





Abstract
Interstitial lung diseases (ILDs) are diverse parenchymal pulmonary disorders, primarily characterised by alveolar and interstitial inflammation and/or fibrosis, and sharing pathophysiological similarities. Thus, patients generally harbour common respiratory symptoms, lung function abnormalities and modified exercise adaptation. The most usual and disabling complaint is exertional dyspnoea, frequently responsible for premature exercise interruption. Cardiopulmonary exercise testing (CPET) is increasingly used for the clinical assessment of patients with ILD. This is because exercise performance or dyspnoea on exertion cannot reliably be predicted by resting pulmonary function tests. CPET, therefore, provides an accurate evaluation of functional capacity on an individual basis. CPET can unmask anomalies in the integrated functions of the respiratory, cardiovascular, metabolic, peripheral muscle and neurosensory systems in ILDs. CPET uniquely provides an evaluation of all above aspects and can help clinicians shape ILD patient management. Preliminary evidence suggests that CPET may also generate valuable prognostic information in ILDs and can be used to shed light on the presence of associated pulmonary hypertension. This review aims to provide comprehensive and updated evidence concerning the clinical utility of CPET in ILD patients, with particular focus on the physiological and clinical value of ventilatory efficiency (V˙E/V˙CO2).
Abstract
Ventilatory inefficiency, as defined by an abnormally increased minute ventilation/carbon dioxide production relationship during cardiopulmonary exercise testing, has diagnostic and prognostic implications in the management of ILDs https://bit.ly/3vFnyhq
Introduction
Interstitial lung diseases (ILDs), formerly called diffuse parenchymal lung diseases, are a heterogeneous group of more than 200 rare, non-neoplastic, often chronic disorders. They are primarily characterised by diffuse infiltrates into the lung interstitium. Damage to the lung parenchyma, by various patterns of inflammation and fibrosis, are frequently associated with the involvement of adjacent alveolar epithelium, small distal airways and lung vascular bed, and may result in architectural alterations of the alveolar capillary membrane. Although ILDs regroup distinct pathologies, they share similarities in pathogenesis [1–3]. Thus, patients generally harbour common respiratory symptoms, lung function abnormalities and modified exercise adaptation. The most usual and disabling complaint is exertional dyspnoea, frequently responsible for premature exercise interruption and important decline in quality of life [4].
Pathological features are worsened during exercise in ILDs. Respiratory, cardiovascular and/or peripheral responses to exercise can all be modified, making cardiopulmonary exercise testing (CPET) an essential tool to untangle the relative contribution of each one [5–9]. Amongst numerous useful variables, the assessment of ventilatory efficiency is of prime importance in CPET interpretation. Ventilatory efficiency is mainly characterised by the relationship between the output of metabolically produced carbon dioxide (V˙CO2) and the quantity of ventilation (V˙E) needed to eliminate it. The V˙E/V˙CO2 index is called ventilatory equivalent for CO2. It mathematically and physiologically depends on CO2 arterial partial pressure (PaCO2) and the dead space to tidal volume ratio (VD/VT). It can be measured at rest, at its lowest value (V˙E/V˙CO2 nadir), at the first ventilatory threshold (V˙E/V˙CO2 at VTh, VTh being alternatively called anaerobic threshold) and at peak exercise (peak V˙E/V˙CO2). The slope of the relationship can be calculated by linear regression (V˙E–V˙CO2 slope). Depending on the authors, the slope is computed from exercise initiation to either the second ventilatory threshold (alternatively called ventilatory compensation point, after which the V˙E/V˙CO2 curve steepens) or to peak exercise (on condition that exercise is maximal) [5, 7, 10, 11]. Numerous studies have proven a link between abnormally increased V˙E/V˙CO2 (i.e. ventilatory inefficiency) and dyspnoea, limited exercise performance and/or poorer outcome in various respiratory or cardiocirculatory conditions, such as chronic obstructive pulmonary disease (COPD), cystic fibrosis, pulmonary hypertension and chronic heart failure [12]. Indeed, multiple mechanisms can interact and result in ventilatory inefficiency: increased physiological dead space, pulmonary vasculopathy, ventilation/perfusion (V˙A/Q˙) mismatch, exercise-induced hypoxaemia, increased metabolic demand, inappropriate hyperventilation, deconditioning, elevated ventilatory neural drive, sympathetic overstimulation, elevated chemoreceptor or ergoreceptor sensitivity, and metabolic acidosis [5–7, 13–15].
The current review belongs to the European Respiratory Review series on “The ventilatory efficiency and its clinical and prognostic value in cardiorespiratory disorders” and provides an up-to-date summary of recent advances concerning the clinical utility of CPET in ILD patients, with particular focus on the physiological and clinical value of ventilatory efficiency.
Epidemiology and classification of ILDs
The incidence and prevalence of ILDs depend on the case counting method and the geographical area. Taking ILDs as a whole, incidence is considered to be around 20–30 cases per 100 000 per year and prevalence around 60–80 cases per 100 000 [16, 17]. A French exhaustive study, performed in a multi-ethnic county of Greater Paris, even found a total crude prevalence of 97.9 per 100 000 [18]. Sarcoidosis, idiopathic pulmonary fibrosis (IPF) and ILDs related to connective tissue diseases (CTDs)/vasculitis represent more than one half of all ILD cases, with respective frequencies depending on age, sex and geographical origin.
