





Abstract
Excessive daytime sleepiness (EDS) is a major symptom of obstructive sleep apnoea (OSA), defined as the inability to stay awake during the day. Its clinical descriptors remain elusive, and the pathogenesis is complex, with disorders such as insufficient sleep and depression commonly associated. Subjective EDS can be evaluated using the Epworth Sleepiness Scale, in which the patient reports the probability of dozing in certain situations; however, its reliability has been challenged. Objective tests such as the multiple sleep latency test or the maintenance of wakefulness test are not commonly used in patients with OSA, since they require nocturnal polysomnography, daytime testing and are expensive. Drugs for EDS are available in the United States but were discontinued in Europe some time ago. For European respiratory physicians, treatment of EDS with medication is new and they may lack experience in pharmacological treatment of EDS, while novel wake-promoting drugs have been recently developed and approved for clinical use in OSA patients in the USA and Europe. This review will discuss 1) the potential prognostic significance of EDS in OSA patients at diagnosis, 2) the prevalence and predictors of residual EDS in treated OSA patients, and 3) the evolution of therapy for EDS specifically for Europe.
Abstract
Drugs for EDS are available in the USA but were discontinued in Europe some time ago. For European sleep doctors, treatment of EDS with medication is new, while novel wake-promoting drugs have been developed and approved for clinical use in OSA patients. https://bit.ly/3u9y3Ln
Introduction
Patients often seek medical advice for excessive daytime sleepiness (EDS), which is a major symptom of obstructive sleep apnoea (OSA) [1]. Sleepiness is defined as the inability to stay awake during the day, but its clinical descriptors remain elusive in both central disorders of hypersomnolence, such as narcolepsy or idiopathic hypersomnia [2] and in OSA [3, 4]. Moreover, the pathogenesis of EDS is complex and sleep disorders are not the only cause of EDS. Insufficient sleep, diseases such as diabetes, hypothyroidism or depression, and habitual use of some medications like hypnotics are amongst the most common. Patients’ symptoms may improve with OSA therapy such as continuous positive airway pressure (CPAP), but a proportion will remain sleepy [5].
Clinical evaluation of EDS can be performed by using subjective and objective tests [6]. The latter include the multiple sleep latency test (MSLT) and the maintenance of wakefulness test (MWT), which measure the propensity to fall asleep and the ability to stay awake, respectively. In patients with OSA, they are not commonly used, since they require full nocturnal polysomnography, additional daytime testing and are expensive. Subjective EDS can be evaluated by using the Epworth Sleepiness Scale (ESS), in which the patient reports the probability of dozing off in eight different situations [7]. A score ≥11 is considered as positive for EDS, and ≥16 indicates severe sleepiness. The reliability and repeatability of the ESS have been recently challenged [8–10].
Some drugs used to treat EDS despite CPAP, so-called residual EDS or residual sleepiness (RES), have been available in the United States but were discontinued in Europe about 10 years ago. Therefore, for many European respiratory physicians, treatment of RES with medication represents a new scenario, since they may lack experience in pharmacologic treatment of EDS, while new wake-promoting drugs have been recently developed and approved for clinical use in OSA patients in United States and Europe. In this review, we describe why sleepiness at diagnosis may have prognostic implications, how common RES is in our OSA population and how pharmacological therapy has evolved especially in recent times. We will focus on the European perspective, but the interested reader is referred to other recent reviews published from the USA [11, 12].
EDS at diagnosis: a risk factor for poor outcome in OSA
EDS is – together with snoring, male gender and obesity – the most prominent clinical sign of OSA. Up to 50% of the patients at diagnosis present with alternative symptoms, such as insomnia and disturbed sleep [13]. However, EDS is clinically most relevant as it affects quality of life and performance in private, social, and professional activities, and increases the risk of accidents whilst driving or at work [14, 15]. Several studies addressed the question if EDS independently predicts morbidity and mortality in OSA patients, as summarised in table 1.
Studies investigating the association between excessive daytime sleepiness (EDS) and mortality and morbidity
Empana et al. [16] performed a population-based multicentre prospective study in France in subjects aged ≥65 years followed over 6 years. The majority of them reported EDS and nocturnal sleep complaints, with a prevalence of EDS during follow-up of 18.7%. This was associated with an increased risk of mortality (1.33, 95% CI 1.13–1.61) after full adjustment for risk factors.
