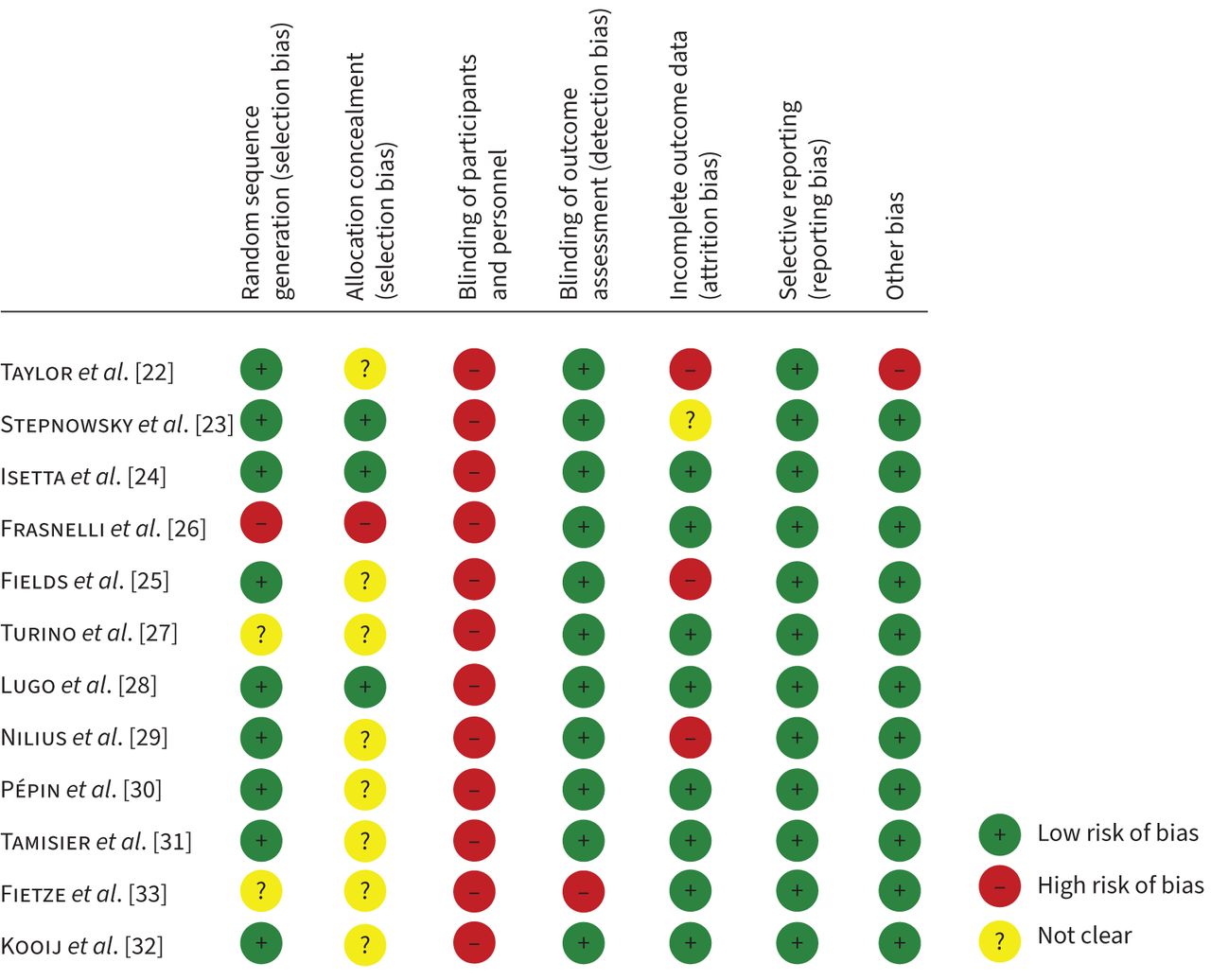
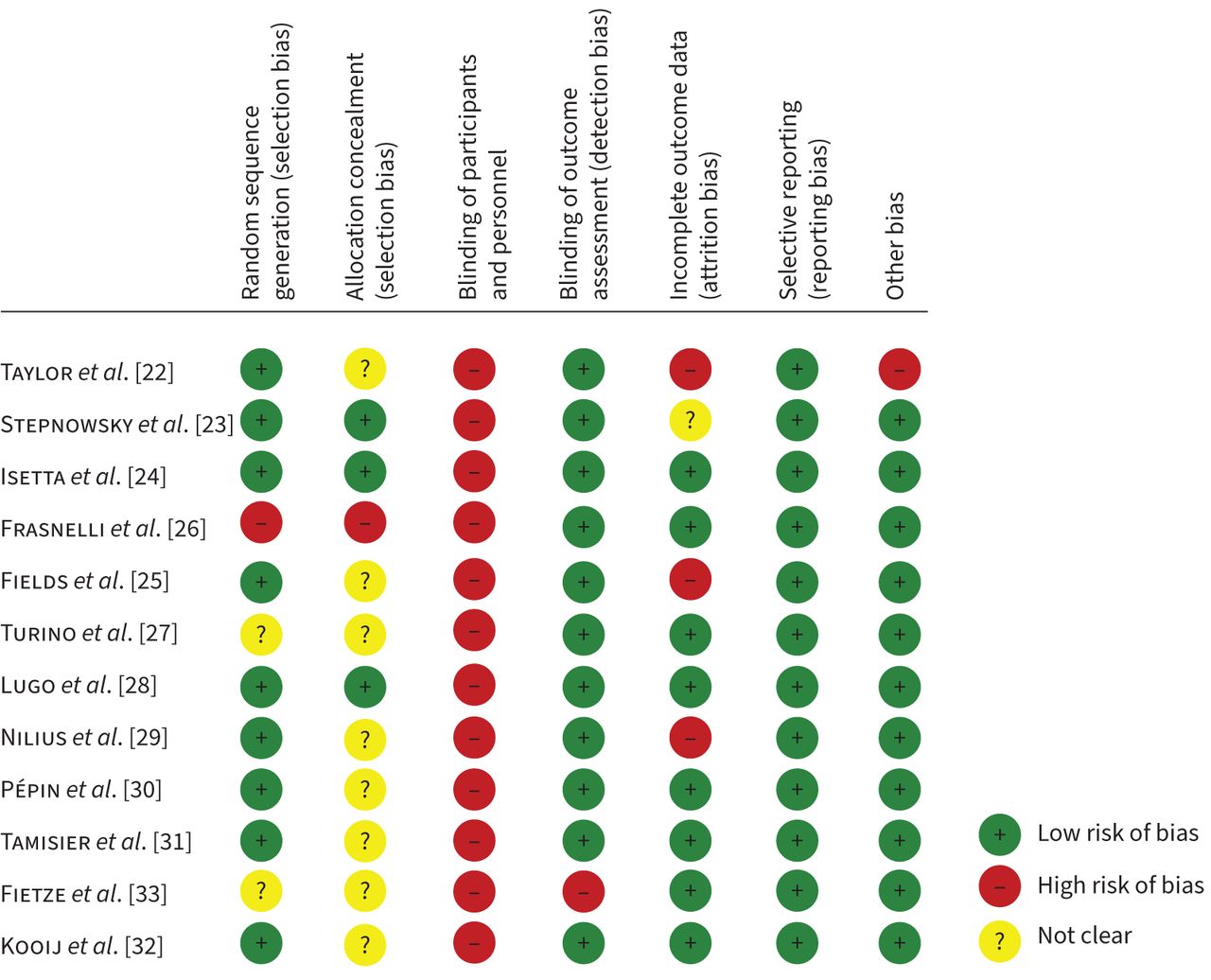
- FIGURE 2
A summary of the risk of bias assessment for the included studies.
- FIGURE 3
Forest plot of the mean difference in patient-reported sleepiness scores, assessed by the Epworth Sleepiness Scale, in patients randomised to virtual compared to in-person consultations for the management of obstructive sleep apnoea/hypopnoea syndrome. The diamond represents the 95% confidence interval of the pooled estimate of the mean difference. df: degrees of freedom; IV: inverse variance.
- FIGURE 4
Forest plot of the mean difference in continuous positive airway pressure usage (hours per night) in virtual compared to in-person consultations. The diamond represents the 95% confidence interval of the pooled estimate of the mean difference. df: degrees of freedom; IV: inverse variance.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Tables
- TABLE 1
Population, intervention, control and outcomes framework for inclusion and exclusion criteria
Population Adults with a clinical diagnosis of OSAHS, either naïve or established users of CPAP; recruited from any healthcare or community setting. Studies were excluded if they investigated patients with other types of sleep disorders such as central sleep apnoea. Intervention Any form of a virtual consultation between a patient and a healthcare provider. This included either synchronous or asynchronous communications made via telephone or videoconferencing, with or without real-time telemonitoring of CPAP. No limitations were imposed regarding the number of consultations, methods of CPAP initiation or the duration of consultations. Trials that investigated automated interventions, without direct input from a healthcare professional, were excluded. Comparator The comparator group were allocated to a clinical in-person consultation, with or without real-time telemonitoring of CPAP therapy. Outcomes The primary clinical outcome was subjective sleepiness, assessed by the Epworth Sleepiness Scale and the primary organisational outcome was cost-effectiveness of the intervention.
Additional outcomes were clinical, patient and/or clinician-reported, and environmental impact outcomes (see supplementary material, section 2, for definitions).Study design Studies were included if they were randomised controlled trials, quasi-randomised controlled trials or controlled clinical trials. CPAP: continuous positive airway pressure; OSAHS: obstructive sleep apnoea/hypopnoea syndrome.
