





Abstract
Patients suffering from chronic obstructive pulmonary disease (COPD) clinically manifest airway mucus hypersecretion as sputum expectoration and cough. Evidence accumulated in the past decade has shown that the cholinergic system not only regulates airway smooth muscle contraction but also the activity of inflammatory and airway epithelial cells, including goblet cells, and submucosal gland activity. Long-acting muscarinic antagonists (LAMAs) with the most favourable M3/M2 muscarinic acetylcholine (ACh) receptors residency properties are not only excellent bronchodilators but potentially also mucus-modifying agents, able to positively impact on mucus hypersecretion and cough. The aim of this systematic review was to investigate the impact of LAMAs on mucus hypersecretion and cough in COPD patients. The evidence confirmed that LAMAs, mainly tiotropium and aclidinium, improved sputum production and cough in moderate to severe COPD. Thus, LAMAs not only antagonise the ACh-induced bronchoconstriction of the airways but also appear to limit the production of mucus secreted in response to ACh by airway goblet cells and/or submucosal glands. Further clinical studies are necessary to evaluate the impact of LAMAs exclusively on sputum symptoms and cough as primary end-points and to investigate whether LAMAs have a modulatory action on the rheological properties of mucus.
Abstract
This systematic review provides evidence that LAMAs, mainly tiotropium and aclidinium, have a beneficial impact on mucus hypersecretion and mucociliary clearance, with consequent improvement of sputum production and cough in moderate to severe COPD. https://bit.ly/3wHXZiZ
Introduction
Chronic obstructive pulmonary disease (COPD) is a major public health problem [1] projected to become the third leading cause of death worldwide by 2030 [2], with a global increase in the estimated prevalence from 10.7% in 1990 to 13.1% in 2019 [3]. Patients suffering from COPD manifest characteristics of airway mucus hypersecretion, including sputum expectoration, cough, and goblet cell hyperplasia and metaplasia [4].
Mucus secretion constitutes a physiological protective mechanical and immunological barrier for the airway epithelium against pathogens and environmental noxious agents [5–7]. However, mucus hypersecretion represents a risk factor for accelerated decline in lung function, pulmonary infections, limitation of physical activity and worsened quality of life [8]. Chronic mucus hypersecretion among middle-aged smokers represents an early developmental phase of COPD and it is characterised by a dynamic remitting–relapsing course across life. Interestingly, it has been demonstrated that COPD patients may report long episodes of chronic mucus hypersecretion across ages 43–64 years, and that each of these events may lead to an additional decrement of 3.6 mL·year−1 in forced expiratory volume in 1 s (FEV1) [9]. Of note, luminal occlusion of small airways with mucus-containing inflammatory exudates has been negatively correlated with lung function, and increases over the entire range of COPD severity [10]. Mucus control in small airways serves as an important therapeutic target to reduce the rate of emphysema progression and improve the prognosis of COPD [11, 12].
Even current or former smokers with preserved pulmonary function who do not meet the current criteria for COPD may have evidence of airway disease and symptoms related to sputum production and cough, so-called “simple chronic bronchitis” [13].
Chronic mucus hypersecretion is reported to be an additional risk factor for death from COPD in patients with impaired lung function. An in-depth analysis of the association between chronic mucus hypersecretion and mortality in COPD showed that the risk of death varied according to the level of ventilatory function, being weak in patients with normal ventilatory function and greater in patients with reduced ventilatory function in which a relative risk of 4.2 was reached for FEV1 values below 40% pred [14].
At present, bronchodilator drugs are the cornerstone treatment for COPD, including long-acting β2-adrenoceptor agonists (LABAs) and long-acting muscarinic antagonists (LAMAs) [15]. According to the 2021 GOLD recommendations [1], the initial pharmacological treatment for symptomatic patients at low risk of exacerbations is either an LAMA or an LABA, while dual bronchodilator therapy with a LABA/LAMA combination should be considered in patients with very severe symptoms and increased exacerbation risk. LAMA monotherapy is suggested as the initial treatment choice in symptomatic patients at high risk of exacerbations [1].
There is accumulating evidence that the cholinergic system not only regulates airway smooth muscle (ASM) contraction but also the functions of inflammatory and airway epithelial cells, including goblets cells, and submucosal gland activity. Hence it has been suggested that LAMAs could exert additional effects of clinical relevance in COPD patients [16]. LAMAs are indeed characterised by intrinsic enhanced M3/M2 muscarinic acetylcholine (ACh) receptors (mAChRs) binding properties, making them not only effective bronchodilators but also mucus-modifying therapies [16], able to positively impact airway mucus hypersecretion.
The objective of this systematic review was to evaluate the impact of LAMAs on mucus hypersecretion and cough in COPD patients. In order to avoid any possible bias related to the use of the different inhaler devices used in comparator groups, the impact of LAMAs has been assessed relative to baseline or placebo (PCB) and not compared to other medications.
Methods
Review question
The question of this systematic review was to evaluate the impact of LAMAs on mucus hypersecretion and cough in COPD patients.
