





Abstract
Background Conflicting literature exists regarding the risk factors for exacerbations among pregnant women with asthma. This systematic review and meta-analysis aimed to determine risk factors for asthma exacerbations during pregnancy.
Methods Electronic databases were searched for the following terms: (asthma or wheeze) and (pregnan* or perinat* or obstet*) and (exacerb* or flare up or morbidit* or attack*).
All studies published between 2000 and 24 August 2021 were considered for inclusion if they reported at least one potential risk factor of asthma exacerbations in pregnant women with asthma. Of the 3337 references considered, 35 publications involving 429 583 pregnant women with asthma were included. Meta-analyses were conducted to determine mean difference in risk factor between exacerbation groups, or the relative risks of exacerbation with certain risk factors. Good study quality was found through the Newcastle-Ottawa Scale (median score 8, interquartile range 7–9).
Results Increased maternal age (mean difference 0.62, 95% CI 0.11–1.13), obesity (relative risk 1.25, 95% CI 1.15–1.37), smoking (relative risk 1.35, 95% CI 1.04–1.75), black ethnicity (relative risk 1.62, 95% CI 1.52–1.73), multiparity (relative risk 1.31, 95% CI 1.01–1.68), depression/anxiety (relative risk 1.42, 95% CI 1.27–1.59), moderate–severe asthma (relative risk 3.44, 95% CI 2.03–5.83, versus mild) and severe asthma (relative risk 2.70, 95% CI 1.85–3.95, versus mild–moderate) were associated with an increased risk of asthma exacerbations during pregnancy.
Conclusions Future interventions aimed at reducing exacerbations in pregnancy could address the modifiable factors, such as smoking and depression/anxiety, and introduce more regular monitoring for those with nonmodifiable risk factors such as obesity and more severe asthma.
Abstract
Increased maternal age, obesity, smoking, higher parity and asthma severity are associated with the risk of maternal asthma exacerbations. Future studies need to investigate a “treatable traits” approach to the management of asthma during pregnancy. https://bit.ly/37TuL6A
Introduction
Asthma is the most common medical condition in pregnancy, affecting between 8% and 12% of pregnant women worldwide. Changes in asthma symptoms vary between women and are unpredictable [1–3]. Up to 45% of pregnant women with asthma have an asthma exacerbation requiring medical intervention during pregnancy [4–6]. Both uncontrolled asthma and asthma exacerbations have been associated with increased risk of several adverse perinatal outcomes [7–9]. Furthermore, exacerbations have been associated with poor offspring respiratory health, including asthma [8, 10, 11].
Several studies identified patient-related risk factors for asthma exacerbations during pregnancy, including maternal age [8, 12], smoking [7, 8, 13, 14] and obesity [14–16]. Other studies identified disease-related factors such as increasing asthma severity [4, 5, 14, 17, 18] and lung function [5]. However, risks vary between studies, some studies report no associations, and no previous synthesis of this literature has been conducted.
Given the association between asthma exacerbations in pregnancy and adverse perinatal and infant health outcomes, it is important to identify risk factors that may be modifiable, allowing early identification and additional monitoring of women. The aim of this systematic review and meta-analysis is to synthesise recent literature to determine risk factors for asthma exacerbations during pregnancy and to quantify associations between risk factors and exacerbations.
Methods
The review protocol was registered with the International Prospective Register Of Systematic Reviews (registration number CRD42020196190). The study was reported following the 2020 Preferred Reporting Items for Systematic Reviews and Meta-Analysis [19] and the Meta-Analysis of Observational Studies in Epidemiology guidelines [20].
Information sources and search strategy
The search was conducted in electronic MEDLINE, Embase, Cumulative Index to Nursing and Allied Health and Cochrane Clinical Trials Register databases. The search terms (asthma or wheeze) and (pregnan* or perinat* or obstet*) and (exacerb* or flare up or morbidit* or attack*) were used to identify all potential studies for inclusion. The search was limited to studies conducted from 2000 to 24 August 2021 and available as an English-language publication.
