





Abstract
Recently, “Technical standards for respiratory oscillometry” was published, which reviewed the physiological basis of oscillometric measures and detailed the technical factors related to equipment and test performance, quality assurance and reporting of results. Here we present a review of the clinical significance and applications of oscillometry. We briefly review the physiological principles of oscillometry and the basics of oscillometry interpretation, and then describe what is currently known about oscillometry in its role as a sensitive measure of airway resistance, bronchodilator responsiveness and bronchial challenge testing, and response to medical therapy, particularly in asthma and COPD. The technique may have unique advantages in situations where spirometry and other lung function tests are not suitable, such as in infants, neuromuscular disease, sleep apnoea and critical care. Other potential applications include detection of bronchiolitis obliterans, vocal cord dysfunction and the effects of environmental exposures. However, despite great promise as a useful clinical tool, we identify a number of areas in which more evidence of clinical utility is needed before oscillometry becomes routinely used for diagnosing or monitoring respiratory disease.
Abstract
This paper provides a current review of the interpretation, clinical significance and application of oscillometry in respiratory medicine, with special emphasis on limitations of evidence and suggestions for future research. https://bit.ly/3GQPViA
Introduction
The mechanical properties of the lungs are disrupted in many disease states and exposures and contribute to major respiratory symptoms such as dyspnoea. Both the clinical management and our understanding of respiratory disease have benefitted from widely available tests like spirometry and the measurement of absolute lung volumes and gas transfer. However, these measurements require significant patient co-operation and a willingness to undertake maximal respiratory efforts. Oscillometry is a noninvasive method for measuring the mechanical properties of the respiratory system, which can enhance our understanding and management of lung disease [1]. Recently, the European Respiratory Journal published “Technical standards for respiratory oscillometry” [2], which reviewed the physiological basis of oscillometric measures and detailed the technical factors related to standardisation of equipment and test performance, quality assurance and reporting of results. Here we provide a review of the clinical significance and applications of oscillometry. We briefly review the physiological principles of oscillometric measurements and the basics of oscillometry interpretation, highlight potential clinical applications, and identify future work required for oscillometry to become routinely used in clinical practice.
The physiology and performance of oscillometry
Oscillometry measures the mechanical impedance of the respiratory system (Zrs), representing the resistive and reactive forces that must be overcome to drive an oscillating flow signal into the respiratory system. The forces arise in the respiratory system from 1) the resistance of the airways and tissues to flow (Rrs), 2) the elastance (stiffness) of the lung parenchyma and chest wall in response to changes in volume (encompassed in reactance, Xrs), and 3) the inertance of accelerating gas in the airways (Irs). Zrs has generally been reported from a single frequency or over the frequency range of 5–40 Hz as an average across the whole breathing cycle (i.e. both inspiration and expiration). It has also been reported separately during the inspiratory and expiratory phases. These concepts and how they are measured by oscillometry are described in detail in the technical document. We provide a brief summary of these details in table 1, figure 1 and the supplementary material.
