





Abstract
The updated analysis suggests that SSD has a favourable impact in the incidence of VAP rates but will have a limited impact on other outcomes, such as shorter duration of mechanical ventilation, ICU length-of-stay, and lower mortality rates https://bit.ly/3rEuzPI
To the Editor:
The aim of this correspondence is to amend a mistake in our original article [1], and to recalculate our meta-analyses for ventilator-associated pneumonia (VAP) and mortality outcomes.
The original paper consisted of an overview of nine systematic reviews and an updated meta-analysis of randomised trials examining the effectiveness of subglottic secretion drainage (SSD) in reducing VAP incidence, duration of mechanical ventilation, intensive care unit (ICU) and hospital length of stay, and mortality. Our original meta-analysis suggested SSD was associated with a significant decrease in the incidence of VAP (risk ratio (RR) 0.56, 95% CI 0.48–0.63; I2=0%) and mortality (RR=0.88, 95% CI 0.80–0.97; I2=0%).
We have since detected two errors in our paper. First, in the original figure 3, which analysed the association between SSD and mortality, the study by Damas et al. [2] was inadvertently counted twice (once for hospital mortality, once for ICU mortality). In the corrected version, we only included the data from Damas et al. [2] on hospital mortality. Secondly, in the original figure 3, in the study by Bouza et al. [3], we mistakenly included the “per protocol” results instead of the “intention to treat” data in the analyses for mortality and VAP incidence outcomes. Thus, a recalculation of the meta-analysis is warranted.
After correction, the new results continue to show an association between SSD and lower incidence of VAP (RR 0.60, 95% CI 0.53–0.68, p<0.001; I2=0%) (figure 1). However, the estimates for mortality are modified (RR 0.92, 95% CI 0.83–1.02, p=0.098; I2=0%) (figure 2), suggesting a nonsignificant trend towards lower mortality in patients randomised to SSD.
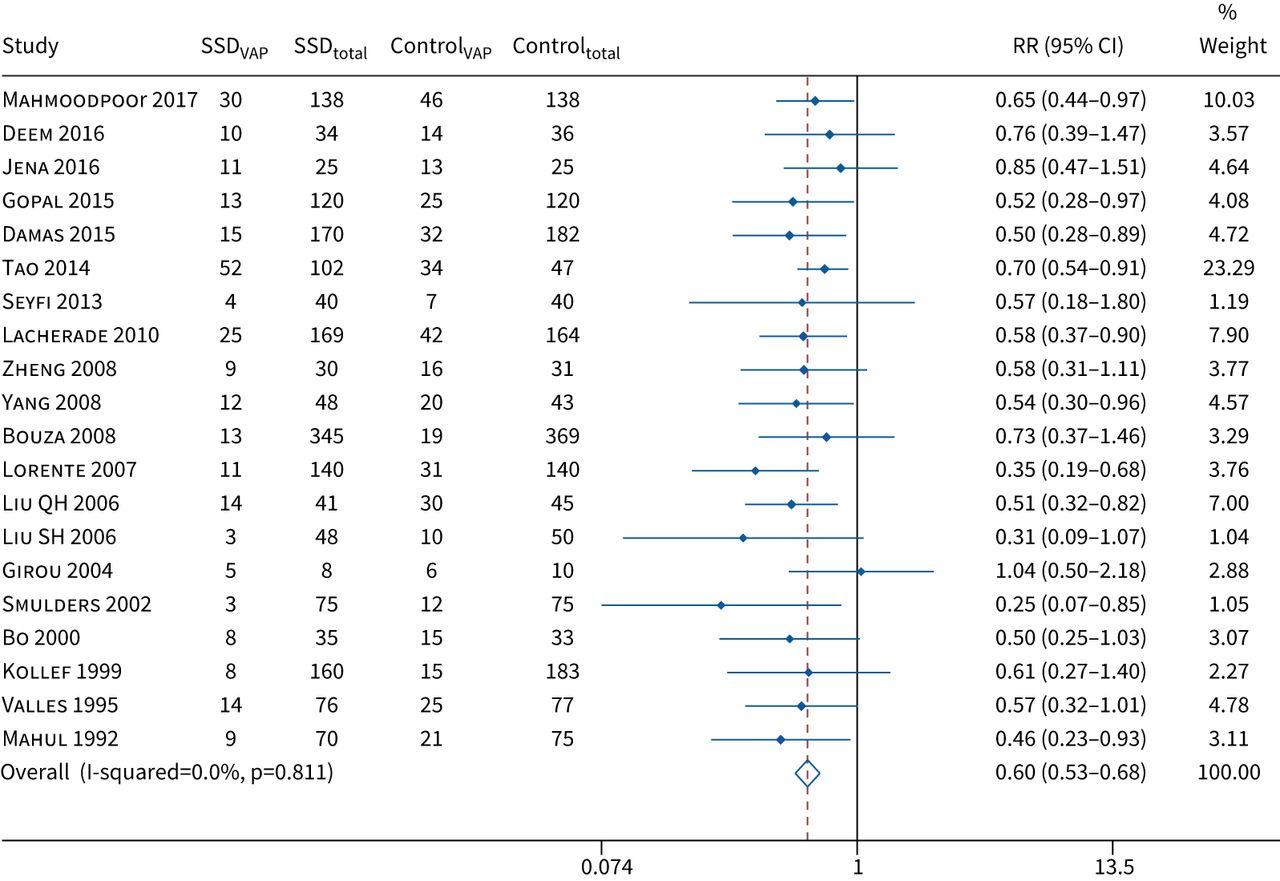
Forest plot comparing subglottic secretion drainage (SSD) versus non-SSD on the incidence of ventilator-associated pneumonia (VAP). RR: risk ratio.

{kind=link}
{kind=link}