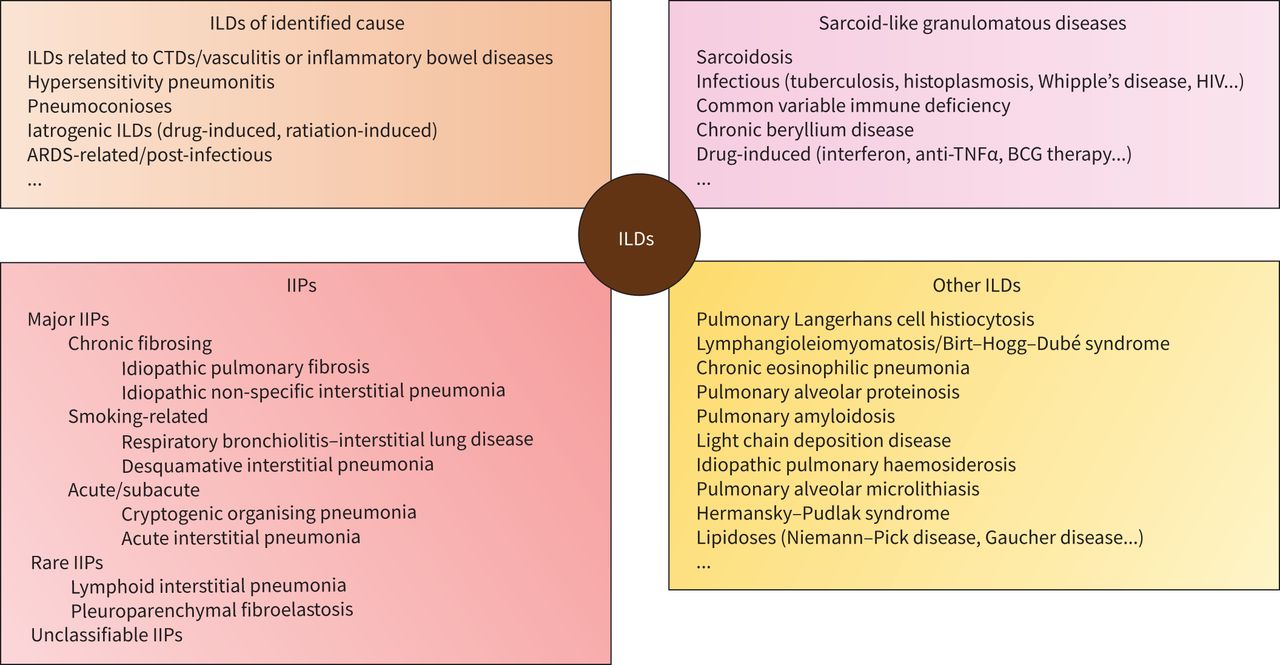
Considerable progress was made in the past decades to better understand ILDs. Harmonised nomenclature and diagnostic criteria were provided by the 2002 international consensus classification [19], later updated in 2013 [20]. ILDs can be separated into four groups: 1) ILDs of known aetiology, e.g. CTDs/vasculitis, hypersensitivity pneumonitis (HP), iatrogenic ILDs, pneumoconioses; 2) idiopathic interstitial pneumonias (IIPs), e.g. IPF, idiopathic non-specific interstitial pneumonia (iNSIP); 3) sarcoidosis and sarcoid-like granulomatous diseases; 4) other forms of ILDs, e.g. pulmonary Langerhans cell histiocytosis (PLCH), lymphangioleiomyomatosis (LAM), chronic eosinophilic pneumonia and pulmonary alveolar proteinosis (figure 1). Multidisciplinary discussion is mandatory in diagnostic decision-making, and high-resolution computed tomography (HRCT) is often the cornerstone examination in the process [21, 22]. For example, although surgical lung biopsy is the gold standard to establish a diagnosis of IPF, it is not required in a patient with high clinical likelihood (>60 years old, exclusion of other known cause of ILD) and suggestive HRCT pattern [22, 23].
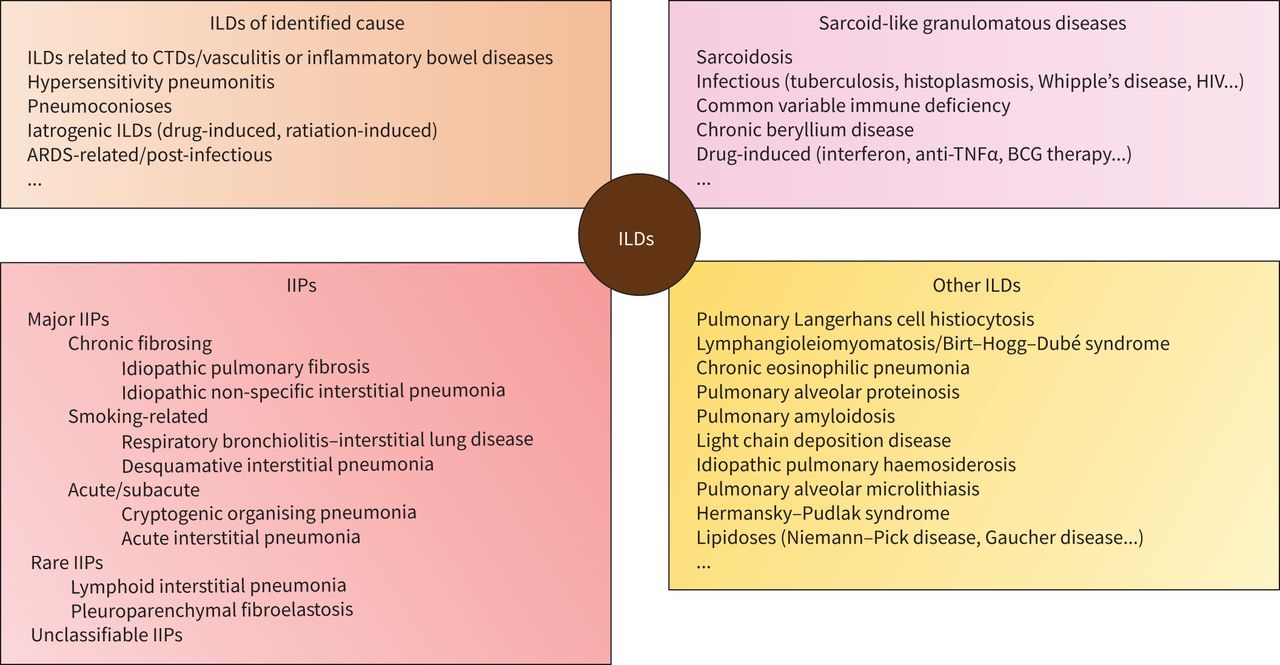
Classification of the main interstitial lung diseases (ILDs). By definition, pulmonary oedema from chronic heart failure, neoplastic diseases (lymphangitis carcinomatosa, lymphoma, lepidic growth adenocarcinoma) and chronic infections (pneumocystosis, miliary tuberculosis) are excluded from ILDs of identified cause. Idiopathic interstitial pneumonias (IIPs) are most often sporadic, but familial cases constitute up to 2–20% of cases. These cases remain classified as IIPs despite the genetic predisposition. In addition to that classification, several rare histologic patterns of ILDs have been described, including acute fibrosing and organising pneumonia (AFOP) and bronchiolocentric patterns of interstitial pneumonia. These rare patterns are not considered as distinct entities of IIPs. The term “non-specific interstitial pneumonia” can apply to a distinct disease classified amongst IIPs (idiopathic non-specific interstitial pneumonia), or a pulmonary histologic pattern that can also be encountered in diverse ILDs of known cause, or even in other IIPs. ARDS: acute respiratory distress syndrome; BCG: bacillus Calmette–Guérin; CTDs: connective tissue diseases; HIV: human immunodeficiency virus; TNFα: tumour necrosis factor alpha.