Search strategy and study eligibility
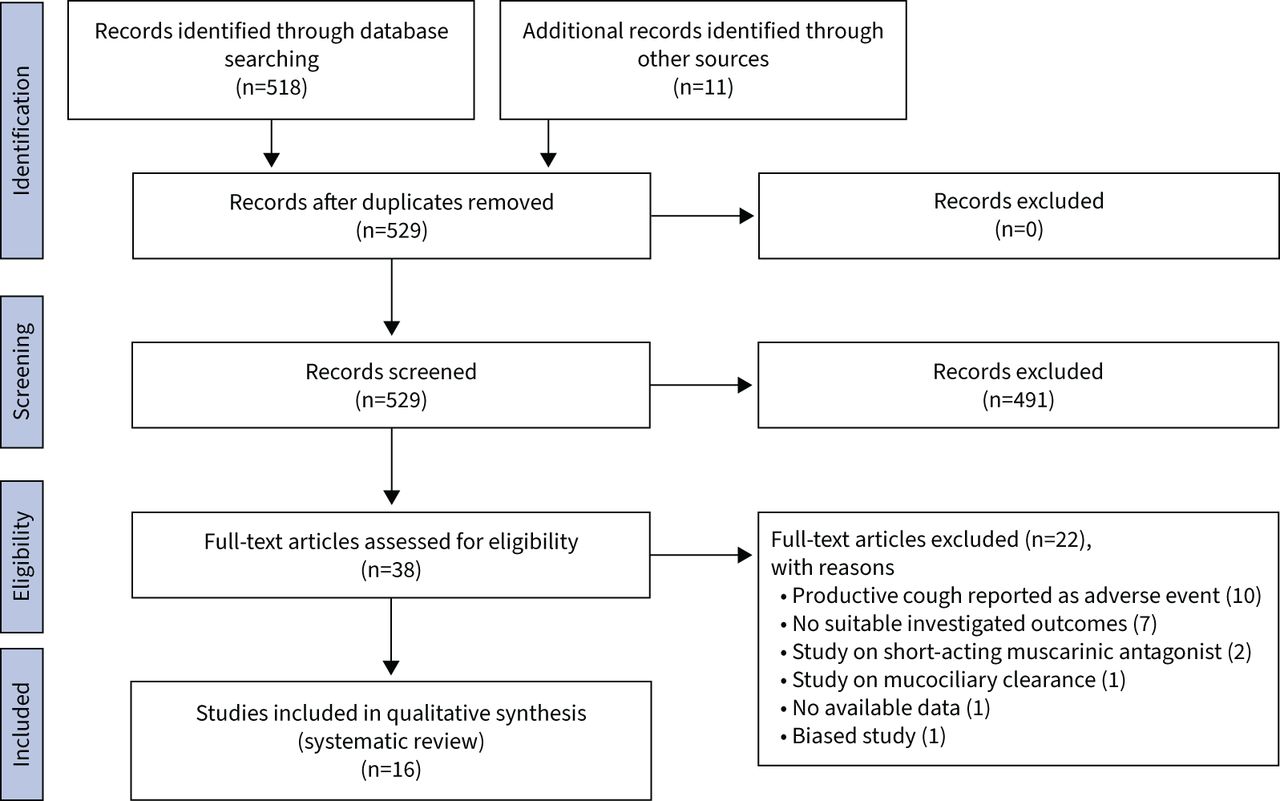
The protocol of this synthesis of the current literature has been registered in PROSPERO (CRD42021254586, protocol available at www.crd.york.ac.uk/prospero/display_record.php?RecordID=254586); the protocol has been amended and updated in PROSPERO by also including cough along with mucus as an outcome, according to the comments during peer review. This systematic review was performed in agreement with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis Protocol (PRISMA-P) [17], with the relative flow diagram shown in figure 1. This study satisfied all the recommended items reported in the PRISMA 2020 checklist available as supplementary material [17].
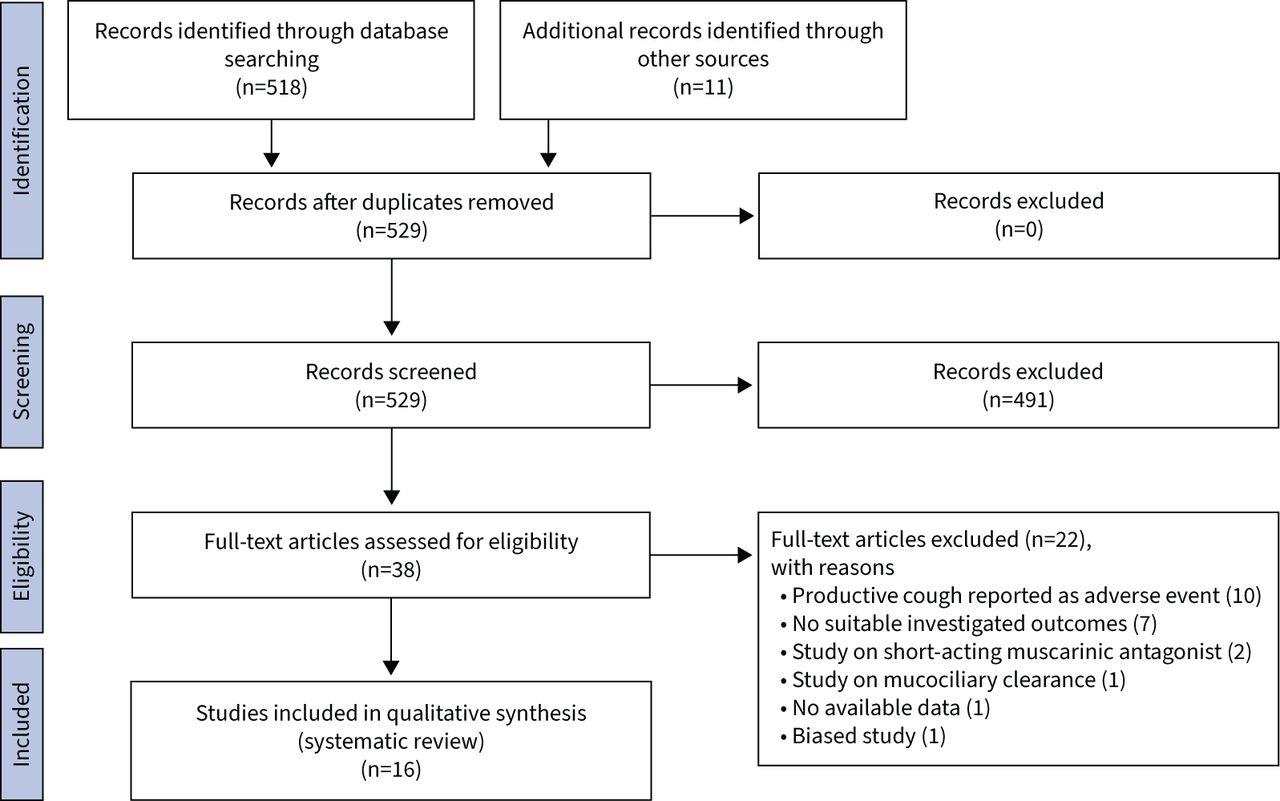
Flow diagram for the identification of the clinical studies included in the systematic review.
