





Figures
- FIGURE 1
Flowchart describing study selection. ICS: inhaled corticosteroid.
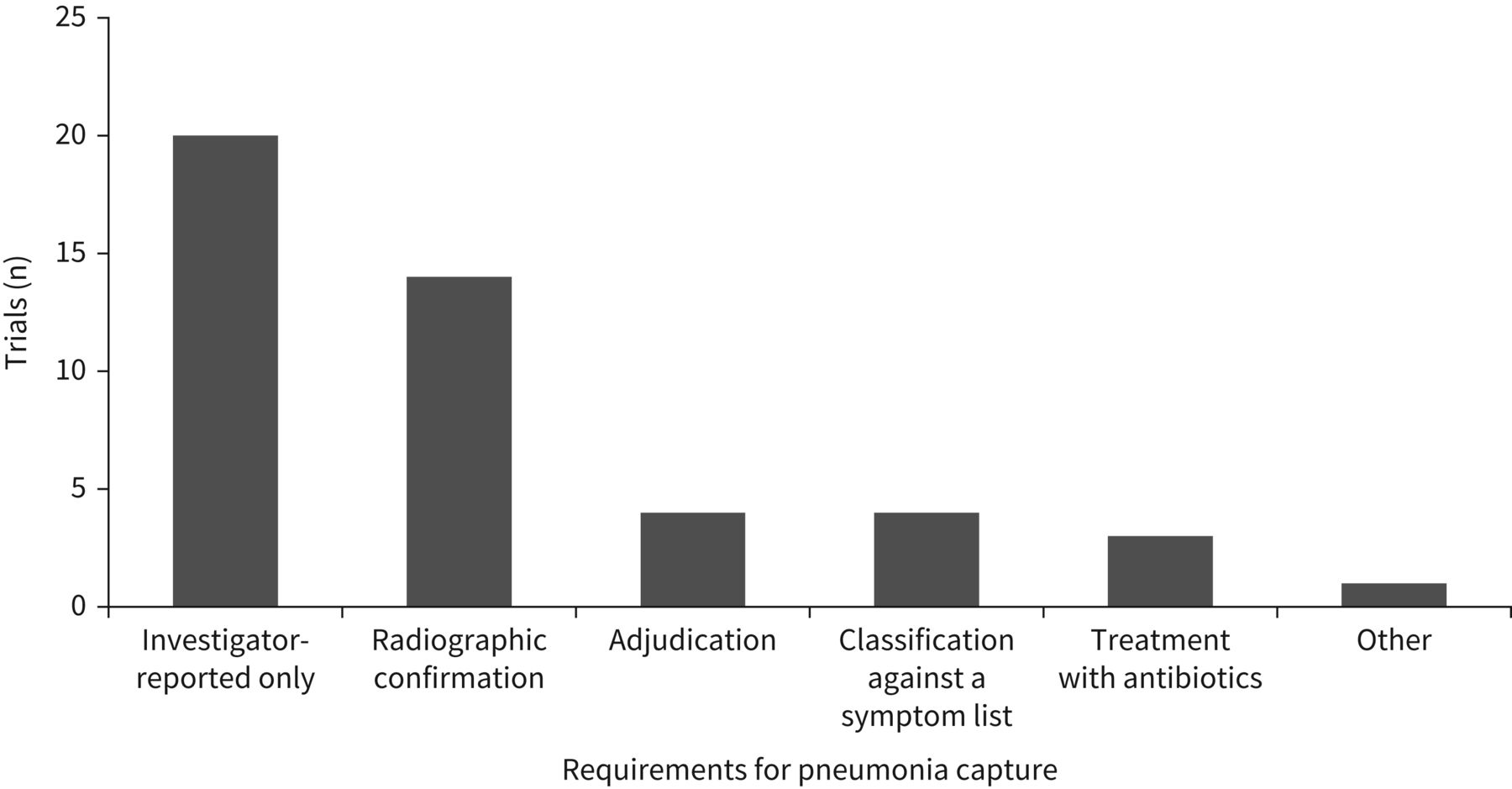
- FIGURE 2
COPD trials by pneumonia capture methodology. Some trials included multiple pneumonia capture methodologies.


