





Figures
- FIGURE 1
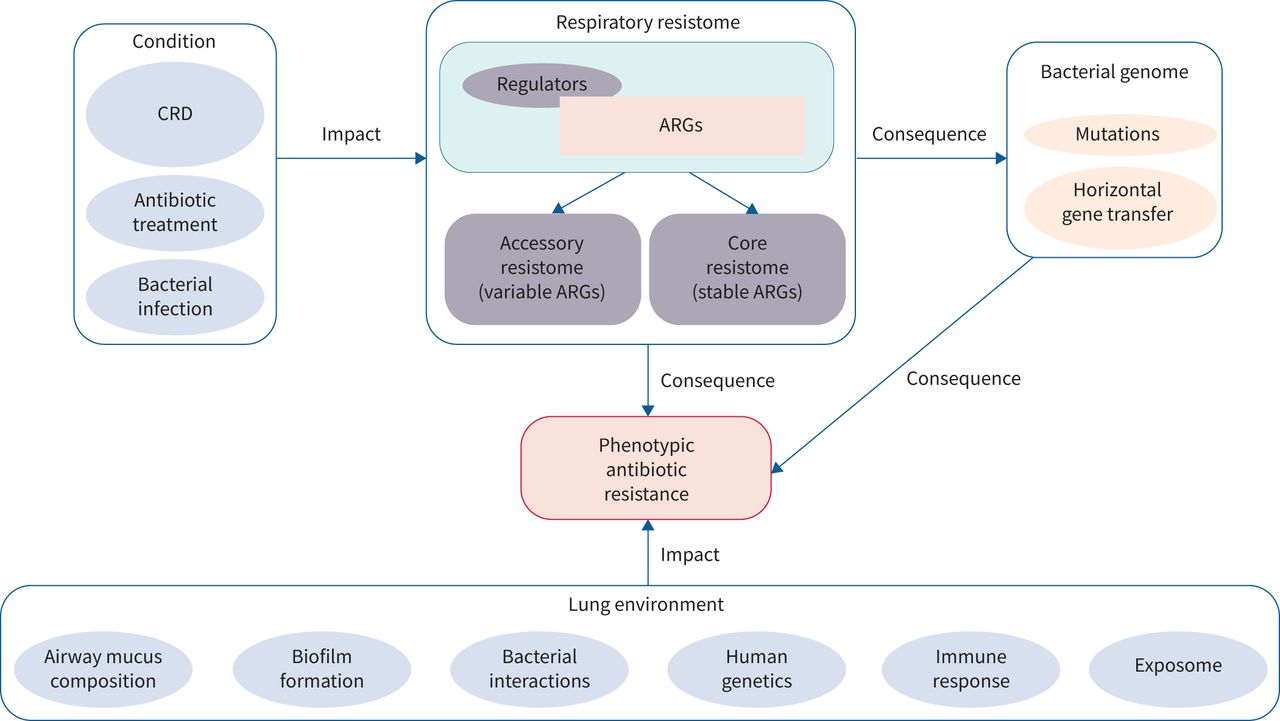
The respiratory resistome and its partners. The respiratory resistome is defined as the total of the antibiotic-resistance genes (ARGs) present in pathogenic and non-pathogenic bacteria in the respiratory airways. These ARGs can undergo mutations and spreading by horizontal gene transfer. A “core” resistome has been defined based on the similarity of ARGs found in healthy subjects and people with chronic respiratory disease (CRD). The “accessory” resistome refers to the resistome specific to CRD patients, and is affected by different factors, e.g. CRD pathophysiology, bacterial infection and antibiotic treatment. The resistome has an impact on the phenotypic antibiotic bacterial resistance, which is also affected by lung environment factors such as airway mucus composition, biofilm formation, bacterial interactions, human genetics and the immune response.
- FIGURE 2
Advantages, challenges and issues of resistome analysis in chronic respiratory diseases. Resistome data interpretation for the implementation of antibiotic resistance prediction relies on different strategies. A scoring system, based on analysis of mutations and horizontally acquired antibiotic-resistance genes (ARGs), has been developed [81]. Another method uses machine-learning strategies to predict phenotypic resistance by combining sequencing and transcriptome analysis [82]. Three-dimensional modelling, by building structural models, can also help in protein function prediction [64]. Functional metagenomics, which correlates phenotypic resistance and metagenomics data, can also provide insight into the interpretation of bacterial resistance [60]. However, some issues need to be settled. The variation in respiratory resistome data depending on the methodology used complicates inter-study comparison [83, 84]. Also, some variation in ARG abundance and resistome data can be associated with the intrinsic resistance of a single bacterial taxa, and needs to be correlated with microbiome analysis [53]. Finally, some difficulties can emerge in the phenotypic prediction of resistance to antibiotic molecules. SOP: standard operating procedure.