The PICO (Patient problem, Intervention, Comparison, and Outcome) framework was applied to develop the literature search strategy and question, as previously reported [18]. Namely, the “patient problem” included subjects affected by COPD, the “intervention” regarded the administration of LAMAs, the “comparison” was performed with respect to baseline or PCB, and the assessed “outcomes” were mucus hypersecretion and cough.
A comprehensive literature search was performed for studies evaluating the impact of LAMAs on mucus hypersecretion and cough in COPD patients. The search was performed in ClinicalTrials.gov, Cochrane Central Register of Controlled Trials (CENTRAL), Embase, EU Clinical Trials Register, MEDLINE, Scopus and Web of Science in order to provide relevant studies available with no time limit up to 29 April 2021. The research string was as follows: ((“pulmonary disease, chronic obstructive”[MeSH Terms] OR (“pulmonary”[All Fields] AND “disease”[All Fields] AND “chronic”[All Fields] AND “obstructive”[All Fields]) OR “chronic obstructive pulmonary disease”[All Fields] OR “copd”[All Fields]) AND (“aclidinium”[All Fields] OR (“glycopyrrolate”[MeSH Terms] OR “glycopyrrolate”[All Fields] OR “glycopyrronium”[All Fields]) OR (“glycopyrrolate”[MeSH Terms] OR “glycopyrrolate”[All Fields]) OR (“revefenacin”[Supplementary Concept] OR “revefenacin”[All Fields]) OR (“tiotropium bromide”[MeSH Terms] OR (“tiotropium”[All Fields] AND “bromide”[All Fields]) OR “tiotropium bromide”[All Fields] OR “tiotropium”[All Fields]) OR (“gsk573719”[Supplementary Concept] OR “gsk573719”[All Fields] OR “umeclidinium”[All Fields]) OR “LAMA”[All Fields] OR (“receptors, muscarinic”[MeSH Terms] OR (“receptors”[All Fields] AND “muscarinic”[All Fields]) OR “muscarinic receptors”[All Fields] OR (“muscarinic”[All Fields] AND “receptor”[All Fields]) OR “muscarinic receptor”[All Fields])) AND (“mucus”[MeSH Terms] OR “mucus”[All Fields] OR (“sputum”[MeSH Terms] OR “sputum”[All Fields] OR “sputums”[All Fields]) OR (“hypersecrete”[All Fields] OR “hypersecreted”[All Fields] OR “hypersecretes”[All Fields] OR “hypersecreting”[All Fields] OR “hypersecretion”[All Fields] OR “hypersecretions”[All Fields]) OR (“bodily secretions”[MeSH Terms] OR (“bodily”[All Fields] AND “secretions”[All Fields]) OR “bodily secretions”[All Fields] OR “secretions”[All Fields] OR “metabolism”[MeSH Subheading] OR “metabolism”[All Fields] OR “secretion”[All Fields] OR “metabolism”[MeSH Terms] OR “secretable”[All Fields] OR “secrete”[All Fields] OR “secreted”[All Fields] OR “secretes”[All Fields] OR “secreting”[All Fields]) OR “mucociliary”[All Fields] OR (“clearance”[All Fields] OR “clearances”[All Fields]) OR ((“submucosal”[All Fields] OR “submucosally”[All Fields]) AND (“gland”[All Fields] OR “gland s”[All Fields] OR “glands”[All Fields])) OR (“goblet cells”[MeSH Terms] OR (“goblet”[All Fields] AND “cells”[All Fields]) OR “goblet cells”[All Fields] OR (“goblet”[All Fields] AND “cell”[All Fields]) OR “goblet cell”[All Fields]) OR (“cough”[MeSH Terms] OR “cough”[All Fields] OR “coughing”[All Fields] OR “coughs”[All Fields] OR “coughed”[All Fields]))) AND (clinicalstudy[Filter] OR clinicaltrial[Filter] OR randomizedcontrolledtrial[Filter]). Citations of previous published relevant reviews were examined to select further pertinent studies, if any [19–21].