Summary of oscillometric parameters with a focus on the medium frequency range likely to be used in clinical practice (5–40 Hz)

{kind=link}
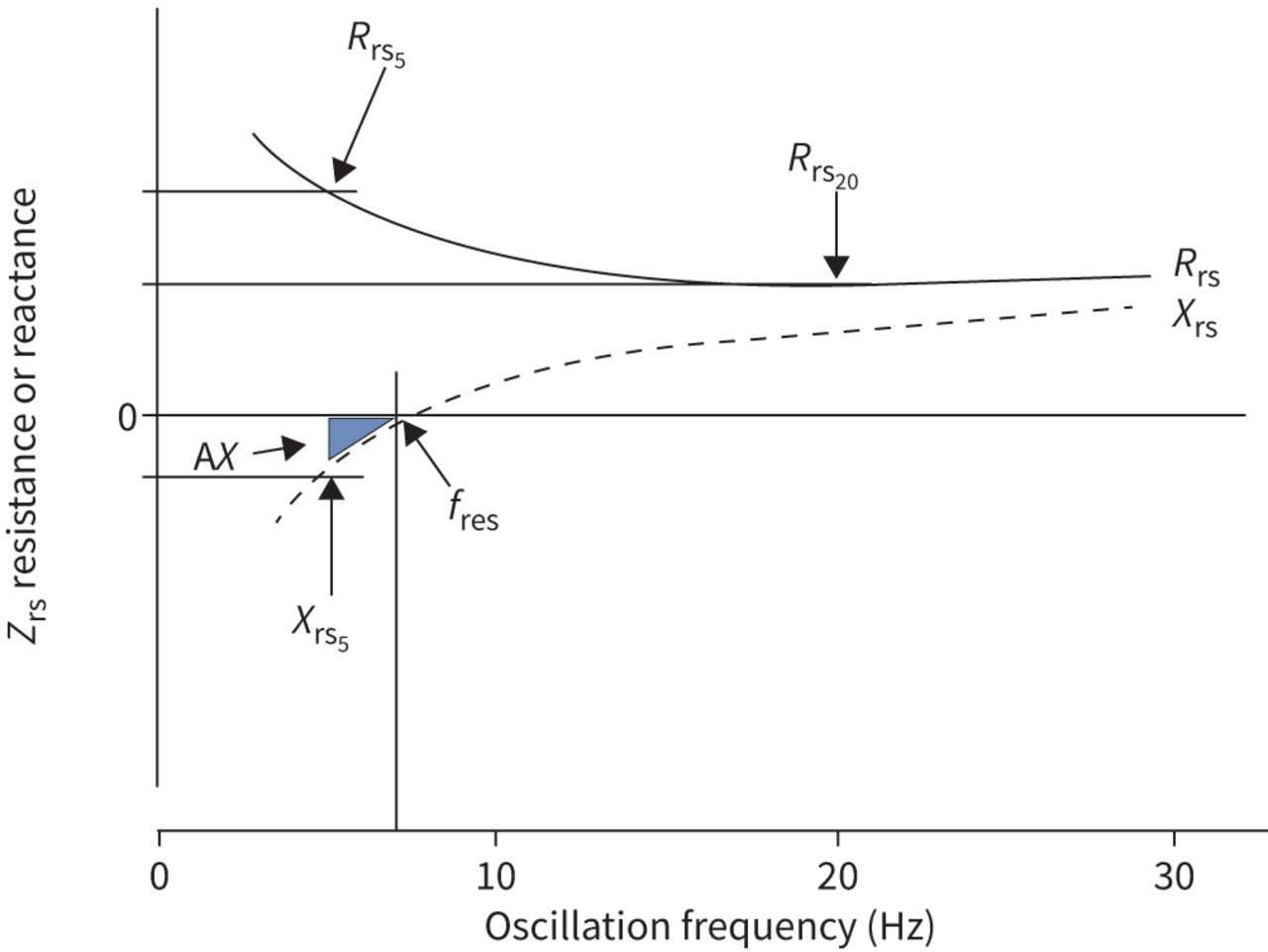
Impedance spectrum. Respiratory system impedance (Zrs) is plotted against frequency. Zrs is composed of a real component seen by resistance (Rrs) and an imaginary component expressed as reactance (Xrs). Rrs and Xrs at specific frequencies are noted by the frequency at which they are measured (e.g. Rrs5=Rrs at 5 Hz, Rrs20=Rrs at 20 Hz). The point at which Xrs crosses zero is the resonant frequency (fres). Below fres, Xrs is dominated by elastance, and above fres, Xrs is dominated by inertance. An integrated measure of low frequency Xrs is the area inscribed by Xrs and Zrs=0 starting at the lowest frequency up to fres, known as the area of the Xrs curve, AX. The lowest frequency defining AX is shown at 5 Hz, but it may be estimated starting from any frequency. Note that the Zrs spectrum shown is characteristic for a healthy adult. In healthy young children, the values and frequency dependence of Rrs would be relatively increased, Xrs would be more negative and fres would be shifted markedly to the right (resulting in increased AX).
Much of the evidence for clinical utility of oscillometry, including the studies cited in the current document, have been collected using a wide range of equipment, protocols and reporting formats. Although there is increasing availability of commercial oscillometry devices, comparability across devices remains a challenge, especially with regards to differences in the frequency dependence of resistance and reactance at higher-than-normal impedance [3, 4]. As such, the applicability of existing reference equations (supplementary table S1) remains uncertain for abnormal disease states and across different devices and manufacturers. Until this is resolved, comparisons between healthy and diseased cohorts should ideally be made using the same device, and differences in results based on variability in equipment, protocols and reference values should be considered when interpreting data presented in this review. Efforts are currently underway by the Global Lung Function Initiative to gather data from around the world to develop more universal, robust reference equations that take into account specific equipment and protocols.
Additionally, while oscillometry is a simple test to perform in clinic, its interpretation remains a challenge for many. Further aspects need to be better established before oscillometry gains an evidence-based position in clinical practice, as summarised in table 2. Many of these aspects are highlighted in the following sections, but in particular it is important to note that establishing minimal important clinical differences to assess change in lung function over time is a crucial area for future research.
Gaps in knowledge and future needs in defining the clinical applications of oscillometry
Oscillometry during infancy
Lung function measurements during infancy have largely been confined to a few specialist centres due to technical complexity, lack of commercially available equipment, and potential risks associated with the measurement (e.g. requirement for sedation). Additionally, the use of a face mask in infants complicates the interpretation of impedance data, since much of the measured Rrs may be attributed to nasal resistance [5]. To date, there is no evidence that impedance measurements in infants contribute to clinical decision-making. However, oscillometric studies have contributed to the pathophysiological understanding of respiratory disease in infants, particularly those with wheezing disorders, as described in the supplementary material.