{kind=link}
{kind=link}
Tables
- TABLE 1
Summary of antibiotic treatments recommended in CRDs
Type of CRD Indication Cystic fibrosis COPD Severe asthma Bronchiectasis Bacterial prophylaxis Staphylococcus aureus
UK: flucloxacillin the first 3 years of life [15, 16]
Other countries: not recommended (uncertainty on clinical consequences and on P. aeruginosa colonisation [17])NA NA NA Bacterial eradication Pseudomonas aeruginosa
First-line treatment: 28 days of TIS or up to 3 months of a combination of nebulised colistin and oral ciprofloxacin [16]
Aggressive therapy: i.v. meropenem or i.v. tobramycin [15]
MRSA
Combined oral and i.v. antibiotic regimen (fusidic acid, rifampicin, teicoplanin and vancomycin) [15]NA NA P. aeruginosa
First-line treatment: 14 days of oral ciprofloxacin
If persistence of positive culture of sputum samples: i.v. treatment (e.g. β-lactam+aminoglycoside) or inhaled antibiotics (e.g. colistin, tobramycin or gentamicin) with a total duration of 3 months [18, 19]Chronic suppressive therapy P. aeruginosa
Intermittent therapy: treatment with TIS for 28 days (300 mg twice daily) on alternate months (28-day on/off)
Alternatives: TIP, inhaled aztreonam lysine, colistimethate dry powder or LIS [16, 20–22]
Continuous daily administration mode also increasingly recommended [23]
Maintenance therapy
Proposition of 6 months of oral azithromycin with a 3 times a week dose of 500 mg [27]Key pathogens
Antibiotic courses administered 3 times per week [24]
Maintenance therapies
Infra-dose of azithromycin [25]Maintenance therapy
Oral infra-dose of azithromycin for 48 weeks
Azithromycin 3 times per week orally, in addition to inhaled corticosteroids and long-acting bronchodilators [7]Recurrent (≥3 per year) or severe acute PEx [19, 26]
Long-term inhaled antibiotics (nebulised gentamicin, TIS, colistimethate dry powder, dry powder or liposomal ciprofloxacin), usually prescribed on alternate months [18]
Long-term oral treatment with macrolide or other molecules [18, 26]Treatment of PEx P. aeruginosa-induced PEx
4 days with i.v. administration route [16]; oral or inhaled administration route can also be used [15, 23]
Other bacterial species-related PEx
≥2 antibiotics with different mechanisms of actions [16]Antibiotic therapy: not systemically recommended [25, 28]
Duration of antibiotic treatment: 5–10 days [28]Antibiotic therapy: not systemically recommended except in cases of documented pneumopathy [29] Antibiotic therapy: 14 days of antibiotics are recommended
First-line: oral antibiotics
In case of severity: i.v. ± inhaled colistimethate dry powder [18, 19, 26]CRD: chronic respiratory disease; COPD: chronic obstructive pulmonary disease; PEx: pulmonary exacerbations; NA: not applicable; TIS: tobramycin solution for inhalation; i.v.: intravenous; MRSA: methicillin-resistant Staphylococcus aureus; TIP: tobramycin inhaled powder; LIS: levofloxacin inhaled solution.