A complementary categorisation was also proposed, according to patterns of disease behaviour (reversible versus irreversible, stable versus progressive), which can be useful in most types of ILDs, regardless of the precise diagnosis, to adjust therapeutic goal and monitoring strategy, and set pertinent endpoints in clinical trials [20, 24, 25]. For example, IPF is the very prototype of the “progressive fibrosing ILD” pattern, characterised by irreversible and self-sustaining fibrosis, progressive worsening in dyspnoea and lung function, associated with early mortality. But it can also be encountered in other ILDs such as iNSIP, CTD-related ILD, HP, stage IV sarcoidosis, drug-induced ILD, pneumoconiosis, acute respiratory distress syndrome-related ILD and unclassifiable IIP. All of them could benefit from the same treatments [26, 27]. Level of dyspnoea, lung function at baseline or in the later course of the disease, exercise performances and exercise-induced desaturation are all major prognostic factors in ILDs, alongside the extent of fibrosis on HRCT (particularly with a honeycombing pattern) and the presence of precapillary PH [22, 28–31].
Resting pulmonary function tests (PFTs) in ILDs
PFTs are essential to the diagnosis and to assess disease severity, prognosis and response to therapy. They typically show a low diffusion capacity of the lungs for carbon monoxide (DLCO), associated with a restrictive ventilatory defect (RVD) with reduction of total lung capacity (TLC) and vital capacity (VC). Forced expiratory volume in one second (FEV1)/VC ratio is often normal or even increased [19, 32–35]. Pathophysiological mechanisms for DLCO changes in ILDs are almost always intertwined: V˙A/Q˙ mismatch being the main factor, in combination with alveolar capillary membrane thickening, reduction in gas exchange surface due to RVD and/or rarefaction of the pulmonary capillary bed. Therefore, DLCO alteration is generally the first anomaly to be observed, decreasing to a greater extent than other functional variables when expressed as a percentage of reference values. Gas exchange impairment leads to widened alveolar–arterial oxygen pressure difference (P(A-a)O2) and hypoxaemia, first at exercise and ultimately at rest when DLCO has severely declined [32–39]. Abnormal respiration mechanics, with increased lung recoil pressure and decreased lung compliance, are responsible for lung volume reduction. Depending on the criteria used, airway obstruction has been described in 8.8% to 57% of sarcoidosis patients [40–42]. Obstructive ventilatory defect (OVD), as defined by an excessively decreased FEV1/VC ratio, can also occur in other ILDs with particular airway involvement: rheumatoid arthritis, Sjögren's syndrome or inflammatory bowel disease associated ILD, HP, PLCH, LAM, silicosis, chronic eosinophilic pneumonia, respiratory bronchiolitis-ILD and chronic beryllium disease. OVD can occur independently or associated with RVD, such patients with mixed ventilatory defect tend to exhibit relatively preserved TLC and residual volume. In patients with combined pulmonary fibrosis and emphysema, the FEV1/VC ratio is only reduced in cases of major emphysema extent. Despite relatively preserved lung volumes, these patients characteristically present with a severe, out-of-proportion, decrease in DLCO [35, 43].