Other studies reported that only OSA with EDS was associated with increased risk [17], whereas neither sleep-disordered breathing nor EDS alone increased all-cause mortality. In a longitudinal study in 289 patients aged >65 years without clinical signs of dementia or depression followed for 13.8 years, moderate to severe OSA (apnoea/hyponoea index (AHI) ≥20 events·h−1) with EDS was associated with a 2.3 hazard ratio (HR) of mortality (95% CI 1.5–3.6) [18].
Similarly, in a prospective study in 2320 community-dwelling elderly (mean age: 73.6 years; follow-up: 9.9 years), the sample was divided into four groups based on snoring and EDS. The HR for incident cardiovascular events was significantly increased only in patients with snoring and EDS (1.46 (95% CI 1.03–2.08)) after adjusting for demographic and clinical confounding factors [19].
EDS may also predict cardiovascular events. In 104 patients with myocardial infarction followed for 48 months and studied by ESS and polysomnography, an ESS score ≥11 was associated with a higher risk for major cardiac events and re-infarction compared to the no EDS group (HR 2.15 (95% CI 1.08–4.18)). If EDS was associated with moderate to severe sleep-disordered breathing, the HR was 3.17 (95% CI 1.22–7.76) after adjustment for age and nadir oxygen saturation [20].
Most studies on the impact of EDS on survival focus on cardiovascular mortality. In the Cardiovascular Health Study (n=5888), EDS was the only symptom associated with mortality, incident cardiovascular morbidity, myocardial infarction and chronic heart failure (HF). After adjustment for age, the HR for mortality was 1.82 for men and 1.29 for women [21].
More recently, Mazzotti et al. [17] analysed OSA patients from the Sleep Heart Health Study to characterise phenotypes and assess their association with cardiovascular disease. The clinical phenotype with EDS showed a threefold higher risk of prevalent HF compared with the other phenotypes. In addition, both excessive and moderate EDS at diagnosis predicted an increased risk for incident cardiovascular disease, coronary heart disease and HF. Similar findings have been recently reported in Hispanic OSA patients [22].
Finally, some reports underlined the association of EDS and stroke, suggesting that daytime sleepiness is an independent risk factor for stroke and other cardiovascular events [23].
Although the majority of investigations reported increased cardiovascular mortality in patients with EDS, there are also negative results. In patients with systolic HF and AHI ≥15 events·h−1 at polysomnography, 5-year mortality was significantly higher in patients with ESS <6 as compared to those with an ESS ≥6 in a fully adjusted model [24]. In 3874 participants of the Sleep Heart Health Study with an AHI ≥15 events·h−1 and an ESS score ≥11 without prevalent cardiovascular disease at baseline, no significant association was found between EDS and risk of cardiovascular disease [25].
There are limited and controversial data on the possible pathogenetic mechanisms underlying the association between mortality and EDS. Lee at al. [26] performed a prospective cohort study to assess associations between coronary plaque phenotype, cardiovascular events and EDS. They measured blood lipid parameters and intravascular ultrasound for plaque evaluation in 170 patients undergoing coronary angiography. Patients with an ESS >10 had significantly higher total cholesterol and low-density-lipoprotein cholesterol. The coronary stenoses were longer and the cumulative incidence of adverse cardiovascular events during the 16-month follow-up was higher in the sleepier group. After adjustments for age and smoking habits, the HR for adverse cardiovascular events in the sleepier group was 3.44 (95% CI 1.01–11.72).
Considering other risk factors, Pak et al. [27] analysed the association between subjective sleepiness on the one hand and increased plasma tumour-necrosis-factor-related protein-1 (C1qTNF1), adipokines and 24 h ambulatory blood pressure on the other. C1qTNF1 was significantly higher in sleepy patients compared to those with an ESS <10. The 24 h blood pressure was significantly higher in sleepy participants as compared to nonsleepy participants.
The sympathetic nervous system plays a role in alertness, and both HF and OSA increase sympathetic nerve activity. In OSA patients with HF, an inverse relationship was found between muscle sympathetic nerve activity (MSNA) and ESS, but not with AHI, arousal index or oxygen saturation [28].