Preterm birth and bronchopulmonary dysplasia beyond the neonatal intensive care unit
Emerging evidence suggests that oscillometry is a clinically useful measure of lung function in survivors of very preterm birth. Compared to preschoolers delivered at term, those born prematurely have increased Rrs, more negative Xrs and increased area of reactance (AX) and resonant frequency (fres) [6]. Deficits are even greater in premature babies with bronchopulmonary dysplasia (BPD) [7–9]. Xrs measured in the first week of life has been shown to improve prognostication of respiratory outcome in very preterm infants on noninvasive respiratory support. Recently, Evans et al. [10] showed that while all oscillometric outcomes were abnormal in those born very prematurely, Xrs was particularly sensitive at distinguishing term versus preterm preschoolers, suggesting a role for oscillometry in monitoring preterm lung disease. Deficits in oscillometric outcomes persist up to at least adolescence and correlate with respiratory symptoms [11, 12].
To date, only one study has measured oscillometry longitudinally in this population [13]. Interestingly, Xrs and AX deteriorated over time in those with BPD in parallel with declines in spirometry measures, and were found to decrease faster in those children exposed to environmental tobacco smoke and those with respiratory symptoms. Deterioration in these oscillometry outcomes was not associated with structural lung damage on chest computed tomography (CT) scans. The pathophysiology underpinning increased lung stiffness in this population remains unclear, but may reflect failed alveolarisation, structural damage to the parenchyma or inflammatory changes to the lungs.
Asthma
Oscillometric measurements can distinguish adult asthmatics from healthy controls [14–16], asthmatics with different degrees of airway obstruction [17], and between groups of adults with asthma compared to COPD [15, 18–21]. Oscillometry may be especially helpful in diagnosing asthma in patients with preserved spirometry as a more sensitive indicator of abnormal airway physiology [22]. However, while helpful in adults, the delineation between healthy controls and asthmatics using oscillometry is less clear in preschool-aged children, with several studies showing no difference between groups [23–25]. These conflicting findings may be due to differing diagnostic criteria, disease severity or degree of control in the paediatric populations studied who may have smaller differences between health and disease than adults.
Oscillometric outcomes other than resistance and reactance (such as AX and Rrs5–20) may also be useful in supporting a diagnosis of asthma, predicting future loss of asthma control or monitoring clinical treatment changes. In particular, the term “small airway dysfunction” (SAD) has gained traction. The large ATLANTIS cohort revealed that Rrs5–20, AX and Xrs5 were all strong contributors to SAD, with high prevalence in asthma compared to other physiological measures thought to reflect small airways [26]. However, a limitation of the study is that the definition of SAD relied on a statistical, data-driven approach, rather than an independent measure. It also is important to realise that no measures are specific for SAD, including Rrs5–20, which is sensitive to heterogeneouis peripheral airway narrowing, but can also be affected by heterogeneity in the central airways and upper airway shunt (table 1). Furthermore, these relative contributions are likely dependent on disease. We urge caution in the strict interpretation of Rrs5–20 as relating solely to small airways disease, especially when measured using devices that are known to be associated with enhanced frequency dependence of resistance [3, 27–29]. The clinical significance of Rrs5–20 continues to be evaluated in terms of its mechanism [30, 31], prevalence [32] and correlations with measures of severity and control in both children and adults [26, 33, 34].
In addition, oscillometry has provided novel insights into the pathophysiology of asthma via the effects of lung volume on oscillatory mechanics, as well as short- and long-term variations in mechanics over time. These topics are further addressed in the supplementary material. These variations may be a marker of instability, and potentially useful to detect exacerbations or loss of control, particularly in a home telemonitoring setting [35]. Intrabreath changes in oscillometry parameters may also provide additional information beyond conventional parameters: in preschoolers it improved detection of acute obstruction and recurrent wheezers from healthy controls [36], while in adults with severe asthma it distinguished those with poor control from those with good control [37]. While oscillometry measures are generally altered in asthmatics at the population level, oscillometry is arguably of most benefit in clinical practice for the diagnosis of asthma (via bronchodilation or bronchoprovocation) and monitoring response to intervention, as discussed in the following sections.
Bronchodilator response testing
As discussed in the recent technical standards [2], cut-offs indicating a significant bronchodilator response (BDR) using oscillometric indices are reported in healthy adults and children (i.e. 40% decrease in Rrs at 5 Hz, 50% increase in Xrs at 5 Hz and 80% decrease in AX relative to baseline) (supplementary table S2) [2]. Recent work has shown results for BDR in adults [38, 39] that are similar to published data using different instruments [4], suggesting that BDR in oscillometry appears to be robust to different devices and populations. Nevertheless, given the diversity of age ranges, equipment and protocols, further work is still needed to best define a BDR, its significance relative to important patient outcomes and consistency of response over time.
Several studies have shown that a BDR based on oscillometric parameters is better than one based on forced expiratory volume in 1 s (FEV1) at differentiating asthmatic from healthy children [40–42]. However, data relating to BDR in children with “early life” wheeze (i.e. no formal diagnosis of asthma) are less clear, with some studies reporting no differences in BDR between wheezy and non-wheezy preschoolers [43]. In adults, bronchodilation was identified more often using oscillometry than spirometry, and in one study changes in Xrs and AX (but not Rrs) correlated with spirometric responses and identified more subjects with poor asthma control compared to spirometry [44]. Other studies have shown that BDR assessed with oscillometry correlates with poor asthma control [14, 45].