Exercise pathophysiology and CPET in ILDs
Resting PFTs cannot always predict exercise performance in individual ILD patients [37, 44, 45]. The six-minute walk test and CPET are valuable to assess functional status and detect precocious alteration in gas exchange. CPET is often mandatory for setting the exercise training intensity for pulmonary rehabilitation. CPET also helps to decipher the mechanisms of dyspnoea and exercise limitation of unclear origin, especially when PFTs and transthoracic echocardiogram (TTE) are either normal or both impaired. This is all the more important in ILDs with potential extrapulmonary involvement (sarcoidosis, CTDs) or when deconditioning with peripheral muscle weakness is suspected, which is a frequent situation in chronic lung diseases [5, 46–50]. Moreover, cardiovascular comorbidities are known to be frequent in IPF patients [51–53]. Given the huge variety of reasons for functional impairment, and the numerous modalities of decline, with many potential clinical and therapeutic questions, CPET positioning and timing during the course of ILDs is not unique [5, 47, 50]. Even if the minimal clinically important difference is unclear for CPET variables, repeated assessment is feasible and could be of great help in personalised medical decisions [54], especially as it can identify the mechanisms of improvement or deterioration. Data are scarce on this topic, but serial CPETs were used to assess the benefits of some pharmacological or non-pharmacological interventions, such as pulmonary rehabilitation [55–58].
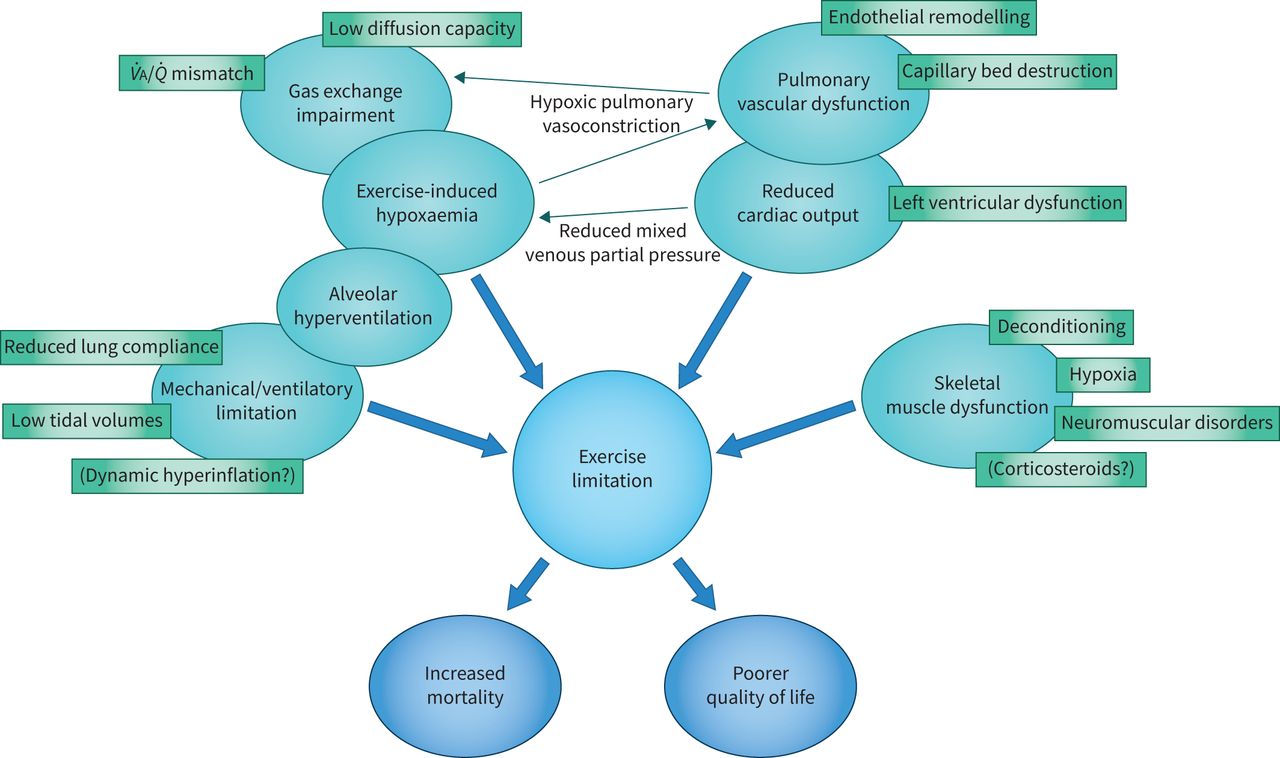
Compared to age- and sex-matched healthy subjects, ILD patients regularly harbour a decrease in maximal O2 uptake (peak V˙O2) and maximal work rate (WR) (table 1) [5, 6, 46–50]. Indeed, various mechanisms can jointly contribute to that limitation, as ILDs induce numerous changes in physiologic and sensory responses to exercise (figure 2) [59–62]. Patients with ILD often hyperventilate at rest and during exercise, as demonstrated by a low PaCO2 [39, 63]. Reduced lung compliance, with increased elastic loading on respiratory muscles and lung elastic recoil, alongside with stimulation of thoracic mechanoreceptors, limits the rise in VT below 50–60% of maximal VC, leading to a characteristic shallow breathing pattern with high respiratory frequency (fR). A low or absent breathing reserve (BR) at peak exercise frequently ensues [59, 60, 64–67]. Although the reduction in VT is an effective strategy to minimise the inspiratory elastic work of breathing during exercise, the compensatory tachypnoea increases VD. Also, impaired alveolar capillary diffusing capacity, low V˙A/Q˙ regions and reduced mixed O2 venous partial pressure (Pv̄O2) lead to exercise-induced hypoxaemia, PaO2 being inversely proportional to WR [37, 39, 59, 61, 68, 69]. Both dynamic restrictive mechanical constraints and hypoxaemia-induced stimulation of peripheral chemoreceptors favour alveolar hyperventilation. In addition to V˙A/Q˙ mismatch, it results in ventilatory inefficiency: high VD/VT ratio (remaining abnormally stable or even increasing in exercising ILD patients) and increased V˙E/V˙CO2 relationship (at any given level of O2 consumption). Increased pulmonary vascular resistance during exercise, from hypoxic pulmonary vasoconstriction and capillary bed remodelling or destruction, also participates in the alteration of ventilatory efficiency by increasing effective VD [39, 59, 61, 67, 68, 70, 71]. Dynamic hyperinflation (DH), i.e. a decrease in inspiratory capacity during exercise, was documented in ILDs involving airways, such as LAM, PLCH and HP [72–75]. Since DH has been demonstrated in patients with pulmonary arterial hypertension (PAH) and chronic thromboembolic pulmonary hypertension [76, 77], it could theoretically be present in patients with ILD and associated PH, but this issue has not yet been investigated. Several of the aforementioned pathophysiological mechanisms may be intertwined in a single individual, and all of them can be responsible for an elevated ventilatory neural drive, at any given WR, largely explaining the level of exertional breathlessness in ILD patients [67, 78–81]. An example of CPET can be found in figure 3. Importantly, cycling frequently underestimates the severity of exercise-related hypoxaemia in ILD patients.