Study selection
Using Covidence systematic review software (www.covidence.org), two independent reviewers screened the abstracts of all identified studies and assessed the full texts of potential articles. Disagreements at either stage of study selection were resolved by consensus or referral to a third reviewer. Studies rejected at each stage of the review were recorded, along with the reasons for rejection at the full-text screening stage.
Eligibility
Prospective or retrospective cohort studies, case–control studies and randomised controlled trials (RCTs) were included. We included studies that contained data from pregnant women with physician-diagnosed asthma (whether confirmed or subject self-report) or database-coded asthma diagnosis.
Exposures included patient characteristics that may be risk factors/predictors of exacerbation, including demographic characteristics, asthma characteristics, other health-related characteristics or pregnancy characteristics.
The outcome was asthma exacerbations requiring medical intervention such as hospitalisations, emergency department visits, unscheduled physician visits or oral corticosteroid (OCS) courses for asthma during pregnancy.
Data extraction
Data from included studies was extracted and recorded in a standardised form including study population details, exacerbation definition and years and country of data collection. Data extraction was performed by one reviewer and checked by a second, with discrepancies resolved by discussion reaching consensus.
Risk of bias assessment
Included studies were independently assessed by two reviewers, using the Newcastle–Ottawa Scale [21] for observational studies and the Cochrane Risk of Bias tool [22] for RCTs. Quality scores were recorded with extracted data. GRADE (Grading of Recommendations, Assessment, Development and Evaluations) was used to determine certainty of the meta-analysis results [23].
Data synthesis and analysis
Narrative synthesis of the findings is structured around subject characteristics and distribution of potential predictors. Meta-analyses were conducted for risk factors reported by two or more studies with comparable exacerbation outcome definitions, using STATA 17.0 (StataCorp, College Station, TX, USA). A random-effects model was used for dichotomous outcomes to calculate relative risk (relative risk) with a 95% confidence interval when more than two studies were combined; alternatively, a fixed-effect model was used. For continuous outcomes, the mean difference was calculated between exacerbation groups. Forest plots were created for each meta-analysis.
Heterogeneity between studies was assessed using the I2 parameter (I2>60% indicates heterogeneity) and Chi-squared test (p<0.1 indicating significant heterogeneity). To investigate heterogeneity, subgroup analysis with random effects by active asthma management was performed for analyses with significant heterogeneity. Publication bias was explored with Egger's tests for analyses including ≥10 studies or more.
Results
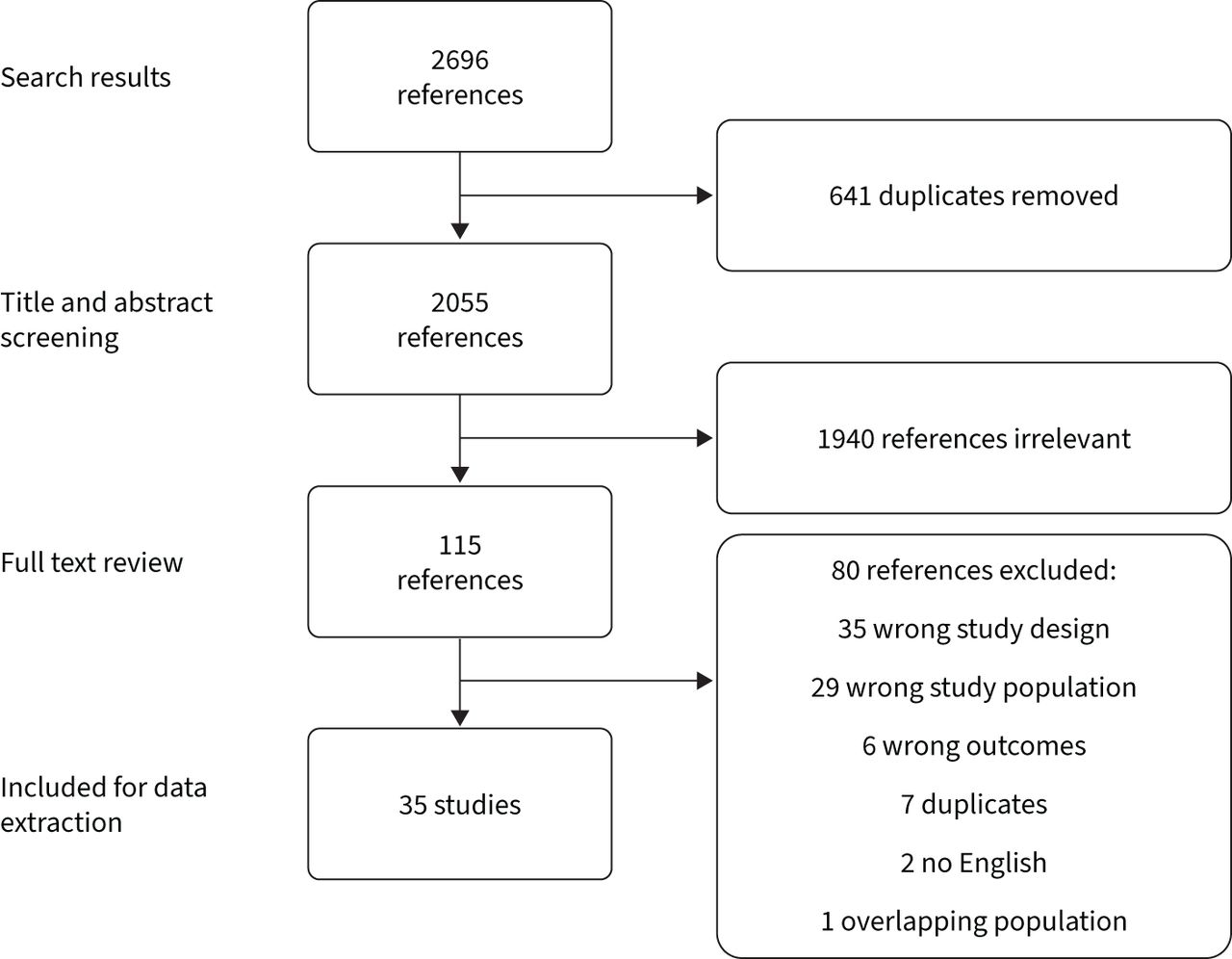
35 articles were included in the review (figure 1). In total, 429 583 pregnant women with asthma were included; the proportion of women with an exacerbation during pregnancy ranged from 2.5% [11] to 36.3% [4]. Studies were of good quality (median score 8, interquartile range (IQR) 7–9) (supplementary table S2). All meta-analyses are presented in supplementary table S3, and subgroup analyses in supplementary table S4.