In summary, EDS is a major symptom of OSA but does not occur in all patients. Despite some conflicting findings, the majority of population-based data imply that EDS may be a marker of poor outcome, since it appears independently associated with cardiovascular morbidity and mortality. The prognostic role of persistent EDS in OSA during CPAP treatment has not been explored to date.
EDS in treated OSA patients
The most common treatment of OSA is the application of CPAP during sleep. CPAP splints the airway open and prevents occurrence of obstructive respiratory events. CPAP improves daytime sleepiness more effectively than placebo [29, 30]. A recent meta-analysis on the results of randomised control trials documented a significant reduction in subjective sleepiness, i.e. the ESS score, post-CPAP, whereas among objective tests changes were significant for the MWT but not for the MSLT [31]. A change in the ESS score of 2 points was considered as clinically significant, in agreement with the estimate of −2 to −3 points as the minimum clinically important difference in ESS score in treated OSA patients [32, 33].
A recent review [34] describes the complex relationship between OSA, cardiovascular risk and CPAP therapy in patients with or without EDS. It is noted that patients with severe EDS and OSA have a greater reduction in blood pressure and cardiovascular risk with CPAP than patients without EDS. This is important to bear in mind when thinking about additional treatments.
Some patients fail to improve their sleepiness after CPAP, with multiple factors possibly involved. In order to evaluate the cause and impact of the sleepiness for the patient a full sleep history by a sleep specialist must be taken (if not already available) rather than merely relying on the ESS. The history should also ask about the intensity and frequency of the sleepiness over a week as the ESS is known to vary considerably intraday and over time [35]. In addition, care should be taken when interpreting the ESS score as a patient may under or overestimate their sleepiness and have substantial misperception of effective sleepiness [36].
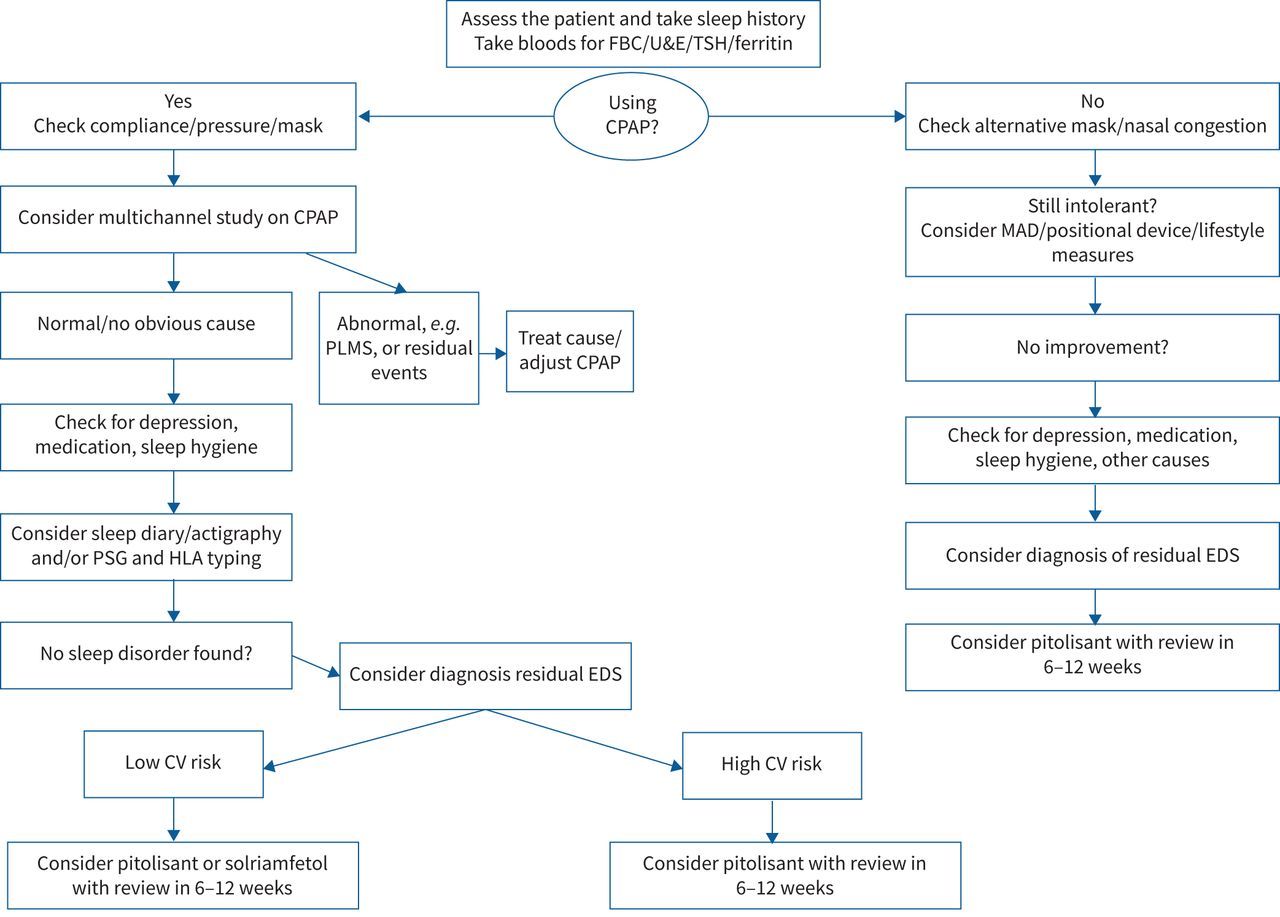
A step-wise approach should then be taken (see figure 1 for a guide).