Common cardiopulmonary exercise testing features in patients with interstitial lung disease (ILD) compared to other cardiopulmonary conditions

Mechanisms of exercise limitation in interstitial lung diseases. The combination of increased dead space and alveolar hyperventilation results in an abnormally elevated V˙E/V˙CO2 ratio. Ventilatory inefficiency and impairment of pulmonary gas exchange are key mechanisms of dyspnoea and exercise intolerance in patients with interstitial lung diseases (ILDs). Some ILDs may present with specific neuromuscular disorders (e.g. in sarcoidosis or connective tissue diseases) or heart involvement (e.g. in sarcoidosis or systemic sclerosis). Additionally, associated cardiovascular comorbidities are common (e.g. in idiopathic pulmonary fibrosis). V˙A/Q˙: ventilation/perfusion.
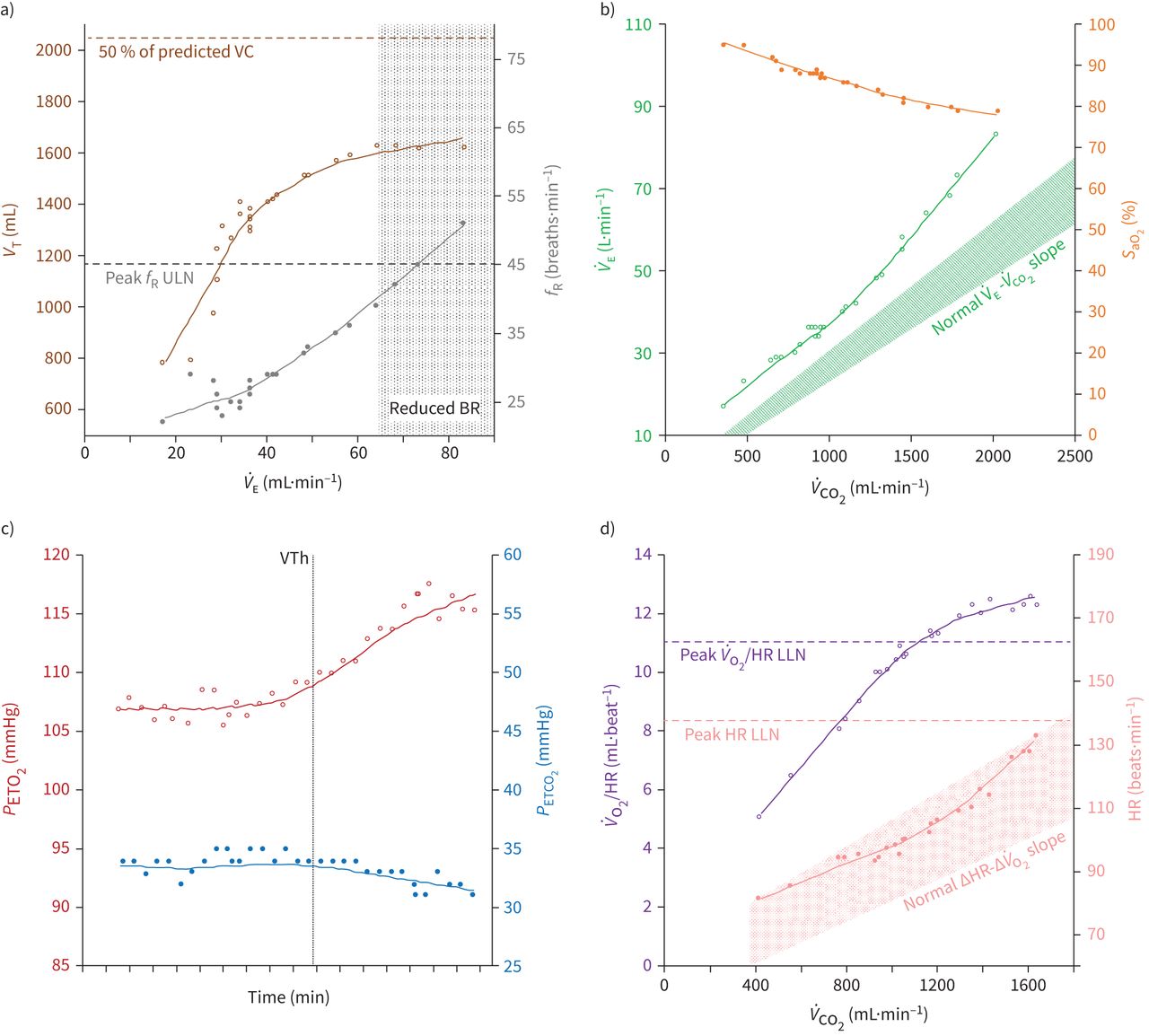
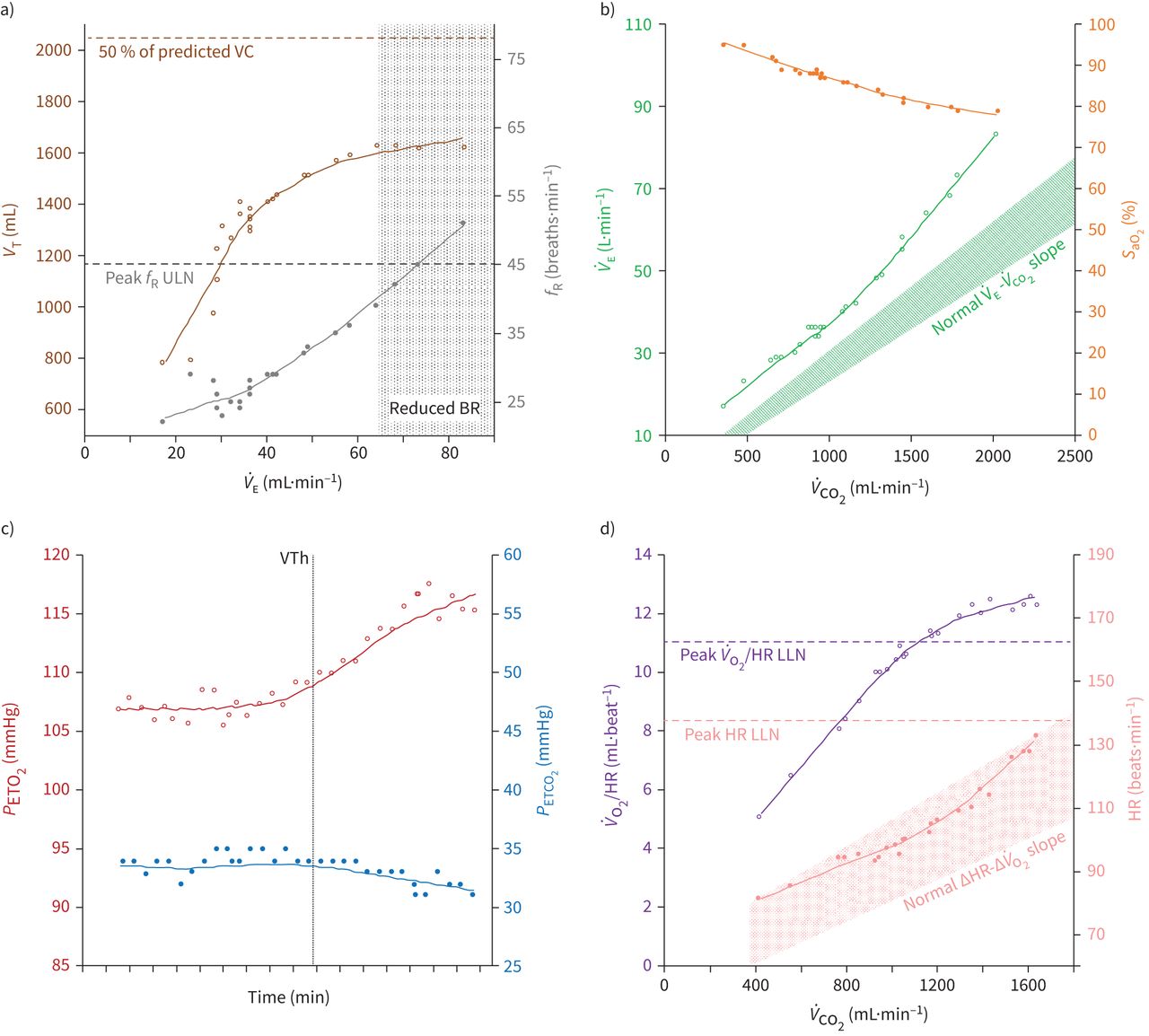
Cardiopulmonary exercise test of a 70-year-old male patient with idiopathic pulmonary fibrosis. Resting pulmonary function tests showed restrictive ventilatory defect (vital capacity=56% of predicted value) and low diffusion capacity for carbon monoxide (DLCO=40%). Peak V˙O2 was mildly reduced (15.6 ml·kg−1·min−1, 78% of predicted value), submaximal heart rate (HR) and null breathing reserve (BR) at peak exercise indicated respiratory limitation. Ventilatory response is shown in