Two reviewers independently checked the relevant studies identified from the literature search. Studies concerning the effect of LAMAs on mucus hypersecretion and cough in COPD patients were selected and included in the systematic review and any difference in opinion about eligibility was resolved by consensus.
Data extraction
Data from included studies were extracted in agreement with Data Extraction for Complex Meta-anALysis (DECiMAL) recommendations [22], and checked for study references and characteristics, number and characteristics of the analysed patients, age, gender, treatments and comparators with doses of medications and type of inhaler, smoking habits, FEV1, outcome measurements to evaluate the impact on mucus hypersecretion and cough, and Jadad score.
End-points
The primary end-point of this systematic review was to assess the impact of LAMAs on mucus hypersecretion in COPD patients. The secondary end-point was to assess the impact of LAMAs on cough in COPD patients.
Strategy for data analysis
Data from original papers were extracted and reported via qualitative synthesis. ImageJ software was used to extract data from the figures when necessary [23].
Quality of studies and risk of bias
The summary of the risk of bias for each included randomised clinical study was analysed via Cochrane Risk of Bias (RoB) 2 [24] by using the robvis visualisation tool [25], and the Jadad score [26]. The RoB 2 tool consists of five domains assessing the bias for the randomisation process, deviations from intended intervention, missing outcome data, measurement of the outcome, and selection of the reported results [24].
The Jadad score ranging from 1 to 5 (score of 5 being the best score) was used to assess the quality of the papers concerning the likelihood of bias related to randomisation, double-blinding, withdrawals, and dropouts [26]. The quality of studies was ranked as follows: score<3, low quality; score=3, medium quality; score>3, high quality. The weighted assessment of the risk of bias was analysed via Cochrane RoB 2 [24].
Two reviewers independently assessed the quality of the studies and the risk bias, and any difference in opinion was resolved by consensus.
Results
Study characteristics
Of the 529 potentially relevant records identified in the initial search, 16 studies were deemed eligible for a qualitative analysis (table 1).
Main characteristics and results of the studies included in the systematic review
This systematic review included data obtained from studies performed on patients with moderate to severe COPD. The investigated LAMAs were tiotropium (TIO) [27–36], aclidinium (ACL) [27, 29, 31, 37–42] and glycopyrronium (GLY) [30]. Overall, 13 studies [31–37, 42–47] were randomised controlled trials (RCTs), among which seven [31, 42–47] were derived from post hoc analyses [27, 29, 30, 38, 40], two studies [39, 41] were performed in real-world settings, and one study [28] was non-randomised and non-controlled. No studies on revefenacin or umeclidinium were identified from the literature search. Detailed dosages with regimens of administration are reported in table 1.
Tiotropium
Mucus hypersecretion
Tagaya et al. [28] conducted a small non-PCB-controlled study to assess whether treatment with TIO modulated mucus hypersecretion and airway clearance in patients with COPD who have never received anticholinergic drugs. Following 8-week therapy with TIO, the sputum severity domain significantly improved from 47.0 points to 64.0 points (p<0.001) and the sputum impact domain from 48.0 points to 57.0 points (p<0.05) [28]. TIO significantly (p<0.05) reduced the nasal mucociliary clearance time from 34.2 min to 21.6 min, the amount of solid components in the sputum from 3.40% to 2.63%, as well as the mucin content from 78.0 mg·mL−1 to 45.0 mg·mL−1 [28]. Powrie et al. [33] provided evidence that TIO was significantly (p=0.001) associated with a subjective decrease in sputum production in 33.0% of COPD patients compared to 7.9% administered with PCB. In a phase IIIb RCT, Beier et al. [31] detected a numerical reduction in severity of early-morning phlegm (−0.07 points) for TIO versus PCB in moderate to severe COPD patients.
A pooled post hoc analysis [30] reported that TIO significantly (p<0.05) reduced the sputum production symptom score over 12 weeks (−0.09 points), 26 weeks (−0.08 points) and 52 weeks of treatment (−0.09 points) in moderate to severe COPD patients. A post hoc analysis [29] of three phase III RCTs [31, 42, 46] confirmed the evidence reported by Beier et al. [31] and also found that TIO induced a numerical increase in the percentage of days without difficulty in bringing up phlegm (+4.8%), along with a decrease from baseline in the severity of phlegm (−0.09 points) [29]. In another post hoc analysis [27] exclusively focused on the treatment response of symptomatic moderate to severe COPD patients, TIO numerically improved the early-morning symptom severity score for phlegm (−0.10 points, −11.2%), compared to PCB.
Overall, TIO decreased the occurrence of symptoms related to expectoration, possibly by inhibiting airway mucus hypersecretion and improving the rate of mucociliary clearance [28].
Cough
A study carried out by Tagaya et al. [28] showed that TIO administered for 8 weeks significantly improved the cough severity domain from 45.0 points to 64.0 points (p<0.001) and the cough impact domain from 44.0 points to 54.0 points (p<0.05) [28]. Overall, TIO improved the occurrence of symptoms related to cough [28]. Hasani et al. [34] performed a 3-week RCT in COPD patients showing that cough frequency was reduced with TIO by 8.0 coughs and increased with PCB by 4.0 coughs during a 6 h observation period [34]. Beier et al. [31] reported a numerical reduction in cough scores (−0.10 points) for TIO versus PCB in moderate to severe COPD patients [31].