{kind=link}
How to manage excess daytime sleepiness (EDS) in a specialist sleep clinic. CPAP: continuous positive airway pressure; CV: cardiovascular; FBC: full blood count; HLA: human leukocyte antigen; MAD: mandibular advancement device; PLMS: periodic limb movements of sleep; PSG: polysomnography; TSH: thyroid-stimulating hormone; U&E: urea and electrolytes.
First, CPAP-related problems may occur and should be carefully investigated. Suboptimal therapeutic pressure, poor mask fitting, or air leaks from the mask are common causes of persistent respiratory events, sleep fragmentation, and sleepiness during treatment. A recent meta-analysis pointed out that use of an oronasal mask was associated with incomplete resolution of OSA and poorer adherence compared to the use of a nasal mask [37]. When automatic positive airway pressure (APAP) is used, the pressure level varies according to sleep stages and position leading to the occurrence of arousals which may disturb sleep [38]. CPAP or APAP machines provide data on residual AHI and adherence to treatment. A high level of suspicion and additional diagnostic tests during positive airway pressure (PAP) treatment have been recommended in patients with persistently elevated AHI on treatment [39, 40] since the reliability of event identification by the PAP device algorithm may be far from optimal [41, 42]. PAP treatment may also be associated with treatment-emergent central sleep apnoea, especially in the first period of use [43], which resolves spontaneously over time in most cases [44]. Finally, poor adherence to PAP treatment, i.e. average nightly use for less than 4 h·night−1 over at least 70% of the nights, can be responsible for persistence of OSA symptoms including EDS.
When CPAP-related factors are ruled out, other possible causes of persistent EDS should be assessed. The most common cause of EDS in the general population is insufficient sleep duration, which should always be excluded, possibly by objective measurements such as actigraphy. The age of the patient, particularly for those over 75, should be taken into account and has been linked to daytime sleepiness [45] probably reflecting the increasing burden of comorbidities. A further expansion of the effect of this demographic is described in a recent review by Zinchuk and Yaggi [46], which showed that not only do older patients become more sleepy, but the older patients with most comorbidities obtain the least improvement with CPAP therapy.
Depression is another common cause of EDS, either directly or through the effects of psychotropic drugs, and is often associated with OSA [47]. Comorbid sleep disorders, such as the occurrence of restless leg syndrome, periodic leg movements (PLMs), or more rarely narcolepsy or idiopathic hypersomnia, or neurologic diseases associated with EDS, should also be investigated, especially when RES is severe despite optimal treatment for OSA. A full history of ongoing medical treatment may uncover the use of drugs causing sleepiness, i.e. hypnotics. Finally, medical conditions such as metabolic disorders (diabetes, obesity, hypothyroidism, among others) can be associated with EDS independent of OSA, through a state of low-grade inflammation. It is known that obesity is a potential cause of EDS, even in the absence of OSA [48, 49]. The role of obesity in the pathogenesis of EDS is supported by its improvement/resolution after weight loss [50], independent of changes in AHI [51].