Flow diagram of included studies.
Maternal factors
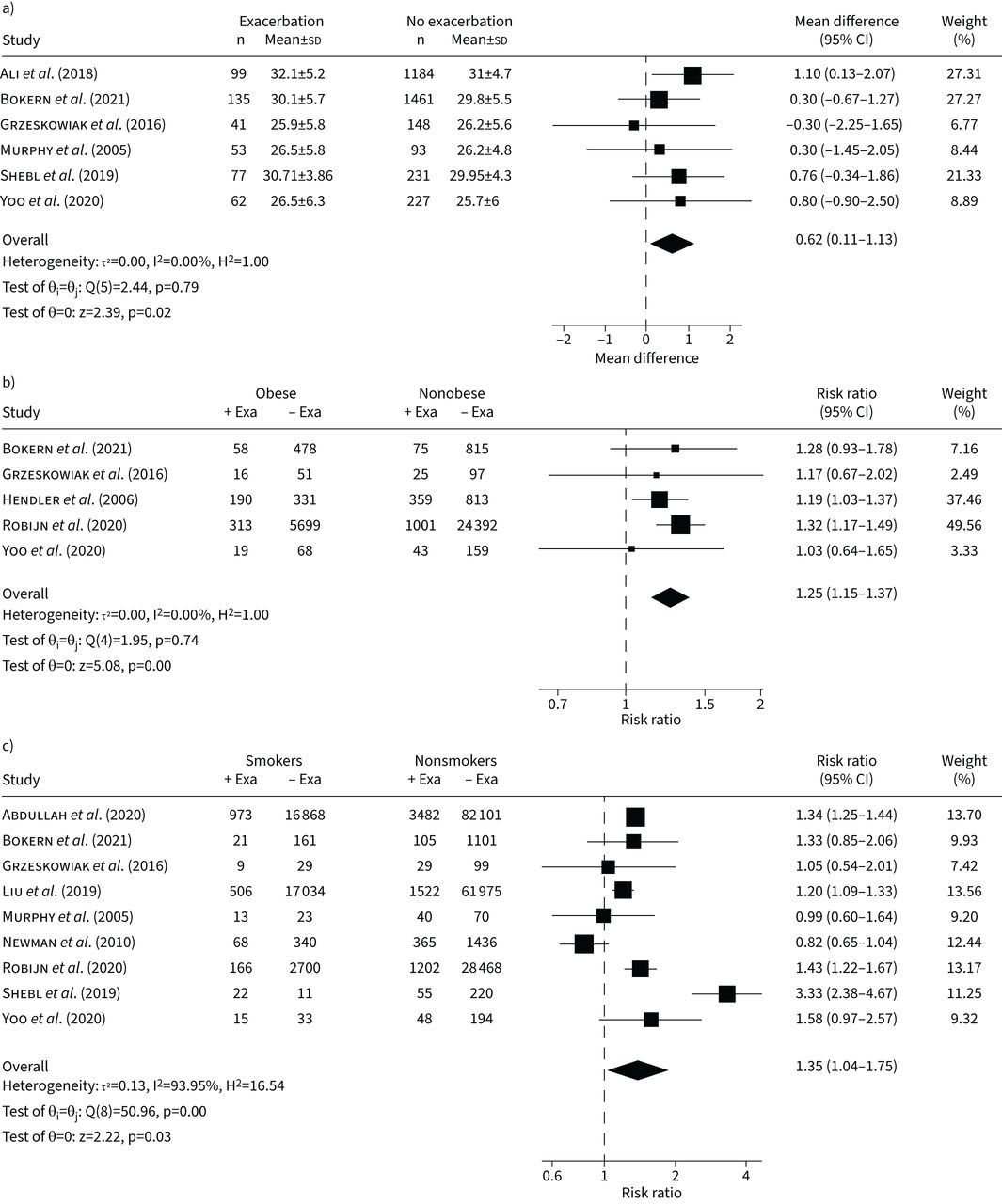
Maternal age was reported in nine studies [4, 8, 12, 14, 24–28]. Six studies [4, 12, 24–27] reporting mean±sd were combined in a meta-analysis finding exacerbations associated with higher age (mean difference 0.62 years, 95% CI 0.11–1.13 years; I2=0.0%) (figure 2a). Four studies reported age categories; one study [8] with a cut-off age of 34 years, and three [4, 14, 28] studies with a cut-off age of 35 years. Meta-analysis showed a 27% increased risk of exacerbation with maternal age ≥35 years (relative risk 1.27, 95% CI 1.06–1.52; I2=87.8%). Heterogeneity remained after subgroup analysis.

Forest plots of meta-analyses. a) Age, b) obesity and c) smoking status. Exa: exacerbation.
Maternal body mass index (BMI) was reported in nine studies [4, 12, 14, 16, 24–27, 29]. Two studies [4, 27] reported data as median (IQR) with no statistical difference between exacerbation status; three studies [12, 24, 25] were combined in a meta-analysis, showing no association between exacerbation status and BMI (mean difference 1.82 kg·m−2, 95% CI –1.12–4.75 kg·m−2; I2=95.2%). Five studies [12, 14, 16, 26, 27] reported BMI categories; meta-analysis showed a significant 25% increased risk of exacerbation in obese versus nonobese women (relative risk 1.25, 95% CI 1.15–1.37; I2=0.0%) (figure 2b). One study [29] reported decreased odds of exacerbation for women with a nonobese BMI compared to an obese BMI.