A pooled post hoc analysis in moderate to severe COPD patients reported that TIO elicited a numerical reduction in the cough symptom score (week 12: −0.04 points; week 26: −0.05 points; week 52: −0.04 points) [30]. In patients with stable COPD, TIO reduced the symptom score for cough after 8 days of treatment by 0.16 points [36], although at weeks 13 and 52 no difference was detected compared to PCB [35, 36].
Results of a post hoc analysis [29] of three phase III RCTs [31, 42, 46] indicated that TIO elicited a numerical increase in the percentage of days without morning cough symptoms (+5.5%) associated with a decrease from baseline in the severity of morning cough (−0.11 points) [29]. Another post hoc analysis [27] aimed to assess the treatment response of symptomatic moderate to severe COPD patients reported that TIO numerically improved the early-morning symptom severity scores for cough (−0.09 points, −6.5%), compared to PCB.
According to a phase IV RCT [32], 12 weeks of TIO administration provided a reduction from baseline in symptom score for cough (−0.088 points) and the improvement was further increased when TIO was combined with budesonide (BUD)/formoterol (FOR) fixed-dose combination (FDC) (−0.250 points).
Exacerbations of Chronic Pulmonary Disease Tool (EXACT)–Respiratory Symptoms (E-RS) cough and sputum domain
Results from a phase IIIb RCT [31] reported a numerical reduction in the E-RS cough and sputum domain symptom score for TIO versus PCB (−0.2 points) [31]. This result was confirmed by post hoc analysis of symptomatic moderate to severe COPD patients indicating that TIO numerically improved the E-RS cough and sputum domain score by −0.2 points (−4.4%), compared to PCB [27].
Aclidinium
Mucus hypersecretion
A phase IIIb RCT [31] in moderate to severe COPD patients reported that, following 6 weeks of treatment with ACL, the severity of early-morning phlegm evaluated by a COPD symptom questionnaire was significantly (p<0.05) reduced by −0.17 points versus PCB [31].
Beier et al. [27] conducted a post hoc analysis of the above-mentioned phase IIIB RCT [31] to assess the impact of treatment with ACL exclusively in symptomatic patients with moderate to severe COPD. ACL demonstrated a numerical improvement in the early-morning symptom severity score for phlegm by 0.20 points (−16.5%) versus PCB.
A post hoc analysis [29] of three phase III RCTs, namely the ATTAIN [46], the ACCORD COPD I [42] and a phase IIIb RCT [31], reported that 24 weeks of treatment with ACL significantly (p<0.01) reduced the percentage of days with difficulty in bringing up phlegm or mucus compared to PCB (−8.6%). Likewise, the percentage of days with night-time symptoms due to difficulty in bringing up phlegm or mucus was significantly (p<0.01) reduced with ACL compared to PCB (−3.0%) [29]. ACL also produced a numerically higher percentage of days without morning difficulty in bringing up phlegm versus PCB [29]. ACL significantly (p<0.05) reduced the frequency of night-time sputum production versus PCB (−0.37 points versus 0.05 points) [29]. The treatment with ACL also significantly (p<0.05) improved symptom scores of phlegm versus PCB (−0.19 points versus −0.02 points) [29].
Bateman et al. [40] analysed pooled data from the ACLIFORM [43] and AUGMENT COPD I [47] phase III RCTs to evaluate the effect of ACL/FOR FDC on mucus-related symptoms in patients with moderate to severe COPD. Over 24 weeks of treatment, ACL/FOR FDC versus PCB significantly (p<0.05) reduced the early-morning and night-time difficulty in bringing up phlegm (−0.11 points and −0.10 points, respectively) [40].
The real-life study by Marth et al. [41] provided evidence that ACL elicited a significant (p<0.0001) reduction from baseline in the COPD Assessment Test (CAT) score for phlegm by −0.67 points, and the improvement was similar across patients with either newly diagnosed or previously known COPD. Another real-life study, performed by Lange et al. [39], confirmed that with up to 24 weeks of treatment, ACL significantly (p<0.001) decreased the CAT score for mucus (−0.44 points).
Cough
Treatment with ACL for 6 weeks significantly (p<0.05) reduced, by −0.17 points versus PCB, the severity in early-morning cough [31]. A post hoc analysis [27] of the above-mentioned study [31] in symptomatic patients with moderate to severe COPD reported that, when compared to PCB, ACL significantly (p<0.01) reduced the early-morning symptom severity score for cough by −0.19 points (−12.5%).
A post hoc analysis [29] of three phase III RCTs [31, 42, 46] showed that treatment with ACL for 24 weeks significantly (p<0.01) reduced the percentage of days with morning cough compared to PCB (−5.4%). Furthermore, the percentage of days with night-time symptoms due to cough was significantly (p<0.01) reduced with ACL compared to PCB (−7.0%) [29]. ACL also provided a significant (p<0.05) increase by 7.2% in the percentage of days without morning cough symptoms versus PCB [29]. ACL versus PCB significantly (p<0.05) reduced the night-time symptom score for cough frequency (−0.36 points versus 0.10 points) and severity (−0.24 points versus −0.10 points) [29]. ACL also significantly (p<0.05) improved symptom scores of morning cough versus PCB (−0.19 points versus −0.02 points) [29].