{kind=link}
{kind=link}
Tables
- TABLE 1
Pneumonia incidence in identified COPD clinical trials, ordered by treatment comparison and pneumonia capture
Citation Study and study length Study population Pneumonia capture method# Pneumonia incidence, % (n/N)¶ Increased incidence of pneumonia versus comparator arm ICS arm Comparator arm Comparison Fold increase in risk+ Studies comparing ICS/LAMA/LABA triple therapy with non-ICS-containing treatment Pneumonia capture: investigator reporting confirmed by radiographic imaging and independent adjudication Rabe, 2020 [14] ETHOS (52 weeks) Post-bronchodilator FEV1 25–50% pred and ≥1 moderate/severe exacerbation or post-bronchodilator FEV1 50–65% pred and ≥2 moderate or ≥1 severe exacerbation in the year prior to screening
CAT total score ≥10Investigator reported, adjudicated by a clinical end-point independent committee
Radiographic imaging compatible with the diagnosis of pneumonia, ≥2 of a list of clinical signs, symptoms or laboratory findings, and treatment with antibiotics and/or antiviral and/or antifungal agents were also required to support the adjudicationBUD/GLY/FOR 320/18/9.6 µg twice daily: 4.2% (90/2144)
BUD/GLY/FOR 160/18/9.6 µg twice daily: 3.5% (75/2124)
BUD/FOR 320/9.6 µg twice daily: 4.5% (96/2136)GLY/FOR 18/9.6 µg twice daily: 2.3% (48/2125) BUD/GLY/FOR 320/18/9.6 µg versus GLY/FOR 1.9 BUD/GLY/FOR 160/18/9.6 µg versus GLY/FOR 1.6 BUD/FOR versus GLY/FOR 2.0 Ferguson, 2018 [26] KRONOS (24 weeks) Post-bronchodilator FEV1 ≥25% and <80% pred
CAT total score ≥10Investigator reported, adjudicated by an independent committee
Radiographic imaging compatible with the diagnosis of pneumonia, ≥2 of a list of clinical signs, symptoms or laboratory findings, and treatment with antibiotics and/or antiviral and/or antifungal agents were also requiredBUD/GLY/FOR 320/18/9.6 μg twice daily via MDI: 1.9% (12/639)
BUD/FOR 320/9.6 μg twice daily via MDI: 1.9% (6/314)
BUD/FOR 400/12 µg twice daily via DPI: 1.3% (4/318)GLY/FOR 18/9.6 μg twice daily via MDI: 1.6% (10/625) BUD/GLY/FOR versus GLY/FOR 1.2 BUD/FOR 320/9.6 µg via MDI versus GLY/FOR 1.2 BUD/FOR 400/12 µg via DPI versus GLY/FOR 0.8 Pneumonia capture: investigator reporting confirmed by radiographic imaging Chapman, 2018 [27] SUNSET (26 weeks) Post-bronchodilator FEV1 ≥40% and <80% pred
≤1 moderate/severe exacerbation in the year prior to screeningInvestigator reported
Radiographic imaging was required to confirm the diagnosis of pneumoniaTIO 18 µg once daily plus SAL/FP 50/500 µg twice daily: 1.7% (9/526) IND/GLY 110/50 µg once daily: 1.1% (6/527) TIO+SAL/FP versus IND/GLY 1.5 Lipson, 2018 [13] IMPACT (52 weeks) Post-bronchodilator FEV1 <50% pred with ≥1 moderate/severe exacerbation in the year prior to screening, or post-bronchodilator FEV1 50–80% pred and ≥2 moderate or ≥1 severe exacerbation in the year prior to screening
CAT total score ≥10Investigator reported