Maternal cigarette smoking was reported in 10 studies [4, 8, 12, 14, 25–30], of which nine [4, 8, 12, 14, 25–28, 30] were included in a meta-analysis, showing a 35% increased risk of exacerbation with current smoking versus nonsmoking (relative risk 1.35, 95% CI 1.04–1.75; I2=94.0%) (figure 2c). Heterogeneity remained in the active management subgroup.
Maternal ethnicity was reported in four studies [26, 27, 31, 32], two [26, 31] of which were combined in a meta-analysis, showing an increased risk of exacerbation in American women of black versus white ethnicity (relative risk 1.62, 95% CI 1.52–1.73; I2=94.0%). One study [32] also reported an increased risk of hospitalisation, emergency department visit and OCS use for women of black ethnicity. One Australian study reported no difference in exacerbations between women of white/European, Indigenous and other/unknown ethnicity [27]. One study [14] reported an increased risk of exacerbations among women born outside Europe versus those born within Europe.
Three studies [8, 25, 28] reported on rurality of maternal residence and were combined in a meta-analysis showing no difference in exacerbation risk for rural versus metropolitan/regional residence (relative risk 0.92, 95% CI 0.66–1.28; I2=95.2%). Heterogeneity remained after subgroup analysis.
Single studies found increased risks of exacerbations for women of low social class versus high class [28], women without a partner versus with a partner [28], women with at least three children in the household versus fewer than three children [28], women with ≤12 years versus ≥13 years of education [14] and women who were illiterate versus those with intermediate/high education [25].
One Canadian study [26] reported on insurance type (public or private), showing no difference in exacerbation risk. Greater proportions of women with an exacerbation during pregnancy were in the “most deprived” categories for material deprivation and residential instability quintiles from the Ontario Marginalization Index [8].
Maternal comorbidities were reported in seven studies [14, 25, 26, 28, 29, 33, 34]. Women with anxiety and/or depression were at significantly higher risk of exacerbation compared to women without anxiety and/or depression (relative risk 1.42, 95% CI 1.27–1.59; I2=68.7%) (two studies [14, 33]). One study [27] reported that women with higher risk scores on the Edinburgh Postnatal Depression Scale were at higher risk of exacerbations. Gastro-oesophageal reflux disease and allergic rhinitis were reported in two studies [25, 26] and were not associated with exacerbation risk (relative risk 0.98, 95% CI 0.61–1.58; I2=0.0% and relative risk 1.28, 95% CI 0.85–1.92; I2=89.5%, respectively). Low vitamin D [35], allergy [29] and atopy [25] were each reported in one study and none were associated with exacerbation risk during pregnancy.
Pregnancy factors
Women with exacerbations during pregnancy gained significantly less weight during pregnancy (mean difference −2.71 kg, 95% CI −4.48– −0.94 kg; I2=69.3%) (three studies [4, 12, 24]; figure 3a) compared to women without exacerbations. One study reported no difference in exacerbation risk between women who gained weight above recommendations versus below/within recommendations [15]. Fetal sex was not associated with exacerbation risk based on a meta-analysis of 10 studies [4, 8, 12, 24–28, 36, 37] (relative risk 1.05, 95% CI 0.89–1.25; I2=88.9%; male versus female, no publication bias p=0.91), and in one study by exacerbation type [38]. Heterogeneity remained in the active involvement subgroup. Six studies [4, 12, 14, 24, 27, 28] were included in a meta-analysis comparing showing a 31% increased risk of exacerbation for multiparous women versus nulliparous (relative risk 1.31, 95% CI 1.01–1.68; I2=89.1%) (figure 3b). Heterogeneity remained in the active involvement subgroup. Women carrying twins or triplets were at a more than two-fold increased risk of exacerbation compared to singleton pregnancies (relative risk 2.23, 95% CI 1.10–4.50; I2=68.9%) (three studies [24, 26, 27]; figure 3c). Heterogeneity did not remain in subgroup analysis.