panels a) and b); tidal volume (VT) could rise up to 71% of maximal vital capacity (VC), but still with an accelerated respiratory frequency (fR) up to 51 breaths·min−1. Ventilatory inefficiency was documented by a V˙E–V˙CO2 slope value of 40 and a V˙E/V˙CO2 nadir of 37. Oxygen saturation (SaO2) progressively decreased with exercise intensity and peak alveolar–arterial oxygen pressure difference (P(A-a)O2) was 55 mmHg. Hyperventilation resulted in low end-tidal carbon dioxide partial pressure (PETCO2) and high end-tidal oxygen partial pressure (PETO2) (panel c), with increased dead space (resting and peak VD/VT of 0.44 and 0.37, respectively). Theoretical maximal HR was not achieved due to respiratory limitation, though cardiocirculatory response was satisfactory and maximal oxygen pulse was 88% of predicted value (panel d). BR: breathing reserve; DLCO: diffusion capacity of the lung for carbon monoxide; fR: respiratory frequency; HR: heart rate; LLN: lower limit of normal; P(A-a)O2: alveolar–arterial oxygen pressure difference; PETCO2: end-tidal carbon dioxide partial pressure; PETO2: end-tidal oxygen partial pressure; PFTs: pulmonary function tests; SaO2: oxygen saturation; ULN: upper limit of normal; VC: vital capacity; V˙CO2: carbon dioxide output; VD: dead space; V˙E: total ventilation; V˙O2: oxygen uptake; VT: tidal volume; VTh: first ventilatory threshold.