Table 2 summarises the available studies on RES in CPAP-treated OSA patients. A study assessing EDS in treated OSA patients and in subjects from the general population reported a similar prevalence of EDS in both groups (with a bell-shaped curve of ESS), but the potential causes of EDS were not investigated and the groups were not well matched for sex or body mass index [52]. One multicentre randomised controlled trial assessed EDS monthly for the first 3 months of CPAP use, and showed a progressive decrease in its prevalence from 60% to 17%, together with significant sleep disruption during CPAP treatment documented by actigraphy [53]. The majority of studies were observational, either multicentre [5, 54–57] or single-centre [47, 53, 58–60]. These studies reported a variable prevalence of EDS in treated OSA patients, and follow-up duration varied from 3 to 24 months. All studies took into account the average nightly use of CPAP, since a clear relationship has been shown between adherence to treatment and decrease in ESS [5]. Similarly, the possibility of incomplete resolution of OSA was ruled out as a cause of RES, and a study underlined the high sensitivity of methods based on pulse arterial tonometry compared to traditional polygraphy in patients with residual EDS [61]. On average, prevalence of EDS was high in the first months of treatment, and declined thereafter. Results in patients using mandibular advancement devices were similar to those in patients using CPAP [60]. Studies agree that a high ESS at baseline increases the risk of remaining sleepy on CPAP treatment [47, 54, 57, 60, 62]. As for the impact of OSA severity assessed as AHI, mild-moderate rather than severe OSA was more often associated with RES [47, 56, 57]. One study investigated the possible role of PLMs in patients with RES, and reported a quite high prevalence of PLMs (38.5%) but no association with EDS [58]. Some studies investigated the role of depression [47, 54, 63], which is a major determinant of sleepiness in the general population. In addition, in most cases evaluation of EDS was based on subjective reports, rather than on objectively documented sleepiness. Vernet et al. [63] extensively studied 20 patients with RES and good adherence to CPAP after at least 6 months of treatment but RES in well-treated OSA patients was hard to explain. Moreover, the criteria defining central hypersomnia occurred only in 15% of the patients, and EDS responded poorly to wake-promoting drugs like modafinil. The accompanying editorial highlighted the lack of clinical descriptors of RES and suggested it might reflect an individually altered sensation, similar to what happens in subjects with a heightened perception of pain [3].
Summary of studies on residual sleepiness (RES) after obstructive sleep apnoea (OSA) treatment
Some studies used both subjective and objective tests for EDS. In the study by Budhiraja et al. [62], there was a good agreement between the prevalence of ESS >10 and of sleep latency at MWT <17 min (22.3% versus 23%). A recent study in 29 patients with RES (average ESS 16.3±2.3) and good adherence to CPAP (about 7 h·night−1) reported that 66% of the patients showed moderate-severe EDS assessed as sleep onset between <8–11 min, but no relationship was found between sleep latency and ESS [64].
Finally, in a small group of patients with EDS on CPAP, a fluorodeoxyglucose-positron emission tomography study found reduced glucose utilization in the frontal area, but lacked a control group [65]. Conversely, other studies have shown that RES on CPAP treatment was associated with changes in cerebral magnetic resonance imaging especially regarding white matter, which correlated with the post-CPAP changes in psychomotor vigilance test and ESS [66, 67]. Improvement in cerebral imaging technology is expected to provide more data and allow a deeper understanding of the dysfunction associated with persistent EDS in treated OSA.
Future studies on residual EDS in OSA patients should also take into account the spontaneous variability of EDS documented in the general population. In a longitudinal study from Canada, based on data obtained by an annual online survey, 33% of the subjects were sleepy at baseline; over follow-up, initially sleepy subjects showed persistent EDS in 33%, intermittent EDS in 44%, and remitted EDS in 23% of cases [68]. The authors analysed predictors of improved EDS, which included a healthy lifestyle, normal body weight, low use of hypnotics, sufficient nightly sleep, and lack of insomnia or depressive symptoms. These results further highlight the complexity of the EDS symptom, and possible areas susceptible to educational interventions.
In addition to clinical studies, we should also consider the underlying pathological effects of RES and whether treating it could prevent cognitive decline. It has been hypothesised that OSA may cause irreversible hypoxic brain damage, thus accounting for the persistence of EDS after initiation of CPAP treatment. This hypothesis has been tested in animal models of chronic intermittent hypoxia or sleep fragmentation, but data in humans are scarce, since the majority of human studies aimed at assessing cognitive impairment without a specific focus on RES. Assessment of sleepiness in mice required the development of a protocol to perform MSLT, by taking into account the wake–sleep pattern typical of murine species [69].