Radiographic imaging was required to confirm the diagnosis of pneumoniaFF/UMEC/VI 100/62.5/25 µg once daily: 7.6% (317/4151)
FF/VI 100/25 µg once daily: 7.1% (292/4134)UMEC/VI 62.5/25 µg once daily: 4.7% (97/2070) FF/UMEC/VI versus UMEC/VI 1.6 FF/VI versus UMEC/VI 1.5 Magnussen, 2014 [28] WISDOM (52 weeks) Post-bronchodilator FEV1 <50% pred
≥1 exacerbation in the year prior to screeningInvestigator reported
Radiographic imaging was requested when pneumonia was suspectedFP/SAL/TIO (500 µg twice daily/50 µg twice daily/18 µg once daily): 5.8% (72/1243) SAL/TIO (50 µg twice daily/18 µg once daily): 5.5% (68/1242) FP/SAL/TIO versus SAL/TIO 1.1 Pneumonia capture: investigator reporting Papi, 2018 [12] TRIBUTE (52 weeks) Post-bronchodilator FEV1 <50% pred
≥1 moderate/severe exacerbation in the year prior to screening
CAT total score ≥10Investigator reported BDP/FOR/GLY 87/5/9 µg twice daily: 3.7% (28/764) IND/GLY 85/43 µg: 3.6% (27/768) BDP/FOR/GLY versus IND/GLY 1.0 Vestbo, 2017 [29] TRINITY (52 weeks) Post-bronchodilator FEV1 <50% pred
≥1 moderate/severe exacerbation in the year prior to screening
CAT total score ≥10Investigator reported BDP/FOR/GLY 100/6/12.5 µg (2 actuations twice daily): 2.6% (28/1077)
BDP/FOR 100/6 µg (2 actuations twice daily)+TIO 18 µg (1 actuation once daily): 2.2% (12/537)TIO 18 µg once daily: 1.8% (19/1076) BDP/FOR/GLY versus TIO 1.5 BDP/FOR+TIO versus TIO 1.3 Jung, 2012 [30] (24 weeks) Post-bronchodilator FEV1 <65% pred Investigator reported TIO 18 µg once daily+FP/SAL 250/50 µg twice daily: 0.9% (2/223) TIO 18 µg once daily: 0.9% (2/232) TIO+FP/SAL versus TIO 1.0 Studies comparing ICS/LABA dual therapy with non-ICS-containing treatment Pneumonia capture: investigator reporting and independent adjudication with/without confirmation by radiographic imaging Hanania, 2020 [31] SOPHOS (52 weeks) Post-bronchodilator FEV1 ≥25% and <80% pred
≥1 moderate/severe exacerbation in the year prior to screening
CAT total score ≥10Investigator reported, adjudicated by an independent committee BUD/FOR 320/10 µg twice daily: 1.6% (10/619)
BUD/FOR 160/10 µg twice daily: 2.4% (15/617)FOR 10 µg twice daily: 2.3% (14/607) BUD/FOR 320/10 µg versus FOR
BUD/FOR 160/10 µg versus FOR0.7
1.1Ferguson, 2018 [32] TELOS (24 weeks) Post-bronchodilator FEV1 <80% pred
CAT total score ≥10Investigator reported, adjudicated by an independent committee
Radiographic imaging compatible with the diagnosis of pneumonia, ≥2 of a list of clinical signs, symptoms or laboratory findings, and treatment with antibiotics and/or antiviral and/or antifungal agents were also requiredBUD/FOR 320/10 μg twice daily via MDI: 0.8% (5/655)
BUD/FOR 160/10 μg twice daily via MDI: 1.1% (7/637)
BUD 320 µg twice daily via MDI: 0.5% (1/206)