Pooled analysis [40] of ACLIFORM [43] and AUGMENT COPD I [47] phase III RCTs in patients with moderate to severe COPD showed that, when compared to PCB, ACL/FOR FDC significantly (p<0.05) reduced early-morning and night-time symptom scores for cough (−0.05 points and −0.07 points, respectively) [40].
Two real-life studies [39, 41] evaluated the effect of treatment with ACL on cough-related outcomes in COPD patients. The study by Marth et al. [41] showed that ACL was effective in significantly (p<0.0001) reducing the CAT score for cough by −0.70 points versus baseline, reporting similar improvement in patients with either newly diagnosed or with previously known COPD. Lange et al. [39] also reported that 24 weeks of treatment with ACL induced a significant (p<0.001) decrease in the CAT score for cough (−0.34 points). Furthermore, at the end of the study [39] period, the severity of cough assessed via a six-point Likert scale was significantly (p<0.001) improved during morning by 0.33 points and during night-time by 0.23 points.
E-RS cough and sputum domain
A phase IIIb RCT [31] reported that following 6-weeks of treatment with ACL, the E-RS cough and sputum domain score was significantly (p<0.05) improved by −0.4 points versus PCB, in moderate to severe COPD patients. The post hoc analysis [27] of the above-mentioned study [31] focused on symptomatic patients with moderate to severe COPD indicated that ACL significantly (p<0.01) reduced the E-RS cough and sputum domain score by −0.5 points (−10.8%) versus PCB.
Another post hoc analysis of three phase III RCTs showed that ACL significantly (p<0.01) reduced the E-RS cough and sputum domain score by −0.4 points versus PCB [29]. Patients experiencing ≥1 exacerbation presented a similar E-RS cough and sputum domain score at baseline between ACL and PCB groups and after 24 weeks of treatment with ACL, the E-RS cough and sputum domain score was significantly (p<0.01) reduced by −0.5 points [29].
A pooled post hoc analysis [38] of two phase III RCTs, namely ATTAIN [46] and AUGMENT COPD I [47], evaluated the effect of ACL on symptoms in the overall COPD population pooled from the two studies and in COPD patients stratified into GOLD groups with either few (GOLD A+C) or high symptoms (GOLD B+D). The improvement from baseline in the E-RS cough and sputum domain scores was significantly (p<0.05) greater with ACL than PCB in the overall COPD population (−0.70 points versus −0.31 points), in the GOLD A+C group (−0.44 points versus −0.01 points) and in the GOLD B+D group (−0.68 points versus −0.33 points) [38]. Patients treated with ACL were significantly (p<0.05) more likely to be E-RS cough and sputum domain scores responders compared to those receiving PCB (odds ratio (OR) 1.8) and this finding was also observed in the GOLD A+C group (OR 3.0) and in the GOLD B+D group (OR 1.7) [38]. Summarising, ACL was found to be effective at improving cough and sputum, regardless of symptom severity at baseline, and the beneficial impact was similar in groups with low or high levels of symptoms [38].
In a recent phase IV RCT [37], the efficacy of ACL on cough was investigated in patients with moderate COPD. Compared to PCB, ACL was shown to induce a numerical reduction of the E-RS cough and sputum domain score (−0.1 points) at week 4 of treatment and a significant (p<0.05) decrease of −0.3 points after 8 weeks [37]. ACL did not improve the Leicester Cough Questionnaire (LCQ) total score at any time point, although patients suffering from more severe cough symptoms at baseline reported a significant (p<0.05) reduction in the E-RS cough and sputum domain score versus PCB at both week 4 and week 8 of treatment (−0.3 points and −0.5 points, respectively), as well as a numerical improvement in LCQ total score (week 4: 0.6 points; week 8: 0.4 points) [37]. In patients with less severe cough, the E-RS cough and sputum domain score numerically decreased only after 8 weeks of treatment (−0.2 points), while the LCQ score did not improve at any time point [37].
Another pooled analysis [40] of ACLIFORM [43] and AUGMENT COPD I [47] phase III RCTs in patients with moderate to severe COPD reported that, over 24 weeks of treatment, ACL/FOR FDC significantly (p<0.001) improved the E-RS domain score for cough and sputum (−0.57 points) versus PCB (−0.35 points), whereas ACL administered alone induced a numerical reduction by −0.48 points [40].
Glycopyrronium
Mucus hypersecretion
According to a pooled post hoc analysis [30] of the Glycopyrronium bromide in COPD airWays 1 [44] and 2 [45] (GLOW1 and GLOW2) studies, GLY significantly (p≤0.01) improved the change from baseline in sputum production symptom score over 12 weeks (−0.06 points), 26 weeks (−0.08 points) and 52 weeks of treatment (−0.11 points) compared to PCB.
Cough
The pooled post hoc analysis [30] of the GLOW1 [44] and GLOW2 [45] studies indicated that GLY elicited a numerical reduction in the cough symptom score (week 12: −0.03 points; week 26: −0.04 points; week 52: −0.03 points).
E-RS cough and sputum domain
No data are currently available for GLY concerning the impact on the E-RS cough and sputum domain.
Quality of studies and risk of bias
The weighted plot for the assessment of the overall risk of bias by domains is shown in figure 2a, and the traffic light plot for the assessment of each included study is reported in figure 2b. Three studies [28, 39, 41] included in the systematic review could not be ranked in agreement with the Cochrane RoB 2 [24] and Jadad score [26] because they were either non-randomised [28] or performed in non-interventional, non-randomised, real-life settings [39, 41].