Skeletal muscle dysfunction (SMD) is another important feature contributing to dyspnoea and exercise limitation in patients with various ILDs [82–86]. Not only quadriceps muscle strength, endurance and/or resistance to fatigue are reduced in ILDs compared to healthy individuals, but SMD seems to be more important in IPF than in COPD [87]. Indeed, leg discomfort is commonly recounted by ILD patients while exercising [57, 88, 89]. On the other hand, clinical significance of potential respiratory muscle impairment is debated. Diaphragmatic dysfunction can be encountered in advanced stages, but peripheral muscle weakness often seems to prevail [90]. Increased work of breathing and ventilatory inefficiency are thought to equate to chronic loading of respiratory muscles, which could preserve their function. All in all, the precise mechanisms of SMD in ILDs are still poorly understood. Several factors are suspected to participate: physical inactivity, ageing, malnutrition, arterial hypoxaemia resulting in tissue hypoxia, systemic inflammatory and oxidative stress, steroid myopathy, and/or direct insult by systemic disease [91, 92].
Diagnostic utility of ventilatory efficiency in ILDs
Assessment of functional impairment (the example of sarcoidosis)
CPET may be useful to detect precocious functional impact in the context of ILD. Exercise limitation, as defined by peak V˙O2<84% of predicted value, affects 50–88% of sarcoidosis patients taken as a whole [93, 94]. But even those with still normal resting PFTs can harbour reduced peak V˙O2 [44, 45] or ventilatory inefficiency with abnormally increased V˙E/V˙CO2 [95]. In a US prospective study that included 39 patients with biopsy-proven sarcoidosis, Athos et al. [96] reported that disease staging by chest radiography was the best overall predictor of exercise performance. However, several other studies failed to find a correlation between disease staging and peak V˙O2 [95, 97, 98]. Along the same lines, although ventilatory inefficiency seems to be a sensitive marker of early functional impairment in sarcoidosis, no correlation was found in these studies between disease staging and V˙E/V˙CO2, measured at VTh or at peak exercise [95–98]. One possible explanation is that organs other than lungs can be involved in sarcoidosis and alter the ventilatory response to exercise. Still, Magrì et al. [99] found that the V˙E–V˙CO2 slope was negatively correlated with resting DLCO (r=−0.85; p<0.001) and positively correlated with the change in arterial O2 saturation (ΔSaO2) between rest and peak exercise (r=0.68; p<0.001) in 30 patients with stage 2–4 sarcoidosis. In the work by Miller et al. [95], 78% of sarcoidosis patients with altered DLCO had an abnormally elevated V˙E/V˙CO2>34 at VTh (mean: 45±9) versus only 38% of those with normal DLCO. Finally, in a more recent monocentric prospective work with 83 sarcoidosis patients, Kallianos et al. [100] found that V˙E/V˙CO2 at VTh progressively increased from stage 1 to stage 4 groups. Interestingly, a principal component analysis showed that elevated V˙E/V˙CO2, peak V˙E/V˙O2 and VD/VT, all markers of inappropriate ventilatory response to exercise, were correlated with radiographic stage and with the presence of extrapulmonary locations. One limit of this study, however, was that it included only nine patients with stage 4 sarcoidosis.
Discrimination between IIPs
As shown in table 1 and figure 4, an increased V˙E/V˙CO2 ratio is a hallmark of many cardiopulmonary conditions. Thus, it is not sufficient alone to discriminate between ILD and a differential diagnosis, but the global pattern of exercise response must be taken into account [5, 9]. Yet, in a Canadian cross-sectional study comparing 16 patients with mild-to-moderate ILD (mean VC: 73±12% of predicted value; mean TLC: 64±10%; mean DLCO: 44±12%) to 16 sex- and age-matched patients with mild-to-moderate COPD (mean FEV1: 63±22%; mean DLCO: 62±22%) and 16 healthy subjects, Faisal et al. [67] found that ventilatory inefficiency was significantly greater in ILD patients than in COPD patients, and even greater than in controls: 33±5 versus 31±4 and 27±3 for V˙E/V˙CO2 nadir, respectively (p<0.05). These results were identical regardless of the calculation method (V˙E/V˙CO2 at rest, V˙E-V˙CO2 slope, peak V˙E/V˙CO2). Nevertheless, Kisaka et al. [101] found no difference between eight ILD patients and nine COPD patients when measuring V˙E/V˙CO2 at VTh: 36±5 versus 37±8, as compared to 27±3 in nine healthy controls. Six patients with pulmonary vasculopathy were also enrolled and they harboured the greatest V˙E/V˙CO2 at VTh (43±5).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Examples of ventilatory efficiency slope (V˙E–V˙CO2 slope) in a healthy subject presenting with a peak oxygen uptake (V˙O2) of 38 ml·min−1·kg−1 (black line and rhomboid), a patient with pulmonary sarcoidosis presenting with a peak V˙O2 of 19 ml·min−1·kg−1 (violet line and circles), a patient with pulmonary arterial hypertension (PAH) presenting with a peak V˙O2 of 18 ml·min−1·kg−1 (red line and triangles) and a patient with idiopathic pulmonary fibrosis (IPF) presenting with a peak V˙O2 of 19 ml·kg−1·min−1 (blue line and squares).