BUD/FOR 400/12 µg twice daily via DPI: 1.4% (3/219)FOR 10 µg twice daily via MDI: 1.4% (9/644) BUD/FOR 320/10 μg versus FOR 0.5 BUD/FOR 160/10 μg versus FOR 0.8 BUD versus FOR 0.3 BUD/FOR 400/12 µg via DPI versus FOR 1.0 Pneumonia capture: investigator reporting confirmed by radiographic imaging Ferguson, 2017 [33] RISE (26 weeks) Post-bronchodilator FEV1 ≤70% pred
≥1 moderate/severe exacerbation in the year prior to screening
mMRC dyspnoea score ≥2Investigator reported
Radiographic imaging compatible with the diagnosis of pneumonia and ≥2 of a list of clinical signs, symptoms or laboratory findings were also requiredBUD/FOR 320/9 µg twice daily: 0.5% (3/605) FOR DPI 9 µg twice daily: 1.0% (6/613) BUD/FOR versus FOR 0.5 Papi, 2017 [24] EFFECT (52 weeks) Post-bronchodilator FEV1 ≤50% pred
≥1 moderate/severe exacerbation in the year prior to screeningInvestigator reported
Radiologically and/or clinically confirmed per British Thoracic Society criteriaFP/FOR 500/20 μg twice daily: 2.9% (17/587)
FP/FOR 250/10 μg twice daily: 3.9% (23/588)FOR 12 µg twice daily: 1.9% (11/590) FP/FOR 500/20 μg versus FOR 1.6 FP/FOR 250/10 μg versus FOR 2.1 Wedzicha, 2016 [34] FLAME (52 weeks) Post-bronchodilator FEV1 ≥25 to <60% pred
≥1 moderate/severe exacerbation in the year prior to screening
mMRC dyspnoea score ≥2Investigator reported
Radiographic imaging was requiredFP/SAL 500/50 µg twice daily: 4.8% (80/1680) IND/GLY 110/50 µg once daily: 3.2% (53/1678) FP/SAL versus IND/GLY 1.5 Ohar, 2014 [35] NCT01110200 (26 weeks) Post-bronchodilator FEV1 <70% pred
Recent exacerbation (≤14 days)Investigator reported
Radiographic imaging was requiredFP/SAL 250/50 µg twice daily: 4.1% (13/314) SAL 50 µg twice daily: 3.1% (10/325) FP/SAL versus SAL 1.3 Vogelmeier, 2013 [36] ILLUMINATE (26 weeks) Post-bronchodilator FEV1 40–80% pred
0 moderate/severe exacerbations in the year prior to screeningInvestigator reported
Radiographic imaging was requiredFP/SAL 500/50 µg twice daily: 1.5% (4/264) IND/GLY 110/50 µg once daily: 0 (0/258) Anzueto, 2009 [10] NCT00115492 (52 weeks) Post-bronchodilator FEV1 ≤50% pred
≥1 moderate/severe exacerbation in the year prior to screeningInvestigator reported
Radiographic imaging was requiredFP/SAL 250/50 µg twice daily: 6.6% (26/394) SAL 50 µg twice daily: 2.5% (10/403) FP/SAL versus SAL 2.7 Pneumonia capture: investigator reporting Suissa, 2018 [37] Up to 1-year follow-up Cohort of patients aged ≥55 years with COPD initiating treatment with a LAMA or ICS/LABA during 2002–2015 from the UK's Clinical Practice Research Datalink Hospital admissions due to severe pneumonia (according to diagnostic codes) ICS/LABA: 3.1% (380/12 366) LAMA: 2.3% (279/12 366) of patients ICS/LABA versus LAMA 1.4 Vestbo, 2016 [38], Crim, 2017 [39] SUMMIT (event driven, common end date of 3 years) Post-bronchodilator FEV1 ≥50% and ≤70% pred
History or increased risk of cardiovascular disease
mMRC dyspnoea score ≥2Investigator reported FF/VI 100/25 µg once daily: 5.7% (237/4140)
FF 100 µg once daily: 5.5% (228/4157)VI 25 µg once daily: 3.9% (163/4140)