Forest plot comparing subglottic secretion drainage (SSD) versus non-SSD on mortality. RR: risk ratio.
This updated analysis is now more in line with the results of prior meta-analyses which also reported no significant impact on mortality. Our revised result is primarily due to decreasing the weight associated with the study by Damas et al. [2] (original weight: 31.0%, corrected weight: 20.7%). In an updated sensitivity analysis, the results remained consistent in all subgroups for the incidence of VAP and mortality.
The discrepancy between SSD's potentially favourable impact on VAP and lack of a clear association with shorter duration of mechanical ventilation, ICU length-of-stay, or lower mortality bears further evaluation. The discrepancy could be due to limited power. It may also reflect the subjectiveness of VAP diagnosis: subconscious bias may account for lower VAP rates in the intervention arms of some studies, particularly unblinded investigations.
SSD is currently recommended in several VAP prevention guidelines [4–6], but this was due in part to prior analyses suggesting a favourable impact on duration of mechanical ventilation and other more objective outcomes. Our updated analysis suggests that SSD may lower perceived VAP rates, but will have a limited impact on other outcomes. Our study therefore provides important context to help hospitals prioritise between different prevention options to improve outcomes for mechanically ventilated patients.
Footnotes
Provenance: Submitted article, peer reviewed.
Conflict of interest: D.P. Pozuelo-Carrascosa has nothing to disclose.
Conflict of interest: M. Klompas has nothing to disclose.
Conflict of interest: C. Alvarez-Bueno has nothing to disclose.
Conflict of interest: J.M. Añón has nothing to disclose.
Conflict of interest: V. Martínez-Vizcaíno has nothing to disclose.
Conflict of interest: I. Cavero-Redondo has nothing to disclose.
Conflict of interest: Á. Herráiz-Adillo has nothing to disclose.
- Received January 24, 2022.
- Accepted February 7, 2022.
- Copyright ©The authors 2022
This version is distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0. For commercial reproduction rights and permissions contact permissions{at}ersnet.org