Bronchial challenge testing
Oscillometry can also be used as an alternative to spirometry for conducting bronchial challenges in adults [46–58] and children [59–65]. A summary of studies to date attempting to define airway hyperresponsiveness (AHR) based on oscillometry is shown in supplementary table S3. Results vary widely, ranging from a 20 to 50% increase in Rrs5 and a 20–80% decrease in Xrs5. Provocation studies in children are feasible in patients as young as 3 years old using oscillometry [59, 61]. However, conclusive data indicating which outcome measures and threshold values best reflect a positive bronchial challenge test are currently lacking in this age group. The main advantage of oscillometry for bronchial challenge testing is increased sensitivity of detecting bronchoconstriction, which might shorten the test and reduce the cumulative dose of the agent. However, there may be underestimation of the response occurring in the lungs in children during a challenge due to loss of the oscillatory flow into the upper and large airways, known as upper airway shunt [66]. More information about upper airway shunt is found in the supplementary material.
Deep breaths (i.e. inflation to total lung capacity (TLC)) during spirometry testing, or with some inhalation agents, potentially affect diagnosis, given both the bronchoprotective and bronchodilator effect of deep inhalation in health and in asthma [67–69]. Consequently, oscillometry may be more sensitive than spirometry for detecting AHR in mild asthmatic patients, given their maintained, albeit reduced, response to a deep breath, resulting in a lower provocative dose of methacholine [47, 70] and therefore a shorter testing protocol. However, since avoiding deep breaths may result in AHR even in healthy individuals [71], oscillometry may be less sensitive than spirometry in distinguishing healthy from asthmatic individuals. Of note, patients may prfer oscillometry over spirometry during bronchial challenge testing because they do not have to repeatedly take the deep breaths needed to perform spirometry.
AHR detected by oscillometry is repeatable [47, 49, 61, 72] and correlates with responsiveness based on FEV1 [73], but the correlations of spirometry and oscillometry are inconsistent. There is wide variability across studies, which may be explained by differences in methodology and study populations. However, it appears that oscillometric indices may provide additional information to spirometry. For example, some subjects report symptoms during bronchial challenge without accompanying changes in FEV1, which may be related to the effects of deep inhalation mitigating changes in FEV1; however, concomitant changes in Rrs and AX suggest there is narrowing and/or closure of small airways [74, 75] not detected by spirometry. In summary, oscillometry is a useful tool to detect airway narrowing before spirometry during bronchial challenge testing, but the correlations and thresholds of response are variable, and further studies are needed to determine if oscillometry indices are more clinically relevant than spirometry.
Treatment responses in asthma
In addition to treatment with bronchodilators, differences in Rrs and Xrs in response to different inhaled corticosteroids (ICS) [76, 77], montelukast [78], ICS/long acting β2-agonist (LABA) formulations [79], and ICS versus ICS/LABA [80] have been demonstrated. In general, Rrs, Xrs and AX are more sensitive than spirometry [81]. Recent work has shown that oscillometry and other parameters related to peripheral airway function can be correlated with an improvement in symptoms for patients with poorly controlled asthma receiving ICS/LABA therapy [82]. One study has attempted to determine whether oscillometry could distinguish any benefit of small versus large particle size ICS therapy based on peripheral versus central airway obstruction, respectively; however, this study only looked at the differential treatment effect on symptoms, not oscillometry, and used an arbitrary oscillometric definition of peripheral airway function [83]. Oscillometric indices are also sensitive to improvements in asthma in response to mepolizumab therapy [84]. These findings suggest an important role of oscillometry in identifying and monitoring treatment responses in asthma, complementary to traditional spirometry.
Thus, in asthma, individual oscillometry studies have demonstrated physiological correlations of specific indices with symptoms, imaging, spirometry, changes in response to bronchodilators, bronchial challenges and treatment, and prediction of treatment response. What needs to follow are larger scale trials beyond proof of concept that demonstrate actual clinical utility in terms of improving patient care in asthma, as well as what constitutes a minimal clinically significant difference in oscillometry parameters.
Cystic fibrosis
A number of studies in children with cystic fibrosis (CF) reveal normal oscillometric indices [85–87], with only one study of preschool children with CF reporting abnormal values [88]. Associations between oscillometric indices and other clinical parameters in children with CF are variable [25, 86, 88–92]. There are limited data on the use of oscillometry in adults with CF; however, by one report, resistance and reactance are abnormal in adults with CF and correlate with other measures of lung function [93]. Therefore, the clinical utility of oscillometry in CF remains uncertain, particularly when other clinical tests have shown superior ability to detect early CF lung disease and successfully monitor improvement in lung function with intervention.
COPD
Oscillometry may play an important role in the early detection of the adverse effects of smoking before COPD is diagnosed [94]. Several studies have found a high prevalence of abnormal Zrs in smokers with normal spirometry, mainly in Rrs and Xrs near 5 Hz [95–98], with up to 60% of smokers with normal spirometry (FEV1/forced vital capacity (FVC)>0.70) having some abnormality on oscillometry. Smokers also have greater prevalence of significant BDR compared to nonsmokers [38]. The clinical significance of these findings still needs to be determined by pathologic correlations and prospective clinical studies to establish relevance and utility.