Placebo: 5.2% (214/4131)FF/VI versus VI 1.5 FF versus placebo 1.1 Vestbo, 2016 [40] Salford Lung Study (52 weeks) ≥1 COPD exacerbations in the previous 3 years Investigator reported pneumonia SAEs FF/VI 100/25 µg once daily: 6.7% (94/1396) Usual care: 5.9% (83/1403) FF/VI 100/25 µg versus usual care 1.1 Vogelmeier, 2016 [41] AFFIRM (24 weeks) Post-bronchodilator FEV1 <80% pred
CAT total score ≥10Investigator reported FP/SAL 500/50 µg twice daily: 1.9% (9/466) ACL/FOR 400/12 µg twice daily: 0.6% (3/467) FP/SAL versus ACL/FOR 3.2 Zheng, 2015 [42] NCT01376245 (24 weeks) Asian patients
Post-bronchodilator FEV1 ≤70% pred
mMRC dyspnoea score ≥2Investigator reported FF/VI 50/25 µg: 1.3% (2/160)
FF/VI 100/25 µg: 0.6% (1/161)
FF/VI 200/25 µg: 3.1% (5/160)Placebo: 2.5% (4/162) FF/VI 50/25 µg versus placebo 0.5 FF/VI 100/25 µg versus placebo 0.3 FF/VI 200/25 µg versus placebo 1.3 Zhong, 2015 [43] LANTERN (26 weeks) Post-bronchodilator FEV1 ≥30% and <80% pred
≤1 moderate/severe exacerbation in the year prior to screening
mMRC dyspnoea score ≥2Investigator reported FP/SAL 500/50 µg: 2.7% (10/369) IND/GLY 110/50 µg: 0.8% (3/372) FP/SAL versus IND/GLY 3.4 Rossi, 2014 [44] INSTEAD (26 weeks) GOLD stage II
0 moderate/severe exacerbation in the year prior to screeningInvestigator-reported pneumonia SAEs FP/SAL 500/50 µg twice daily: 0.7% (2/288) IND 150 µg once daily: 0 (0/293) FP/SAL versus IND Wedzicha, 2014 [45] FORWARD (48 weeks) Post-bronchodilator FEV1 ≥30% and <50% pred
≥1 moderate/severe exacerbation in the year prior to screeningInvestigator reported BDP/FOR 200/12 µg twice daily: 3.8% (23/601) FOR 12 µg twice daily: 1.8% (11/596) BDP/FOR versus FOR 2.1 Dransfield, 2013 [46], Crim, 2015 [47] NCT01009463, NCT01017952 (52 weeks) Post-bronchodilator FEV1 <70% pred
≥1 moderate/severe exacerbation in the year prior to screeningInvestigator reported FF/VI 200/25 µg once daily: 6.8% (55/811)
FF/VI 100/25 µg once daily: 6.3% (51/806)
FF/VI 50/25 µg once daily: 5.9% (48/820)VI 25 µg once daily: 3.3% (27/818) FF/VI 50/25 µg versus VI 1.8 FF/VI 100/25 µg versus VI 1.9 FF/VI 200/25 µg versus VI 2.1 Kerwin, 2013 [48] NCT01053988 (24 weeks) Post-bronchodilator FEV1 ≤70% pred
mMRC dyspnoea score ≥2Investigator reported FF/VI 100/25 µg once daily: 2.4% (5/206)
FF/VI 50/25 µg once daily: 1.5% (3/206)
FF 100 µg once daily: 1.9% (4/206)VI 25 µg once daily: 2.4% (5/205)
Placebo: 1.4% (3/207)FF/VI 100/25 µg versus VI 1.0 FF/VI 50/25 µg versus VI 0.6 FF versus placebo 1.3 Martinez, 2013 [49] NCT01054885 (24 weeks) Post-bronchodilator FEV1 ≤70% pred
mMRC dyspnoea score ≥2Investigator reported FF/VI 200/25 µg once daily: 2.0% (4/205)
FF/VI 100/25 µg once daily: 0.5% (1/204)
FF 200 µg once daily: 1.5% (3/203)
FF 100 µg once daily: 1.0% (2/204)VI 25 µg once daily: 1.0% (2/203)