- TABLE 2
Summary of the included studies
Study (year, country) Study design and overall RoB Number of participants (n=1823) Population description Intervention Intensity and duration Mode of delivery Main findings Taylor et al. [22] (2006, USA) RCT
FU: 30 days
High RoBTotal: 114
VC: 56
IP: 58Adult patients with OSA who were initiating CPAP therapy Telemonitoring via the Health Buddy.
OSA patients with “high-risk” responses were contacted within 24 h.Patients were contacted as needed to resolve issues Telephone consultation ESS was not reported for post-intervention follow-up Stepnowsky et al. [23] (2007, USA) RCT
FU: 2 months
Moderate RoBTotal: 45
VC: 24
IP: 21Adult patients newly diagnosed with OSA Telemonitoring via flow generator data.
Objective and subjective patient reports triggered patient contact.Patients were contacted as needed based on a pre-defined clinical pathway Telephone consultation No significant differences in ESS scores between the study groups at baseline and post-intervention Isetta et al. [24] (2015, Spain) RCT
FU: 6 months
Moderate RoBTotal: 139
VC: 69
IP: 70Adult OSA patients requiring CPAP treatment Telemonitoring via a website developed for this study.
Input evaluation triggered patient contact.Virtual consultations via Skype were scheduled at 1 and 3 months.
Consultation duration: 38.97±12.04 min.Video consultation Improvement in ESS at 6 months, but no significant difference in change from baseline between the study groups.
The telemedicine-based strategy had a lower total cost compared to standard care.Frasnelli et al. [26] (2015, Switzerland) CCT
FU: 30 days
High RoBTotal: 223
VC: 113
IP: 110Adult patients with sleep apnoea Telemonitoring via CPAP.
A colour-coded algorithm triggered patient contact.Patients were contacted as needed for a duration of ∼30 min Telephone consultation ESS was not reported for post-intervention follow-up Fields et al. [25] (2016, USA) RCT
FU: 3 months
Moderate to high RoBTotal: 60
VC: 32
IP: 28Adult patients with OSA from two community-based outpatient centres Telemonitoring via APAP.
Scheduled follow-up contact and if needed.Initial evaluation visit for 40 min with a 10 min (or less) follow-up call at week 1.
Virtual consultations scheduled at 1 and 3 months for 20 min each.Initial evaluation via real-time CVT.
Telephone consultation for follow-up.No significant difference in the change of ESS scores from baseline to 3 months follow-up between the study groups Turino et al. [27] (2016, Spain) RCT
FU: 1 and 3 months
Moderate RoBTotal: 100
VC: 52
IP: 48Adult patients with newly diagnosed OSA requiring treatment with CPAP Telemonitoring via MyOSA – Oxigen Salud web database.
Automatic alarms triggered patient contact.Patients were contacted as needed to resolve issues Telephone consultation ESS was not reported for post-intervention follow-up.
The total average cost per randomised patient was 28% lower in the VC group than in the IP standard care group.Lugo et al. [28] (2019, Spain) RCT
FU: 3 months
Moderate RoBTotal: 186
VC: 94 (32 with CPAP)
IP: 92 (40 with CPAP)Adult patients with suspected OSA who were referred to the sleep unit Telemonitoring via CPAP.
Input in a custom web application triggered patient contact.Virtual consultations were scheduled at 3, 6 and 12 weeks for no more than 15 min each Video or telephone consultation No significant differences in the ESS scores between the study groups.
The costs of the VC were cheaper than those for IP standard care and the Bayesian analysis showed that the VC was cost-effective.Nilius et al. [29] (2019, Germany) RCT
FU: 6 months
Moderate to high RoBTotal: 80
VC: 40
IP: 40Adult OSA patients who had suffered an ischaemic stroke within the last 3 months Telemonitoring.
A colour-coded algorithm triggered a more detailed evaluation and patient contact if needed.Patients were contacted as needed for a duration of 5 min Telephone consultation VC group had a significantly lower ESS scores at 6 months follow-up Pépin et al. [30] (2019, France) RCT
FU: 6 months
Moderate RoBTotal: 306
VC: 157
IP: 149Adult patients with severe OSA and high cardiovascular risk Telemonitoring via CPAP and the multimodal system.
Automatic algorithms triggered patient contact.Patients were contacted as needed.
Regular assessments at day 8 and months 1 and 6.Telephone or teleconsultation ESS scores significantly improved in both study groups, but the size of improvement was significantly higher in the VC group Tamisier et al. [31] (2020, France) RCT
FU: 6 months
Moderate RoBTotal:206
VC: 102
IP: 104Newly diagnosed adult patients with OSA and low cardiovascular risk who were referred for CPAP therapy Telemonitoring via CPAP and the multimodal system.