Patients with COPD have significantly higher Rrs and more negative Xrs values than healthy people [99], changes that are proportional to the degree of airway obstruction [100]. Empirical studies demonstrate that Xrs is related to the degree of gas trapping and hyperinflation in the lungs and reflects the amount of communicating lung volume [101]. Xrs and fres relate better to FEV1, and measures of hyperinflation, i.e. inspiratory capacity/TLC and residual volume/TLC ratios, than do resistance measurements [102, 103]. Magnetic resonance imaging-derived measurements of abnormal gas mixing correlate best with Rrs5–19 and AX in COPD patients [104]. Recent work with parametric response mapping by CT has demonstrated strong correlations with oscillometry-derived Rrs5–19 in patients with COPD [105], which is presumed to reflect small airways disease (but may also reflect large airway heterogeneity). A similar finding has been shown using endobronchial optical coherency tomography, which demonstrated that Rrs5–20 correlated with small airways pathology in heavy smokers and patients with COPD [106]. Oscillometric parameters likely related to gas trapping (i.e. Xrs ) in patients with COPD correlated with changes in exercise capacity following completion of pulmonary rehabilitation [107]. Oscillometry may also help in the categorisation of COPD severity [108].
As in asthma, oscillometry parameters are sensitive to treatment in patients with COPD. For example, Xrs near 5 Hz rather than Rrs appears to be more sensitive to bronchodilators [109–113] or ICS/LABA combination treatment [114], or recovery from exacerbations [102, 115–117]. The magnitude of the BDR depends on the disease stage. In the earlier stages of COPD, improvements in oscillometric parameters are greater compared to healthy subjects and are related mainly to an increased bronchodilation of the central airways, improvements in ventilation homogeneity based on the slope of the resistive component of Zrs, and total mechanical load [118].
Examination of intrabreath oscillometry has been especially significant in COPD, where it has been used to demonstrate evidence of tidal expiratory flow limitation (EFLT). Reactance and resistance are higher during expiration compared to inspiration in patients with COPD [119–121], reflecting dynamic airway compression and expiratory airflow limitation [122]. The underlying mechanisms of airway collapse during tidal breathing are uncertain. An empirically defined threshold of the difference between inspiratory and expiratory Xrs has been shown to be a sensitive and specific method for detecting EFLT [123, 124]. The inspiratory–expiratory difference in Xrs and its variability over time is also associated with worse dyspnoea [125]. This index is also associated with more rapid deterioration in exercise capacity over time and an increased likelihood of exacerbations irrespective of the degree of spirometric impairment [126, 127]. EFLT during tidal breathing is an important determinant of dynamic hyperinflation and its identification using oscillometry during noninvasive ventilation allows determining the lowest positive end-expiratory pressure (PEEP) able to abolish it. Recent preliminary studies showed that oscillometry can be incorporated in home noninvasive ventilators for abolishing EFLT by continuously tailoring PEEP to varying lung mechanics [128] leading to reduced hypercapnia and ineffective efforts in stable COPD during nocturnal noninvasive ventilation [129]. Currently, some major limitations to the use of intrabreath monitoring of oscillometry are the lack of normative data and standardisation of analysis and reporting of data.
Oscillometry is often thought to be a better reflection of breathing conditions of everyday life than spirometry, as it directly assesses mechanical impediment to airflow during normal breathing, rather than following deep inhalation; this arguably makes it more useful in COPD, where dyspnoea often occurs even at rest, or where severely obstructed patients can have difficulties with forced manoeuvres. It also makes it amenable to home telemonitoring in COPD, in which feasibility and potential clinical utility has been demonstrated [130] (see supplementary material). Furthermore, the deep inspiration required in spirometry has variable effects on airway calibre in COPD, which may affect clinical correlations [131, 132]. Oscillometry has also revealed greater variations in lung function over time [133, 134] and greater bronchodilator responses in COPD than expected from spirometry [38], again shedding light on disease pathogenesis that goes beyond fixed airway obstruction and reversibility in the larger airways.
In summary, oscillometry may aide in earlier detection of smoking-related effects on the lung and adds insight into the pathophysiology of COPD; however, we still need more data to assess how oscillometry relates to clinical phenotypes of COPD (e.g. predominance of emphysema versus bronchitis) and how it will affect clinical management of patients with COPD.
Bronchiolitis obliterans
Because of its sensitivity to small airway disease, oscillometry has been used to study patients with or at risk of bronchiolitis obliterans. In children, post-infectious bronchiolitis obliterans can be detected by greater changes in Xrs compared to spirometry [135]. In adult lung and bone marrow transplant recipients, bronchiolitis obliterans syndrome may be detected earlier by oscillometry than by conventional spirometry [136–138]. The lack of a need for deep inspiration with oscillometry is also beneficial in patients in the acute postoperative lung transplant period.