Placebo: 0 (0/205)FF/VI 200/25 µg versus VI 2.0 FF/VI 100/25 µg versus VI 0.5 FF 200 µg versus VI 1.5 FF 100 µg versus VI 1.0 Doherty, 2012 [50] (52 weeks) Post-bronchodilator FEV1 25–60% pred
Symptoms of COPD for ≥24 months prior to enrolmentInvestigator reported MF/FOR 400/10 µg twice daily: 3.1% (7/225)
MF/FOR 200/10 µg twice daily: 1.7% (4/239)
MF 400 µg twice daily: 2.0% (5/253)FOR 10 µg twice daily: 1.6% (4/243)
Placebo: 0.8% (2/236)MF/FOR 400/10 µg versus FOR 1.9 MF/FOR 200/10 µg versus FOR 1.0 MF versus placebo 2.3 Tashkin, 2012 [51] NCT00383435 (52 weeks) Post-bronchodilator FEV1 ≥25% and ≤60% pred
Symptoms of COPD for ≥24 monthsInvestigator reported MF/FOR 400/10 µg twice daily: 1.8% (4/217)
MF/FOR 200/10 µg twice daily: 0.5% (1/207)
MF 400 µg twice daily: 1.0% (2/210)FOR 10 µg twice daily: 1.9% (4/209) MF/FOR 400/10 µg versus FOR 1.0 MF/FOR 200/10 µg versus FOR 0.3 MF versus FOR 0.5 Sharafkhaneh, 2012 [52] NCT00419744 (52 weeks) Pre-bronchodilator FEV1 ≤50% pred
≥1 moderate/severe exacerbation in the year prior to screeningInvestigator reported BUD/FOR 320/9 µg twice daily: 6.4% (26/407)
BUD/FOR 160/9 µg:
4.7% (19/408)FOR 9 µg twice daily: 2.7% (11/403) BUD/FOR 320/9 µg versus FOR 2.3 BUD/FOR 160/9 µg versus FOR 1.7 Calverley, 2010 [53] NCT00476099 (48 weeks) Post-bronchodilator FEV1 30–50% pred
≥1 moderate/severe exacerbation in the year prior to screeningInvestigator reported BDP/FOR 200/12 µg twice daily: 2.2% (5/232)
BUD/FOR 400/12 µg twice daily: 2.9% (7/238)FOR 12 µg twice daily: 0.4% (1/233) BDP/FOR versus FOR 5.0 BUD/FOR versus FOR 6.9 Rennard, 2009 [54] NCT00206167 (52 weeks) Post-bronchodilator FEV1 ≤50% pred
≥1 moderate/severe exacerbation in the year prior to screening
mMRC dyspnoea score ≥2Investigator reported BUD/FOR 320/9 µg twice daily: 4.0% (20/494)
BUD/FOR 160/9 µg twice daily: 3.4% (17/494)FOR 9 µg twice daily: 3.4% (17/495)
Placebo: 5.0% (24/481)BUD/FOR 320/9 µg versus FOR 1.2 BUD/FOR 160/9 µg versus FOR 1.0 Ferguson, 2008 [11] NCT00144911 (52 weeks) Post-bronchodilator FEV1 ≤50% pred
≥1 moderate/severe exacerbation in the year prior to screeningInvestigator reported FP/SAL 250/50 µg twice daily: 7.4% (29/394) SAL 50 µg twice daily: 3.9% (15/388) FP/SAL versus SAL 1.9 Tashkin, 2008 [55] NCT00206154 (26 weeks) Pre-bronchodilator FEV1 ≤50% pred
≥1 moderate/severe exacerbation in the year prior to screening
mMRC dyspnoea score ≥2Investigator reported BUD/FOR 320/9 µg twice daily: 0.4% (1/277)
BUD/FOR 160/9 µg twice daily: 0.7% (2/281)
BUD 320 µg twice daily+FOR 9 µg twice daily: 0.7% (2/287)
BUD 320 µg twice daily: 1.1% (3/275)FOR 9 µg twice daily: 0.4% (1/284)
Placebo: 0.3% (1/300)BUD/FOR 320/9 µg versus FOR 1.0 BUD/FOR 160/9 µg versus FOR 2.0 BUD 320 µg+FOR 9 µg versus FOR 2.0 BUD versus placebo 3.3 Wedzicha, 2008 [56], Calverley, 2011 [57] INSPIRE (2 years) Post-bronchodilator FEV1 <50% pred, mMRC dyspnoea score ≥2, clinical history of exacerbations Investigator reported FP/SAL 500/50 µg twice daily: 7.6% (50/658) TIO 18 µg once daily: 3.6% (24/665) FP/SAL versus TIO 2.1 Calverley, 2007 [58], Crim, 2009 [59] TORCH (3 years) (pneumonia incidences from a post hoc analysis focusing on pneumonia are reported here) Pre-bronchodilator FEV1 <60% pred Investigator reported FP 500 µg twice daily: 14.4% (224/1552)