Chronic intermittent hypoxia exposure for 6 months was associated with loss of 40% of wake-promoting catecholaminergic neurons in rodents [70], possibly explained by white matter loss [71] and vicious cycles of oxidative stress causing damage involving both neurons and microglia [72]. Similarly, neuronal damage in wake-active regions was found after 4 weeks of sleep fragmentation [73]. These studies are important pieces of evidence, but due to the lack of data in humans, the role of hypoxic damage in the pathogenesis or residual EDS remains currently unproven.
History of treatments for EDS in addition to CPAP
The concept of RES and recognition of the need to develop pharmacotherapy for treating RES in CPAP-treated patients appeared during the late 1990s. There was initially an intense debate regarding RES as a true pathological entity as some leading experts assumed that the prevalence of EDS in CPAP-treated OSA simply reflected a prevalent complaint in the general population [75].
The first pivotal studies evaluating modafinil and armodafinil as adjunct therapy in CPAP-treated patients were conducted in the years 2000–2010 [76, 77]. Modafinil, which had been used in narcolepsy since the early 1990s [78], was then used internationally to treat RES in OSA and was reported as improving the ESS score by ∼2 points and the MWT by ∼3 min over placebo [79, 80].
In addition, there was interest in modafinil as a possible adjunct during CPAP holidays to maintain neurobehavioural functioning (see table 3). This was explored by Williams et al. [81] in a small crossover study where the subjects used CPAP for four nights with one night off and then received either modafinil or placebo. Driving simulation, sleep diaries, cortical activation measures and subjective sleep questionnaires were used to investigate whether modafinil could prevent decline in function. Although a small study, it did show subjective but not objective maintenance of function, which the authors were concerned about in case this gave false reassurance to the user. However, this was a short withdrawal where CPAP may have masked the real decline that would be seen during longer withdrawal periods.
Effect of modafinil on continuous positive airway pressure (CPAP) withdrawal
The next study [82], also by the Sydney group, looked at a longer withdrawal period of two nights again in a crossover design. During the withdrawal, severe sleep-disordered breathing was seen and, in this case, modafinil did improve simulated driving performance as well as subjective sleepiness. The authors concluded that modafinil could be used to ameliorate performance when CPAP therapy was disrupted for some reason such as travelling or infections.
Wang et al. [83] further showed that CPAP withdrawal (with the same protocol) led to general slowing of electroencephalography (EEG) and this improved with modafinil. Alpha/delta ratio was a key biomarker of EEG activation, showing a correlation with improved subjective sleepiness and driving simulator performance with modafinil. This removes the subjective nature of some of the previous work as there is a clearer neurobiological pathway from EEG to sleepiness and performance.
In addition, a study from the Sydney group [84] showed that CPAP naïve subjects with mild to moderate OSA (AHI=5–30 events·h−1) with ESS 13.6 (3.3) also showed improvement in ESS and driving performance in a similar way to the withdrawal studies. The effect size on ESS with modafinil was greater than with CPAP in this group possibly due to poor levels of adherence in these patients. It should be noted that despite these studies modafinil is only licensed for narcolepsy in Australia.
During the same period, robust evidence was published regarding epidemiology, prevalence and clinical phenotypes of RES in OSA [54, 56], suggesting that this was a real syndrome that could benefit from treatment. However, there were safety concerns regarding modafinil/armodafinil and in 2011 the European Medicines Agency withdrew this indication owing to a poor benefit/risk ratio. It was considered that the risk of serious cardiovascular, neuropsychiatric, skin and hypersensitivity disorders prevailed over any potential benefit of treating residual EDS in patients with OSA. Thus, from 2011 to 2020 no pharmacological treatment was available in Europe for RES or as an adjunct to CPAP in OSA and only modafinil off-label use continued in a limited number of patients. Currently, modafinil and armodafinil remain approved in the United States, but not in Europe.
From 2019 to 2021, the efficacy of solriamfetol, a dopamine/norepinephrine reuptake inhibitor, has been established in randomised controlled trials and long-term open label studies (table 4).