a) Traffic light plot for assessment of the risk of bias of each included randomised controlled trial and b) weighted plot for the assessment of the overall risk of bias via the Cochrane Risk of Bias 2 tool (n=16 studies, from 16 records).
Most of the clinical studies had a low risk of bias for the randomisation process (12; 92.3%), deviations from intended interventions (7; 53.8%), missing outcome data (13; 100.0%), measurement of the outcomes (11; 84.6%) and selection of the reported results (13; 100.0%).
Of the 13 RCTs, one (7.7%) had some concerns regarding the risk of bias for the randomisation process, two (15.4%) for deviations from intended intervention, and one (7.7%) for the measurement of the outcomes, whereas one study (7.7%) had a high risk of bias due to measurement of the outcome. Overall, four RCTs (30.8%) provided insufficient information for the assessment of bias in the domain of deviations from intended intervention.
Almost all of the included studies were ranked as being of medium to high quality in agreement with the Jadad score (table 1), except for one study [37] which was of low quality (Jadad score<3). Three studies [33, 44, 45] were of medium quality (Jadad score=3) and nine studies [31, 32, 34–36, 42, 43, 46, 47] were of high quality (Jadad score>3).
Discussion
This systematic review provides evidence that LAMAs elicit a beneficial effect by ameliorating mucus hypersecretion and cough in COPD patients, leading to an improvement of COPD exacerbation rate and lung function decline. Specifically, TIO was reported to improve sputum production [27, 30, 31, 33] and cough [27–32, 34], as well as the severity of early-morning cough and phlegm [29, 31]. Likewise, ACL was effective at reducing the frequency and severity of sputum expectoration and cough [27, 29, 31, 37, 38, 40], even in real-life settings [39, 41], and induced an improvement in the severity of early-morning and night-time phlegm and cough [27, 29, 31, 40]. TIO [28] achieved minimally important clinical differences (MCIDs) in the Cough and Sputum Assessment Questionnaire (CASA-Q) scores for cough and sputum severity [48]. ACL [38], but not TIO [27, 31], achieved MCIDs in the overall COPD population in the cough and sputum domain scores of the E-RS [49]. The evidence concerning GLY was limited, although a reduction of sputum production and cough was provided [30].
The mAChRs throughout the bronchial tree are mainly restricted to M1, M2 and M3 subtypes [50]. Neuronal and non-neuronal ACh activating M1 and M3 mAChRs brings on ASM contraction, airway remodelling, mucus secretion, and inflammation, whereas the activation of presynaptic postganglionic M2 mAChRs autoreceptors protects against vagally induced bronchoconstriction [51]. Indeed, blocking of mAChRs autoreceptors increases ACh-mediated contractility of ASM [52]. Thus, ideally an antimuscarinic agent should block M1 and M3 mAChRs, sparing M2 mAChRs. Fortunately, the current LAMAs have greater selectivity for M3 than for M2 mAChRs and dissociate more slowly from the M3 than from M2 mAChRs [50].
While at the level of large and medium bronchi mucus is produced by both goblet cells and submucosal glands, in small airways the only source of mucus is the goblet cell [53]. COPD is characterised by an increase in the number of goblet cells, and its progression is strictly related to the accumulation of mucus in the lumen of small airways, a condition that may contribute to the development of small airway disease [53, 54]. LAMAs do not specifically target mucus hypersecretion, they instead act by reversing the parasympathetic-induced bronchoconstriction in the human airways [55]. Vagally derived ACh induces mucus secretion mainly via M3 mAChRs expressed on submucosal glands, while electrolytes and water secretion are regulated via both M1 and M3 mAChRs [50]. Furthermore, goblet cells discharge airway mucus in response to ACh [50]. Interestingly, ACh is not solely a classical parasympathetic neurotransmitter, it should be also considered an autocrine or paracrine hormone synthesised and secreted by non-neuronal cells, including airway epithelial cells, fibroblasts and inflammatory cells [56–58]. The beneficial effect of LAMAs against mucus hypersecretion in large and medium bronchi and in small airways is shown in figure 3.

{kind=link}
{kind=link}
{kind=link}
The beneficial effect of long-acting muscarinic antagonists (LAMAs) against mucus hypersecretion in large and medium bronchi, and in small airways when using inhaler devices effective at delivering the drug into the small airway compartment. ACh: acetylcholine; LAMA: long-acting muscarinic antagonist; mAChRs: M3 muscarinic ACh receptors.
The cholinergic tone is elevated in COPD patients [59], leading to higher levels of ACh and ASM contraction, and to the production of the main macromolecular components of mucus, namely mucin glycoproteins, secreted by airway goblet cells and/or submucosal glands [60].
Up-regulation of the gel-forming mucin gene MUC5AC is implicated in the pathogenesis of COPD, and it may contribute to worsening of the clinical status of patients since it is a trigger for airways obstruction [9, 61]. Moreover, recent evidence from the Subpopulations Intermediate Outcome Measures in COPD Study suggested that airway mucin concentrations in the sputum of COPD patients were indicative of disease severity [62].
In agreement with pre-clinical findings, TIO was found to reduce MUC5AC overexpression [63, 64] and mucus gland hypertrophy in guinea pigs [63], and suppressed the neutrophil elastase-induced goblet cell metaplasia in mice by preventing mucin synthesis [11]. Likewise, Cortijo et al. [65] have shown that ACL inhibited the overexpression of MUC5AC induced by carbachol and cigarette smoke.