Forest plots of meta-analyses. a) Gestational weight gain, b) parity and c) plurality. Exa: exacerbation.
Antenatal model of care (midwife/medical/shared care) was not associated with exacerbations [27].
Asthma factors
Six studies [4, 5, 25, 39–41] containing seven populations were included in meta-analyses showing that women with moderate/severe asthma, based on medication utilisation, were 3.4 times more likely to have an exacerbation compared to women with mild asthma (relative risk 3.44, 95% CI 2.03–5.83; I2=99.2%) (figure 4a). Women with severe asthma were 2.7 times more likely to have an exacerbation compared to moderate/mild asthma (relative risk 2.70, 95% CI 1.85–3.95; I2=98.5%). Heterogeneity remained in subgroup analysis.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plots of meta-analyses. a) Asthma severity, b) history of recent hospitalisation/emergency department visit for asthma and c) inhaled corticosteroid (ICS) use ∼18 weeks’ gestation. Exa: exacerbation; MS: MarketScan (private insurance); MAX: Medicaid Analytic Extract (public insurance).
History of pre-pregnancy exacerbations, including hospitalisation [27, 42] (relative risk 3.75, 95% CI 2.82–4.97; I2=39.0%) (figure 4b), emergency department visits [27, 42] (relative risk 3.80, 95% CI 2.94–4.90; I2=91.6%) (figure 4b), outpatient visits [42], OCS courses [27] and mechanical ventilation [26] were associated with an increased risk of exacerbations during pregnancy. No history of pre-pregnancy exacerbations (hospitalisation/emergency department visits/OCS courses) was associated with reduced risk of exacerbations during pregnancy (OR 0.22, 95% CI 0.14–0.35) [29].
Nine [12, 14, 26, 27, 29, 42–45] studies reported the use of inhaled corticosteroid (ICS). Two studies [12, 27] reported that women using ICS at study enrolment (∼18 weeks’ gestation) were 65% more likely to have an exacerbation later during pregnancy (relative risk 1.65, 95% CI 1.42–1.92; I2=0.0%) (figure 4c). One [29] study reported reduced odds for exacerbation among women without an ICS prescription in early pregnancy compared to those with ICS. One study reported that women using ICS with long-acting β-agonists (LABA) in mid-pregnancy were at increased risk of exacerbation [27]. One study reported no difference in exacerbations per month during pregnancy between treatment groups (no ICS, ICS mono-therapy, ICS/LABA therapy) [45]. Additionally, this study reported higher odds of exacerbation among those treated with ICS/LABA in mid-pregnancy compared to no ICS [45].
Two studies reported on medication dosage; one found significant odds for exacerbation with mid-pregnancy low–moderate doses versus no ICS and for high doses versus no ICS. One RCT reported no difference in risk of exacerbation among women treated with beclomethasone versus theophylline [44]. No difference was found between step-up in ICS dose versus step-down [46]
Four [4, 25, 27, 29] studies reported various spirometry measures. One study [29] reported reduced risk of future exacerbations in women with a forced expiratory volume in 1 s (FEV1)/forced vital capacity (FVC) ratio above the lower limit of normal (LLN) compared to a ratio below the LLN. In one study [27], decreased FEV1% predicted was associated with an increased risk of future exacerbations treated with OCS, while mean FVC% predicted also differed in women treated with OCS versus no OCS [27]. Other studies reported no differences in lung function by exacerbation status [4, 25, 27, 29].
Lung inflammation measured by fraction of exhaled nitric oxide (FeNO) was not associated with future exacerbations in one study [27], whereas another study reported a reduced risk of exacerbations for those with FeNO levels <25 ppb [29]. There was no difference between asthma subtypes [47].