Summary of clinical studies investigating novel wake-promoting drugs in obstructive sleep apnoea (OSA) (solriamfetol and pitolisant)
The initial study, TONES 3, [85], in 476 adults with OSA who were currently treated with CPAP, mandibular advancement device or surgery showed a dose-dependent improvement in subjective sleepiness (ESS decreased by 2–5 points) and objective sleepiness (MWT improved by 5–13 mins) compared with placebo over a 12-week period. There was also a dose-dependent response in cardiovascular effects with 300 mg giving a small rise in blood pressure. In a randomised withdrawal study, TONES 4, it was demonstrated that improvements in sleepiness were maintained in the active group compared to those withdrawn from the medication. It also showed no rebound phenomena once the drug was withdrawn [86]. A longer-term study in patients with narcolepsy or OSA, TONES 5 [87], showed that the short-term effects shown in these initial studies are maintained in both type of patients over a 6-month period. Solriamfetol has been approved in the United States and EU in 2020 at the 150 mg dosage for OSA, which shows small effects on blood pressure.
Pitolisant, a selective histamine receptor 3 antagonist/inverse agonist, has been used worldwide to treat EDS and cataplexy in narcolepsy very effectively for a number of years following the HARMONY 1 randomised placebo-controlled trial [88]. More recently, two pivotal studies have demonstrated efficacy of pitolisant in two distinct populations of OSA patients, adherent to CPAP [89] and refusing or not tolerating CPAP [90], respectively. In HAROSA 1 (n=244), CPAP-adherent patients showed an improvement in ESS and the Oxford Sleep Resistance Test (a behavioural MWT test) with no safety concerns. HAROSA 2 investigated 268 adults with OSA who had refused CPAP and showed a 2.8-point improvement in ESS with no cardiovascular or safety concerns. There will be long-term data for pitolisant in the OSA population published soon, but in the meantime pitolisant has been approved, at the 20 mg dose, in the EU in 2021 for these two distinct indications.
There will be concerns from sleep physicians that clinical trials involving patients who are intolerant of CPAP have been carried out and could lead to higher rates of non-use if stimulants were prescribed. However, consistent data from large-scale studies are demonstrating that the rate of CPAP termination is up to 45% at 3 years after CPAP initiation [91]. Implementation of alternatives to CPAP remain limited in routine practice [15, 92], and the majority of these patients stay untreated. Recent data demonstrate in real-life that CPAP discontinuation is associated with an increase of 39% in mortality rates [93]. Beyond mortality, quality of life and fitness to drive are altered in a subgroup of these patients. For these reasons, research was conducted to address efficacy of stimulants in this specific situation of untreated or nonadherent OSA [94, 95]. In these studies, the range of efficacy for improving sleepiness was the same for adherent and nonadherent patients. Other drugs such as methylphenidate, used in narcolepsy, are unlikely to be used in this patient group due to their high cardiovascular risk profile, which also makes it difficult to design clinical trials using these medications. There is a dilemma for sleep physicians with all these wake-promoting agents as there is potential harm against the benefits of improving symptoms of RES. Therefore, for these reasons, prescription, if any, in patients without primary therapy for OSA probably requires it to be strictly limited to expert centres after appropriate evaluation and a cautious follow-up regarding safety.
Future research questions
Should the indications of wake-stimulating agents be limited to OSA patients adequately treated by CPAP or extended to those not tolerating primary therapy?
Prospective registries should be implemented to assess long-term benefits and safety, specifically in OSA with cardiometabolic comorbidities including cognitive deficits.
What is the impact of stimulants on CPAP adherence with attention specially paid to the subgroup of intermittent users?
Could wake-promoting agents favour a healthier lifestyle, e.g. increased physical activity?
Would resolution of EDS help improve cognition?
What parameters would a sleep physician use to decide on a particular wake-promoting agent?
Conclusions
EDS is a major but not universal feature of OSA. The majority of population-based data imply that EDS is a marker of poor outcome, but the prognostic role of persistent EDS in treated patients is unknown although animal models appear to suggest a link with cognitive decline.
In the meantime, sleep physicians now have more varied treatments available for OSA and RES. These newer drugs potentially allow us to treat CPAP adherent and nonadherent patients without the cardiovascular concerns associated with older medications. However, available data suggest that assessment of RES should only be considered after the first 6 months of treatment, since EDS may spontaneously resolve in about half of sleepy patients [57].