Obesity
Impedance measured by oscillometry has been well studied in obesity [139–145]. The effects of obesity are most apparent in Xrs, which suggests that there is an increase in heterogeneous airway narrowing and in airway closure in the lung periphery, although increased stiffness of the chest wall can also contribute [146]. By contrast, there are minimal changes in spirometry and typically no changes in FEV1/FVC ratio in obesity, with the exception of very severe obesity (>40 kg·m−2) [147].
In obesity, Rrs is increased, possibly due to reduced operating lung volume [148–150]. However, this is not the whole reason for this increase [140, 144, 151] as pulmonary circulatory congestion and airway oedema occur in obesity [152, 153] and are correlated with the magnitude of abnormality in both Rrs and Xrs [143]. These changes in airway function make interpretation of impedance in obesity difficult when assessing a patient with potential coexisting airway disease. Obese individuals with clinically and physiologically confirmed asthma have a more negative Xrs than obese, non-asthmatic individuals, probably because of enhanced peripheral airway closure [142, 146]. Changes in Rrs and Xrs with obesity and following bariatric surgery are more pronounced in the supine position with oscillometry being more sensitive to weight loss compared with spirometry [142, 146, 154]. The responses to methacholine bronchial challenge in obese subjects are different compared to non-obese subjects, particularly with regard to bronchoprotection [155] and exaggerated decreases in Xrs [139, 141, 155]. These nuanced differences cannot be easily determined with spirometry. Therefore, obesity is associated with a greater response to bronchoconstriction in terms of changes in the respiratory system elastic properties, but the clinical and pathophysiologic significance of these observations is uncertain.
In children, obesity has been found to be associated with a pattern different from that of obese adults (reduced FEV1/FVC with normal or even increased FEV1 and FVC), called “airway dysanapsis” [156]. Oscillometry may help distinguish the effects of obesity or asthma on the cause of a low FEV1/FVC in children due to dysanapsis or airway narrowing [157]. Increased Rrs5–20 and AX were also found in a cross-sectional study on overweight and obese adolescents [158]. Further research is needed to better define the effects of obesity on oscillometric parameters in overweight and obese children. In both adults and children, it remains unclear how oscillometry data in obesity will contribute to clinical diagnosis and management.
Restrictive diseases
The clinical application of oscillometry in restrictive lung disease is less established in comparison to obstructive disease. Most oscillometric studies of restrictive lung diseases have investigated interstitial lung disease (ILD). Although ILD and obstructive lung diseases are clinically distinct, their corresponding Zrs spectra demonstrate similar patterns of abnormalities, perhaps due to the higher airway resistance found at lower lung volume in ILD. For example, a patient with ILD may demonstrate elevated Rrs, enhanced frequency dependence of Rrs, and more negative Xrs at low frequencies consistent with increased elastance [159–162]. Such findings correlate with the severity of the restriction assessed by either TLC or vital capacity and with the severity of radiographic abnormalities [162–165]. Recent work has shown that while oscillometric parameters in both patients with ILD and COPD correlate well with ventilation unevenness and Rrs, correlations were poor with alterations in static compliance due to emphysema or pulmonary fibrosis [166]. The longitudinal change of Zrs measured by oscillometry in ILD has not been studied.
Oscillometry has also been used to study lung function in pulmonary restriction caused by neuromuscular disease. Conventional physiological studies document diminished vital capacity due to both reduced lung compliance and reduced outward pull of the chest wall in children and adults with neuromuscular disease [167, 168]. While it has been suggested that oscillometry may be useful for the evaluation of neuromuscular disease [169], the data are limited. Technical difficulties in establishing an adequate mouth seal in patients with bulbar weakness may limit applicability in this group. However, oscillometry would appear to have a major advantage over spirometry in detecting lung disease in patients with neuromuscular weakness in general because it does not require muscle force to generate the deep inspiration involved in spirometry.
Vocal cord dysfunction
Paradoxical inspiratory adduction of the vocal cords or reduction in subglottal cross-sectional area induces acute symptoms that is often mistaken for (or associated with) asthma [170]. Detection of inspiratory flow limitation is not widely assessed in clinic and is poorly tolerated, particularly in children. Model analysis has indicated the potential of oscillometry for assessing vocal cord dysfunction (VCD) [171, 172]. It is recommended to carefully examine intratidal changes in Zrs for large positive swings during inspiration [173], especially when tidal inspiratory flow limitation may be suspected [174], and to identify markedly positive differences between inspiratory and expiratory Rrs [175]. Owing to expiratory glottal narrowing, these differences are usually negative in control subjects or stable asthmatics and may be enhanced further in acute bronchoconstriction [175–177]. Large case-control studies are necessary to establish the sensitivity and specificity in VCD.