Automatic algorithms triggered patient contact.Patients were contacted as needed based on an automatic algorithm Telephone or teleconsultation ESS scores significantly improved in both study groups, with no significant difference between the groups Fietze et al. [33] (2021, Germany) RCT
FU: 6 months
Moderate to high RoBTotal: 224
VC: 110
IP: 114Adult patients with moderate to severe OSA Telemonitoring via APAP.
Pre-defined criteria triggered patient contact.Patients were contacted as needed based on pre-defined criteria Telephone consultation Change from baseline to 6 months in ESS scores was not significantly different between the two groups Kooij et al. [32] (2021, Netherlands) RCT
FU: 4 weeks, 12 weeks, 24 weeks
Moderate RoBTotal: 140
VC: 70
IP: 70Adult patients diagnosed with moderate or severe OSA who require CPAP treatment Telemonitoring.
Not achieving pre-defined objectives (e.g. adherence and residual AHI) triggered patient contact.Patients were contacted as needed
Scheduled follow-ups at 1 and 4 weeksVideo and telephone consultation ESS was not reported for post-intervention follow-up AHI: apnoea–hypopnoea index; APAP: automatically adjusting positive airway pressure; CCT: controlled clinical trial; CPAP: continuous positive airway pressure; CVT: clinical video tele-health; ESS: Epworth Sleepiness Scale; FU: follow-up duration; IP: in person; OSA: obstructive sleep apnoea; RCT: randomised controlled trial; RoB: risk of bias; VC: virtual consultation.
- TABLE 3
Participant baseline characteristics
Study (year) Number of participants (n=1823) Age (years) Gender (male %) BMI (kg·m−2) AHI (events per hour) VC IP VC IP VC IP VC IP Taylor et al. [22] (2006) Total: 114
VC: 56
IP: 5845.8±10 44.6±8.5 66 71 NR NR NR NR Stepnowsky et al. [23] (2007) Total: 45
VC: 24
IP: 2160±10.8 58±13.7 98 98 33.3±4.9 30.5±5.1 44.8±17.9 37.6±14.3 Isetta et al. [24] (2015) Total: 139
VC: 69
IP: 7051.0±8.9 47.0±10.9¶ 85 87 32.8±7.3 33.6±8.3 45 (35–70)# 52 (35–62)# Frasnelli et al. [26] (2015) Total: 223
VC: 113
IP: 11055 (47–63)# 55 (45–61)# 76 78 NR NR 37 (23–62)# 40 (20–69)# Fields et al. [25] (2016) Total: 60
VC: 32
IP: 2846.7±13.1 58.2±14.4 93 94 33.2±6.0 32.9±3.8 32.0±33.9 30.1±30.0 Turino et al. [27] (2016) Total: 100
VC: 52
IP: 4856 ±13 54 ±12 77 77 35±7 35±7 52±25 53±26 Lugo et al. [28] (2019) Total: 186
VC: 94 (32 with CPAP)
IP: 92 (40 with CPAP)50.39±11.31 50.82±12.15 70 66 29.97±6.19 31.50±10.91 24.68±21.01 33.60±28.96 Nilius et al. [29] (2019) Total: 80
VC: 40
IP: 4055.4±10.4 58.6±9.3 73 73 31.7±5.4 30.1±6.6 41.2±19.0 37.6±18.4 Pépin et al. [30] (2019) Total: 306
VC: 157
IP: 14960.8 (53.8–66)# 61.8 (54.7–66.1)# 73 74 32.4 (29.6–36.5)# 31.4 (28.1–35)# 47 (35–60.5)# 45 (35.4–61.2)# Tamisier et al. [31] (2020) Total: 206
VC: 102
IP: 10451.9 (44.8–58.8)# 49.4 (40–57.9)# 58 68.3 30.5 (27.5–34.9)# 31.3 (26.6–35.2)# 45 (34–58)# 42.3 (33–57.6)# Fietze et al. [33] (2021) Total: 224
VC: 110
IP: 11453.6±11.8 53.1±10.6 83 79 32.8±6.4 31.7±5.6 35.3±17.6 37.0±20.3 Kooij et al. [32] (2021) Total: 140
VC: 70
IP: 7052.3±12.4 54.3±11.9 83 76 BMI >30
n=51 (73%)BMI >30
n=46 (66%)31 (22–46)# 30.5 (20–42)# Data are presented as n or mean±sd, unless otherwise stated. AHI: apnoea–hypopnoea index; BMI: body mass index; CPAP: continuous positive airway pressure; IP: in person; NR: not reported; VC: virtual consultation. #: Median (interquartile range). ¶: Significantly different value from the other group.
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Supplementary material ERR-0180-2022.SUPPLEMENT