Footnotes
Provenance: Submitted article, peer reviewed.
Conflict of interest: S. Craig reports receiving grants or contracts from UCB (Xyrem), outside the submitted work. Support for attending meetings and/or travel received from Bioprojet, outside the submitted work. Other disclosures outside the submitted work: Member of advisory board for Bioprojet. NICE committee meetings 2021 on behalf of British Thoracic Society investigating Pitolisant and Solriamfetol.
Conflict of interest: J-L. Pépin reports receiving grants or contracts from Air Liquide Foundation, AstraZeneca, Agiradom, Fisher and Paykel, Mutualia, Philips, Resmed, Vitalaire, Agiradom, AstraZeneca, Boehringer Ingelheim, Jazz pharmaceuticals, Night Balance, Philips, Resmed, and Sefam, outside the submitted work.
Conflict of interest: W. Randerath reports receiving payment for lectures, presentations, speakers’ bureaus, manuscript writing or educational events from Weinmann, Heinen & Löwenstein, Resmed, Jazz Pharmaceuticals, Inspire, Philips Respironics, Bioprojet, and Vanda Pharma, outside the submitted work. Support for attending meetings and/or travel from Heinen & Löwenstein, Resmed, Inspire, Philips Respironics, and Bioprojet, outside the submitted work. Participation on an Advisory Board for Bioprojet, Jazz Pharmaceuticals, and Philips Respironics, outside the submitted work.
Conflict of interest: C. Caussé reports support for the present manuscript received from Bioprojet company, for whom they are a current paid employee.
Conflict of interest: J. Verbraecken reports grants or contracts received from Air Liquide, Bekaert Deslee Academy, Bioprojet, Fisher & Paykel, Heinen & Löwenstein, Inspire, Jazz Pharmaceuticals, Medidis, Mediq Tefa, Nightbalance, OSG, Philips, ResMed, Sanofi, SomnoMed, Total Care, UCB Pharma, Vivisol, Wave Medical, and Westfalen Medical, outside the submitted work. Consulting fees received from Ectosense, outside the submitted work. Payment or honoraria for lectures, presentations, speakers’ bureaus, manuscript writing or educational events from AstraZeneca, Bioprojet, SomnoMed, TotalCare, and OSA Academy, outside the submitted work. Support for attending meetings and/or travel from Bioprojet, outside the submitted work. Participation on a Data Safety Monitoring Board or Advisory Board for Bioprojet, Desitin, Idorsia, Resmed Arval, outside the submitted work. Leadership or fiduciary role in other board, society, committee or advocacy group, paid or unpaid: past-president of the Belgian Association for Sleep research and Sleep medicine, outside the submitted work.
Conflict of interest: J. Asin reports receiving grants or contracts from Philips and Somnomed, Academy and Somnomed, and Jazz Pharmaceuticals, outside the submitted work. Support for attending meetings and/or travel received from Jazz Pharmaceuticals, Bioproject and GSK, outside the submitted work. Participation on a Data Safety Monitoring Board or Advisory Board for Bioproject and Jazz Pharmaceuticals, outside the submitted work. Leadership or fiduciary role in other board, society, committee or advocacy group: SVNL (Dutch Sleep Society) committee meetings as member of the board, unpaid. Involvement with the Dutch OSA Guidelines as member of the SRBD committee of the NVALT, unpaid. All disclosures made outside the submitted work.
Conflict of interest: F. Barbé reports receiving consulting fees from Jazz Pharmaceuticals, outside the submitted work. Support for attending meetings and/or travel received from Bioprojet, outside the submitted work. Participation on a Data Safety Monitoring Board or Advisory Board for Bioproject, outside the submitted work.
Conflict of interest: M.R. Bonsignore reports receiving payments for lectures, presentations, speakers’ bureaus, manuscript writing or educational events for Bioprojet and Jazz Pharmaceuticals, outside the submitted work. Participation on a Data Safety Monitoring Board or Advisory Board for Bioprojet and Eisai, outside the submitted work.
- Received October 11, 2021.
- Accepted March 28, 2022.
- Copyright ©The authors 2022
This version is distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0. For commercial reproduction rights and permissions contact permissions{at}ersnet.org
References