FP/SAL 500/50 µg twice daily: 16.0% (248/1546)SAL 50 µg twice daily: 10.5% (162/1542)
Placebo: 9.0% (139/1544)FP/SAL versus SAL 1.5 FP versus placebo 1.6 ICS: inhaled corticosteroid; LAMA: long-acting muscarinic antagonist; LABA: long-acting β2-agonist; FEV1: forced expiratory volume in 1 s; CAT: COPD Assessment Test; BUD: budesonide; GLY: glycopyrronium; FOR: formoterol; MDI: metered-dose inhaler; DPI: dry powder inhaler; TIO: tiotropium; SAL: salmeterol; FP: fluticasone propionate; FF: fluticasone furoate; UMEC: umeclidinium; VI: vilanterol; BDP: beclomethasone dipropionate; mMRC: modified Medical Research Council; SAE: serious adverse event; ACL: aclidinium; IND: indacaterol; GOLD: Global Initiative for Chronic Obstructive Lung Disease; MF: mometasone furoate. #: when a study uses different sets of criteria to define pneumonia and reports different pneumonia incidences when using these different criteria, only the pneumonia incidence for the most stringent pneumonia capture method is reported. The corresponding method is summarised in the “pneumonia capture method” column; ¶: N is the total number of patients in the subgroup of interest, n the number of patients with events; +: fold increase calculated as (incidence in treatment arm of interest)/(incidence in comparator arm).
- TABLE 2
Pneumonia incidence determined by clinical end-point committee
Study and treatment group Patients, n Pneumonia events submitted to clinical end-point committee, n (%) Pneumonia events confirmed by clinical end-point committee, n (%) ETHOS [14] BUD/GLY/FOR (160/18/9.6 µg) 2124 100 (4.7) 75 (3.5) BUD/GLY/FOR (320/18/9.6 µg) 2144 115 (5.4) 90 (4.2) BUD/FOR (320/9.6 µg) 2136 118 (5.5) 96 (4.5) GLY/FOR (18/9.6 µg) 2125 66 (3.1) 48 (2.3) KRONOS [26] BUD/GLY/FOR (320/18/9.6 µg; via MDI) 639 16 (2.5) 12 (1.9) BUD/FOR (320/9.6 µg; via MDI) 314 7 (2.2) 6 (1.9) BUD/FOR (400/12 µg; via DPI) 318 6 (1.9) 4 (1.3) GLY/FOR (18/9.6 µg; via MDI) 625 11 (1.8) 10 (1.6) BUD: budesonide; GLY: glycopyrronium; FOR: formoterol; MDI: metered dose inhaler; DPI: dry powder inhaler.
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Supplementary material ERR-0124-2021.SUPPLEMENT











Jump To
- Article
- Abstract
- Abstract
- Introduction
- Methods
- Differences in pneumonia capture and reporting
- Distinguishing between pneumonia and COPD exacerbations
- Differences in study design and population characteristics
- Towards a standardised definition of pneumonia for COPD clinical trials
- Conclusions
- Supplementary material
- Acknowledgements
- Footnotes
- References
- Figures & Data
- Info & Metrics