Higher scores on the Asthma Quality of Life Questionnaire were associated with reduced risk of exacerbation [48], with similar estimates for the emotion and symptom subdomains [49]. Higher scores on the consequences, identity and emotional response domains from the illness perception questionnaire were associated with increased exacerbation risk during pregnancy [49], but no association with Pregnancy Asthma Control Test [50]. The same study [49] reported a reduced risk of exacerbations with lower scores on the Perceived Control of Asthma Questionnaire. Worse asthma control measured using the Asthma Control Questionnaire [27] or Global Initiative for Asthma (GINA) standards [27, 51] was associated with an increased risk of exacerbations. Clinically stable asthma (well controlled by GINA guidelines, FEV1 >80% predicted and FeNO <25 ppb) before 18 weeks’ gestation was associated with a reduced risk of exacerbations during the remainder of pregnancy [29].
Two studies reported antenatal asthma management strategies. A nurse-led programme versus standard care did not have a significant effect on reducing exacerbations [52], while an inflammation-based management versus a symptom-based management significantly reduced exacerbation risk during pregnancy [53].
One study reported higher prevalence of certain self-reported asthma triggers, such as reflux, work environment, pets, foods, aspirin and fumes, among pregnant women who experienced an exacerbation compared to those who did not exacerbate [27].
Asthma self-management skills such as correct medication knowledge and ICS nonadherence at ∼18 weeks’ gestation were not associated with future exacerbations, whereas good inhaler technique and possession of a written action plan were associated with an increased risk of exacerbations in one study [27].
Discussion
Main findings
This is the first systematic review and meta-analysis to synthesise the literature on risk factors for asthma exacerbations during pregnancy. The greatest increased risk of exacerbations requiring medical intervention was a 3.4-fold increased risk for women with moderate to severe asthma, compared to women with mild asthma. Women carrying twins/triplets were at a 2.2-fold risk for an exacerbation compared to women carrying singletons. Furthermore, there was a 62% increased risk for asthma exacerbations in pregnancy for women of black ethnicity, a 42% increased risk for women with depression and anxiety, a 35% increased risk for current smokers, a 31% increased risk for multiparous women, a 27% increased risk for women aged >35 years and a 25% increased risk for obese women.
Strengths and limitations
Although some of the factors presented in this review are already known, this study has several strengths: the systematic approach to reviewing the literature, the inclusion of meta-analyses and the use of GRADE, showing high certainty for many of the analyses. However, there were some limitations, including high heterogeneity between studies. The latter may have been related to the observational nature of the cohort studies reviewed, and the influence of potential confounding factors.
ICS use varies between countries [54] and may be associated with different prevalence of exacerbations. Unfortunately, we were only able to combine two Australian studies on ICS use at 18 weeks’ gestation to give a relative risk of ICS use or dose for asthma exacerbations in pregnancy. Individual studies showed that expectant mothers with lower education and those born outside Europe were at increased risk of having an asthma exacerbation. Further research is needed to determine whether these factors, and black ethnicity, are indicative of health literacy and whether that is the underlying risk factor. Health literacy has been reported to affect long-term asthma outcomes and exacerbations [55]. Others may also have underlying risk factors; indicators such as pre-pregnancy exacerbations, ICS or ICS/LABA use, good inhaler technique and possession of a written action plan may be associated with moderate–severe asthma.
Interpretation
Several of the risk factors for exacerbation identified in this review are also risk factors for adverse perinatal outcomes, in general, and specifically for women with asthma. Cigarette smoking is known to contribute to low birthweight [56] and preterm birth [57], adverse outcomes that are more common among women with asthma [58], and specifically those who exacerbate during pregnancy [9, 59]. Among adults with asthma, smoking reduces response to treatment with corticosteroids [60–62]. Therefore, smoking cessation is recommended for all people with asthma who smoke, as achieving good asthma control is more difficult among smokers. For women of childbearing age smoking cessation prior to pregnancy may improve asthma control, increase responsiveness to treatment and improve perinatal and infant outcomes [56, 57, 63, 64].