Sleep apnoea
Obstructive sleep apnoea (OSA) is a very prevalent disease in adults, characterised by recurrent upper airway collapse and obstruction, resulting in nocturnal apnoea and hypopnoea. Given that increase in upper airway resistance is a landmark of OSA, oscillometry is particularly suited for detecting such airway obstruction [178] and hence for application in this disease [179, 180]. Initially, oscillometry was applied to help diagnose OSA in awake patients, since increased susceptibility to airway collapse can be detected by measuring changes in Rrs during continuous negative airway pressure [181]. The effect of posture on oscillometric measures is also enhanced in supine patients with OSA compared to supine patients without OSA, increasing the sensitivity of oscillometry in OSA [182]. Although initial data showed that oscillometry was able to distinguish OSA patients from healthy adults [181], its application for simplified diagnosis has not yet been implemented in routine clinical practice. However, oscillometry is useful for monitoring upper airway collapse during sleep [183–185]. Oscillometry also provides insight into how airway resistance is normalised by application of continuous positive airway pressure (CPAP) [186], and how sleep apnoea and asthma may interact to worsen airway obstruction [187]. Further information on the use of oscillometry in the setting of CPAP is found in the supplementary material.
Environmental and occupational exposures
Oscillometry has been used in monitoring and detection of lung function among people exposed to various environmental or occupational irritants or hazards. Firefighters and those exposed to asbestos have been shown to have abnormalities in oscillometry parameters even with normal spirometric indices [188]. Similar findings are seen in symptomatic people exposed to World Trade Center dust during the 9/11 attacks and suggest the detection of distal airway dysfunction even when spirometry is normal [189, 190]. Exposures to specific inhaled contaminants have been shown to result in changes in Zrs that often but not invariably correlate with changes in spirometry; hence, the two measures may be complementary [191]. Oscillometry has the potential to detect changes years after an environmental exposure. For example, infants exposed to poor air quality from a coal mine fire for a 6-week episode when less than 2 years old had worse AX 3 years after the fire [192]. Furthermore, a study in adolescents showed that exposure to air pollution from local traffic during infancy was associated with abnormal oscillometry parameters suggesting distal airways disease, especially in those with asthma [193]. These studies all suggest that oscillometry may be useful for monitoring lung function in occupational settings and in detecting early changes in lung function in association with environmental exposures.
Of unique concern at the time of this writing is the prevention of spreading contaminated aerosols during lung function testing during the current coronavirus disease 2019 pandemic. Although no data are available, oscillometry is thought to be safer than spirometry in this regard, given that deep inhalation and forced exhalation are not required [194].
Critical care
The measurement of Zrs in critically ill patients receiving ventilatory support poses many unique challenges to the clinician, especially regarding technique and safety [195–200], including managing the interface between the oscillometric generator and the patient's airway [201–203], and the influence of the ventilator circuit on the excitation waveform [204–215]. Further details related to the technical issues of applying oscillometry through the ventilatory circuit are discussed in the supplementary material. Despite technical challenges, the use of oscillometry in ventilated and critically ill patients has yielded tremendous information on the mechanical derangements and pathophysiological processes associated with various respiratory diseases [198, 200, 216–220], such as lung derecruitment [221], parenchymal overdistention [222] and EFLT [124, 223, 224]. In the paediatric patients, oscillometry may be useful for monitoring the effects of positional changes and adjustment of PEEP [220, 225–228] and for improving prediction of respiratory outcomes in extremely preterm newborns receiving invasive ventilation [229]. A recent American Thoracic Society/European Respiratory Society workshop report on the evaluation of respiratory function, including oscillometry in the neonatal and paediatric intensive care units, has recently been published [230]. Oscillometry thus has the potential not only to optimise ventilator settings [226, 231–235], but also to enhance our understanding of the immediate impact of various surgical interventions on lung function [204, 205, 216, 236].
Summary and future research
In summary, oscillometry has shown to be of value for the diagnosing lung disease in our youngest patients and throughout life, and monitoring disease progression, acute exacerbations and treatment effects. While many gaps in our understanding are closing, many still need to be filled in order to ensure a smooth transition of oscillometry from a research tool to a reliable, robust, clinical tool (table 2). In undertaking this review of clinical literature using oscillometry, we have identified several areas where more evidence is required before oscillometry may be used routinely in clinical practice. Looking to the future, we envision many opportunities to develop oscillometry for a wide range of clinical applications [1].
Supplementary material
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Supplementary material ERR-0208-2021.SUPPLEMENT
Footnotes
Provenance: Submitted article, peer reviewed.
This article has supplementary material available from err.ersjournals.com
Conflict of interest: D.A. Kaminsky reports personal payments made as faculty speaker for Cardiorespiratory Diagnostics Seminar from MGC Diagnostics, Inc. outside the submitted work. Past Chair of ATS Proficiency Standards for Pulmonary Function Laboratories Committee, unpaid.
Conflict of interest: S.J. Simpson has nothing to disclose.
Conflict of interest: K.I. Berger has nothing to disclose.
Conflict of interest: P. Calverley reports receiving consulting fees paid by Phillips Respironics for advisory work on a novel COPD ventilator. Payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events received from Phillips Respironics, outside the submitted work.
Conflict of interest: P.L. de Melo reports patent 28727 issued.