Airway mucus hypersecretion manifests clinically as chronic productive cough and sputum expectoration, both associated with an accelerated decline in lung function [66], increased risk for pulmonary infections [67] and higher rates of exacerbations and hospitalisations [68]. Not surprisingly, the prevalence of cough and expectoration in COPD patients has been estimated in the range between 14.0% and 74.0% [69–71]. In this regard, it has been speculated that the improvement in cough and sputum symptoms following treatment with LAMAs might result from the inhibition of airway mucus hypersecretion [28].
Surprisingly, there is an absence of controlled clinical trials concerning the impact of LAMAs on mucin synthesis, production and rheology [72], while there are conflicting findings regarding airway mucociliary clearance [28, 34, 73]. Tagaya et al. [28] reported that TIO reduced the nasal clearance time in COPD patients, an effect that could be the result of a lower mucus hypersecretion and an increase in mucociliary clearance time in the airways. By contrast, two [34, 73] small-scale studies failed to show an improvement of mucociliary clearance as a result of TIO inhalation.
The main limitations to this systematic review are related to the intrinsic characteristics of the included clinical studies. Specifically, the RCT by Smith et al. [37] was not powered for detecting LCQ scores, therefore it could not be considered sensitive enough to distinguish a change in patients’ symptoms. Likewise, McGarvey et al. [29] reported that none of the three RCTs included in their pooled post hoc analysis was adequately powered to detect changes in cough and sputum. Furthermore, Powrie et al. [33] relied on patients’ subjective perception for evaluating the impact of TIO on sputum production, without any quantitative assessment.
The assessment of cough and sputum, which serves as evidence of airway mucus hypersecretion, was generally performed by specific symptom questionnaires, such as the validated E-RS, LCQ and CASA-Q. Nevertheless, some of the included studies were characterised by the absence of a verified tool to evaluate the severity and impact of symptoms [31, 42]. In actual fact, there is no standardised method for quantifying airway mucus hypersecretion in COPD patients, which requires invasive procedures and so is seldom performed in clinical settings [4].
In addition, the clinical studies included in this systematic review mainly focused on patients suffering from moderate to severe COPD; therefore, follow-up research is necessary to evaluate the impact of LAMAs on airway mucus, across the whole range of disease severity.
To the best of our knowledge, this is the first systematic review exclusively focusing on the impact of LAMAs on airway mucus in COPD patients. Most of the studies published in the literature have mainly focused on improvements in lung function, breathlessness, and reductions in the risk of exacerbation. It is therefore necessary to conduct further clinical studies specifically designed to assess the impact of LAMAs on cough and sputum symptoms as primary end-points, as well as to ascertain the presence of a modulatory action on the rheological properties of mucus. Improvements in the efficacy of LAMAs on small airways disease in COPD can be achieved through the development of novel formulations and devices to deliver the drugs more uniformly to both large and small airways [12].
It would also be interesting to investigate whether the beneficial action of LAMAs on airway mucus hypersecretion could improve the efficacy of some classes of drugs targeting the airway epithelium. The reduction of the increased water-based polymeric mucus layer covering the airways as a liquid film and barrier might promote the penetration of drug particles, including LABAs and inhaled corticosteroids, thus working together for a more targeted therapeutic action.
Concluding, hypersecretion of mucus by airway goblet cells and submucosal glands, along with decreased elimination of mucus due to decreased mucociliary clearance, are the main mechanisms related to excessive mucus levels in the airways, a condition leading to adverse effects on important outcomes in COPD patients such as lung function, health-related quality of life, exacerbations, hospitalisations and mortality [74]. The findings reported by this systematic review indicate that LAMAs, mainly TIO and ACL, have a beneficial impact on mucus hypersecretion and mucociliary clearance, with consequent improvement in sputum production and cough in moderate to severe COPD patients.
Supplementary material
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
PRISMA checklist ERR-0196-2021.SUPPLEMENT
Footnotes
Provenance: Submitted article, peer reviewed.
Conflict of interest: L. Calzetta reports grants and personal fees from Boehringer Ingelheim, grants and personal fees from Novartis, non-financial support from AstraZeneca, grants from Chiesi Farmaceutici, grants from Almirall, personal fees from ABC Farmaceutici, personal fees from Edmond Pharma, grants and personal fees from Zambon, personal fees from Verona Pharma, and personal fees from Ockham Biotech.
Conflict of interest: B.L. Ritondo declares no conflict of interest.
Conflict of interest: M.C. Zappa declares no conflict of interest.
Conflict of interest: G.M. Manzetti. declares no conflict of interest.
Conflict of interest: A. Perduno declares no conflict of interest.
Conflict of interest: J. Shute is the Scientific Director of Ockham Biotech Ltd.
Conflict of interest: P. Rogliani reports grants and personal fees from Boehringer Ingelheim, grants and personal fees from Novartis, personal fees from AstraZeneca, grants and personal fees from Chiesi Farmaceutici, grants and personal fees from Almirall, grants from Zambon, personal fees from Biofutura, personal fees from GlaxoSmithKline, personal fees from Menarini, and personal fees from Mundipharma.
- Received August 24, 2021.
- Accepted March 20, 2022.
- Copyright ©The authors 2022
This version is distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0. For commercial reproduction rights and permissions contact permissions{at}ersnet.org
References