We showed previously that maternal overweight and obesity, but not excess gestational weight gain [65], was associated with exacerbations of asthma in pregnancy, and driven by macrophage activation, measured as elevated serum soluble CD163 [15]. Among adults with asthma, obesity reduces response to ICS treatment, limiting asthma control [66]. The results of this review support recommendations to lose weight prior to pregnancy for women with asthma with overweight and obese BMI. Weight loss may reduce exacerbation risk, and the risk of adverse perinatal outcomes [67, 68].
The prevalence of depression and other mental illnesses is common among pregnant women with asthma [33, 69]. Adults with asthma and depression/anxiety have higher rates of other risk factors for asthma exacerbations, such as smoking, obesity and increasing asthma severity, compared to adults with asthma without depression/anxiety [70]. It is unknown whether the biological changes associated with mental illness increase the risk of exacerbation or whether the risk of exacerbations can be mitigated by treatment, both pharmaceutical and nonpharmaceutical.
Healthcare professionals caring for women with asthma who are pregnant or planning a pregnancy could use the risk factors from this review to identify women at particular risk of exacerbation. For women planning a pregnancy, modifiable risk factors such as obesity and smoking should be addressed as early as possible to mitigate the risk of exacerbations. These data support the development of a “treatable traits” approach to asthma management during pregnancy, which in addition to pulmonary traits (such as airway inflammation and symptoms), addresses extrapulmonary traits such as depression/anxiety and behavioural traits such as smoking. In the context of severe asthma, traits such as being prone to exacerbations, depression and vocal cord dysfunction, were associated with future exacerbation risk [71, 72], and a trial of a treatable traits approach improved both asthma control and health-related quality of life [73].
In conclusion, this systematic review and meta-analysis has corroborated an increased asthma exacerbation risk in pregnancy in association with moderate and severe asthma, maternal age, obesity, smoking, black ethnicity, depression and anxiety and parity. Future interventions aimed at reducing exacerbations in pregnancy could address modifiable factors and introduce more regular monitoring for those with nonmodifiable risk factors.
Supplementary material
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Search strategy ERR-0039-2022.SUPPLEMENT1
Supplementary tables ERR-0039-2022.SUPPLEMENT2
Footnotes
Provenance: Submitted article, peer reviewed.
Author contributions: A.L. Robijn: study selection, data extraction, data analysis, interpretation of results, writing of manuscript. M.P. Bokern: protocol development, study selection, data extraction. M.E. Jensen: study conception, development search strategy. D. Barker: protocol development, statistical advisor. K.J. Baines: protocol development. V.E. Murphy: study conception, development search strategy, interpretation of results, manuscript writing. All authors read and approved the final manuscript.
Conflict of interest: M.P. Bokern reports support for the present manuscript from Groningen Research Institute of Pharmacy, PharmacoTherapy, Epidemiology and Economics, University of Groningen, Groningen, the Netherlands and Department of Non-Communicable Disease Epidemiology, London School of Hygiene and Tropical Medicine, London, UK. M.P. Bokern reports grants or contracts from GlaxoSmithKline (GSK PhD scholarship at London School of Hygiene and Tropical Medicine), outside the submitted work. V.E. Murphy reports support for the present manuscript from Medical Research Future Fund Investigator Grant (paid to her institution). The remaining authors have nothing to disclose.
Support statement: M.E. Jensen is supported by a Peggy Lang Hunter Children's Research Foundation Early Career Fellowship. K.J. Baines is funded by an Australian Lung Foundation COPD Research Fellowship and received funding from NHMRC (APP1104645 and APP1144941), and the John Hunter Charitable Trust. V.E. Murphy received a Career Development Fellowship from the NHMRC (grant no. APP1084816), the Gladys M. Brawn Memorial Career Development Fellowship from the University of Newcastle and the Medical Research Futures Fund Investigator Grant (application ID 1196252). The authors alone are responsible for the content of this manuscript. No funding was received for the study.
- Received February 22, 2022.
- Accepted April 7, 2022.
- Copyright ©The authors 2022
This version is distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0. For commercial reproduction rights and permissions contact permissions{at}ersnet.org
References