Conflict of interest: R.J. Dandurand reports grants or contracts paid to the institution from AstraZeneca, Boehringer-Ingelheim, Covis Pharma, Grifols, MGC Diagnostics, Teva Pharma, Thorasys, and Vyaire, outside the submitted work. Speaking payment from Novartis for L'oscillométrie en clinique: qu'ajoute-t-elle aux évaluations pulmonaires?, 18 September 2019, Boehringer-Ingelheim for L'oscillométrie: vieille physiologie avec un avenir brilliant, 17 November 2020, and Latin American Respiratory Physiology Society for Oscillometry in Asthma and COPD: Interpretation Strategies, 14 November 2020, outside the submitted work. Chairman, Oscillometry Harmonisation Study Group, an international committee academic and industry experts working to standardise oscillometry devices, and Chairman, Respiratory Effectiveness Group Technologies Working Group, Cambridge, U.K. (https://www.regresearchnetwork.org).
Conflict of interest: R.L. Dellacà reports royalties or licenses from Restech, Philips and Vyaire. Payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events received from Restech and Philips, outside the submitted work. Support for attending meetings from Philips and Vyaire. Patent issued, owned and licensed from Politecnico di Milano University. Member of the Board of Directors for Restech. Stocks owned for Restech. Free loan of equipment for studies received from Vyaire and Restech.
Conflict of interest: C.S. Farah has nothing to disclose.
Conflict of interest: R. Farré has nothing to disclose.
Conflict of interest: G.L. Hall has nothing to disclose.
Conflict of interest: I. Ioan has nothing to disclose.
Conflict of interest: C.G. Irvin received consulting fees from Medical Graphics Corporation, outside the submitted work.
Conflict of interest: D.W. Kaczka reports support for the present manuscript from University of Iowa. Grants or contracts from Dept of Defence and NIH, outside the submitted work. Consulting fees received from ZOLL Medical, Inc. Payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events received from CHEST, ASME, Medical Society of New Zealand, and Johns Hopkins University, outside the submitted work. US patent 10,675,423 B2 (patent on MFOV technique, inventor) and PCT patent pending, patent on MFOV technique pending. Stock or stock options held for OscillaVent, Inc. Loan of ventilator for other projects from ZOLL Medical Inc.
Conflict of interest: G.G. King reports grants or contracts from Restech Italy, NHMRC, Boehringer Ingelheim, CycloPharm, GlaxoSmithKline, Menarini, MundiPharma, Philanthropic individuals and societies, outside the submitted work. Payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events received from AstraZeneca, Boehringer Ingelheim, Chiesi, Cipla, CycloPharm, GlaxoSmithKline, Menarini, MundiPharma and Novartis, outside the submitted work. Leadership or fiduciary role in other board, society, committee or advocacy group for ERS Technical Standards for Respiratory Oscillometry.
Conflict of interest: H. Kurosawa reports receiving a grant from CHEST Co. Ltd. Royalties or licence for CHEST Co. Ltd. Payment or honoraria for lectures received from CHEST Co. Ltd. Nippon, Boehringer Ingelheim, Novartis, and Teijin Pharma, outside the submitted work.
Conflict of interest: E. Lombardi reports grants or contracts from Restech and Sanofi, outside the submitted work. Payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events received from Angelini, Chiesi, GSK, Novartis and Sanofi, outside the submitted work. Participation on a Data Safety Monitoring Board or Advisory Board for GSK and Novartis.
Conflict of interest: G.N. Maksym reports grants or contracts from National Research Council of Canada, Cyclomedica Inc. Australia, and Lung Association of Nova Scotia, outside the submitted work. Accommodation Expenses received from Thorasys, Thoracic Medical Systems Inc. for attending European Society Meeting 2019. Patents planned, issued or pending for Method and system to acquire oscillometry measurements, owned by Thorasys, Thoracic Medical Systems Inc. Stock or stock options held for Thorasys, Thoracic Medical Systems Inc.
Conflict of interest: F. Marchal has nothing to disclose.
Conflict of interest: E. Oostveen has nothing to disclose.
Conflict of interest: B.W. Oppenheimer has nothing to disclose.
Conflict of interest: P.D. Robinson has nothing to disclose.
Conflict of interest: M. van den Berge reports grants or contracts from GlaxoSmithKline, Novartis, Astra Zeneca, Roche, and Genentech, outside the submitted work.
Conflict of interest: C. Thamrin report grants or contracts from Restech SRL and THORASYS Thoracic. Equipment on loan for research studies from Restech SRL and THORASYS Thoracic, outside the submitted work.
- Received September 11, 2021.
- Accepted October 29, 2021.
- Copyright ©The authors 2022
This version is distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0. For commercial reproduction rights and permissions contact permissions{at}ersnet.org
References











Jump To
- Article
- Abstract
- Abstract
- Introduction
- Oscillometry during infancy
- Preterm birth and bronchopulmonary dysplasia beyond the neonatal intensive care unit
- Asthma
- Cystic fibrosis
- COPD
- Bronchiolitis obliterans
- Obesity
- Restrictive diseases
- Vocal cord dysfunction
- Sleep apnoea
- Environmental and occupational exposures
- Critical care
- Summary and future research
- Supplementary material
- Footnotes
- References
- Figures & Data
- Info & Metrics