- TABLE 2
Impact of antibiotics on the respiratory microbiome in CRDs
Antibiotic Sample analysed Type of treatment Impact of antibiotics on diversity of the microbiome Impact on relative abundance of bacterial taxa Disease Reference Association of different antibiotic class in treatment of CF exacerbation episodes Sputum Diverse antibiotic treatments for a course of 8–9 years ↓ α-diversity (inverse Simpson index) – CF [30] Sputum Diverse antibiotics used for the treatment of acute PEx ↑ Species richness through PEx and treatment periods, but return to the baseline state during recovery period ↓ Prevotella melaninogenica and Streptococcus sanguinis
↑ Veillonella parvula during treatment period, but return to baseline state in post-recovery samplesCF [31] Sputum Diverse antibiotics used for the treatment of acute PEx Either very little change through exacerbation cycle or return to baseline state on the post-recovery sample No taxa modification associated with clinical stage, including treatment CF [32] Oral macrolides Oropharyngeal swab 12 months of twice daily oral doses of 400 mg of erythromycin No impact on α-diversity measures Difference between treated and placebo groups:
↓ Actinomyces and Streptococcus
↑ Haemophilus after 48 weeks of treatmentBE [33] Oropharyngeal swab 6 months of 250 mg daily azithromycin for 5 days and then 250 mg 3 times per week Impact on β-diversity measures ↓ Fusobacteria
↑ Firmicutes during treatment compared with untreated group, but return to pre-treatment state after a 1-month washout periodSevere asthma [34] Sputum 12 months of low-dose azithromycin ↓ Faith's phylogenetic diversity ↓ Gammaproteobacteria (including H. influenzae) after 48 weeks of azithromycin treatment compared with placebo group Severe asthma [35] Bronchoalveolar lavage of the right upper lung lobe 6 weeks of low-dose azithromycin ↓ Shannon's diversity index ↓ Prevotella, Staphylococcus and Haemophilus
↑ Anaerococcus between pre- and post-treatment stateModerate and severe asthma [36] Sputum Low-dose erythromycin Increase of genus richness between baseline and 48 weeks in treated group but no difference with placebo group No change in composition of airway microbiome in P. aeruginosa-dominated subgroup
↓ H. influenzae and ↑ P. aeruginosa in non-P. aeruginosa-dominated subgroupBE [37] Sputum Treatment of exacerbations exclusively by antibiotics (without addition of corticosteroids) (two treatments azithromycin, one by ofloxacin, one by trimethoprim-sulfamethoxazole) – ↓ of multiple taxa, mainly Proteobacteria COPD [38] β-lactams Nasal swabs Various courses of treatments of several weeks, mostly (71%) β-lactams ↑ Shannon's diversity index ↓ Moraxellaceae
↑ other bacterial families (this increase was verified after more than one antibiotic treatment)CF [39] Bronchoalveolar lavage, sputum or deep throat swabs Courses of treatment including β-lactams (25 of 31 involving a single β-lactam molecule) for acute PEx ↓ α-diversity between exacerbation and treatment
↓ α-diversity at therapeutic doses between baseline and treatment
↑ α-diversity at sub-therapeutic doses at the same time points↓ Haemophilus, Clostridiales and Lachnospiraceae
↑ Fusobacterium and Pseudomonas in the group treated at therapeutic doses between baseline and treatment samples
No difference was observed in the sub-therapeutic group at the same time points
No difference in the bacterial composition was observed in the two groups between post-recovery and baseline samples, or between exacerbation and treatment samplesCF [40] Sputum Treatment of exacerbation episodes, 19 of 23 treatments including β-lactams Minimal impact on global community structure ↓ RA of some low abundance taxa with antibiotic treatment: Gemella, two Pasteurella OTUs, two Streptococcus OTUs, Oribacterium and Neisseria CF [41] Sputum Treatment of exacerbation episodes by associations including at least one i.v. β-lactam ↑ Shannon's diversity index in the first 72 h of treatment
Return to the baseline state after 8–10 days of treatment↓ P. aeruginosa
↑ anaerobes (Prevotella and Veillonella), in the first 72 h of treatment but return to the baseline state after 8–10 days of treatmentCF [42] Sputum Cycle of 28 days of AZLI treatment followed by a 28-day period without treatment No significant change in Shannon's diversity index or Bray-Curtis β-diversity index in one AZLI cycle
↓ Shannon's diversity index
↓ Bray–Curtis β-diversity with ↑ AZLI cycles– CF [43] Aminoglycosides Sputum A 1-month treatment with TIP ↓ average species richness (Shannon and Simpson diversity indices) after 1 week of therapy
Return to baseline state after the end of TIP therapyMost changes noticed between baseline state and first week of treatment occurring among low abundance taxa, mostly facultative and obligate anaerobes (Neisseria, Megasphaera, Granulicatella, Haemophilus, Streptococcus, Gemella, Rothia, Veillonella, Oribacterium) CF [44] Sputum TIP or TIS during at least 1 year No difference in Shannon's diversity index ↓ Parvimonas CF [45] CRD: chronic respiratory disease; CF: cystic fibrosis; PEx: pulmonary exacerbation; BE: bronchiectasis; COPD: chronic obstructive pulmonary disease; RA: relative abundance; OTU: operational taxonomic unit; i.v.: intravenous; AZLI: aztreonam lysine for inhalation; TIP: tobramycin inhaled powder; TIS: tobramycin inhaled solution.
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Supplementary material ERR-0259-2021.SUPPLEMENT