Given the particular sensitivity of CPET, Hagmeyer et al. [102] hypothesised that it could perhaps help to distinguish between two IIPs in the early course of the disease. In a prospective monocentric study, they compared exercise variables of 27 mild-to-moderate untreated IIPs, divided into two groups: 14 patients with IPF and 13 with iNSIP. They reported a significantly lower mean peak V˙O2 in IPF patients (74±31% versus 99±15%; p=0.01) and a significantly higher mean V˙E/V˙CO2 at any given level of O2 consumption (e.g. 50±14 versus 38±6 at VTh; p=0.01). Nonetheless, one should remain cautious before integrating these findings into a diagnostic tree of IIPs. In fact, mean forced VC (FVC) was lower in IPFs (65±12% versus 80±23%), suggesting a more important alteration of lung compliance in this group, but no indication was given about fR, although V˙E/V˙CO2 at VTh is presumably correlated with fR at peak exercise in IIPs [103]. IPF patients also tended to exhibit a wider mean peak P(A-a)O2 (65±11 mmHg versus 55±14 mmHg), which could have participated in an accelerated fR. Lastly, mean DLCO tended to be lower in IPFs (52±22% versus 62±16%), especially since V˙E/V˙CO2 values differed amongst DLCO quartiles; this difference could have accounted in part for a pulmonary vascular involvement that was not evaluated.
Early detection of pneumoconiosis in patients at risk
The assessment of ventilatory efficiency could play a role in monitoring patients exposed to inhaled mineral dust. Duvenkamp et al. [104] compared 20 former coal miners with anthracosilicosis to 24 healthy volunteers and showed that mean V˙E/V˙CO2 at a submaximal WR of 50 watts was abnormally elevated in patients (39±5 versus 31±4; p<0.0001) and was not correlated with the radiological grading of the disease. In a later French study of 38 patients with mild-to-moderate anthracosilicosis, all complaining of dyspnoea and divided into four groups in accordance with resting PFTs, Favre et al. [105] found a ventilatory inefficiency across all groups, including 21 patients with normal resting PFTs (mean peak V˙E/V˙CO2 in the normal PFT group: 39±8). Peak V˙E/V˙CO2 was negatively correlated with DLCO and positively correlated with ΔSaO2. One proposed reason why CPET was more sensitive than PFTs was that cardiac limitation (mixed or isolated) was involved in 12 (31%) of the patients having completed maximal exercise. In some coal miners, ventilatory inefficiency could also reveal the presence of small airway dysfunction [106]. Somewhat analogous observations were made with asbestosis: one German study compared 19 patients with former occupational asbestos exposure and variable resting PFTs to 24 healthy subjects; mean V˙E/V˙CO2 was higher in patients than in controls, but no correlation was found between ventilatory insufficiency and radiological severity of the disease [107].
Non-invasive diagnosis of coexisting PH
More importantly, patients with ILD are at high risk of developing PH. Guidelines have proposed risk stratification based on CPET variables, including peak V˙O2, V˙E/V˙CO2 and end-tidal CO2 partial pressure (PETCO2), to evaluate patients with suspected PAH, either idiopathic or CTD-related. ILD patients with disproportionate V˙E/V˙CO2 must be suspected of pulmonary vasculopathy as well: in the context of ILD, PH may worsen pulmonary gas exchange and exacerbate the already exaggerated ventilatory response to exercise [15, 108, 109]. Specifically, in IPF patients, at least four studies, including two with prospective designs, have shown that V˙E/V˙CO2 was the best functional variable able to predict the coexistence of PH [110–113]. In another retrospective monocentric series of lung transplant candidates with various severe ILDs (almost half of them non-IPF), peak V˙E/V˙CO2, PETCO2 and resting DLCO were significantly associated with PH [114]. Ventilatory inefficiency was also assessed in a Brazilian prospective monocentric study of 32 PLCH patients with subsequent CPET and right heart catheterisation (RHC). The 13 (41%) patients with coexisting PH showed worse resting PFTs (FEV1, DLCO) and tended to have a greater V˙E–V˙CO2 slope (38±15 versus 30±5; p=0.07), but this last result was not statistically significant because of the small population size and large inter-subject variability [74]. In a prospective monocentric study with 27 mild-to-moderate ILDs (mean FVC: 68±3%; mean DLCO: 45±5%), amongst which 14 (52%) were IPFs, Degani-Costa et al. [115] performed invasive haemodynamic measurements during exercise to explore pulmonary vascular dysfunction (PVD), defined in accordance with the ratio between mean pulmonary artery pressure and cardiac output (mPAP– Q̇ C slope). Although only seven patients had PH with elevated mPAP≥25 mmHg at rest, PVD during exercise was identified in 15, harbouring higher V˙E/V˙CO2 at VTh than patients without PVD (45±2 versus 38±1; p=0.015), and higher peak VD/VT (39±2 versus 30±2; p=0.008).
In the particular case of systemic sclerosis (SSc), PAH may occur even without associated ILD. In SSc patients without respiratory limitation at exercise (normal BR at peak V˙O2), high V˙E/V˙CO2 (at VTh or at maximal exercise) and decreasing PETCO2 from start of exercise to VTh were said to discriminate pulmonary vasculopathy from left ventricular dysfunction [116, 117]. In the US prospective series from Dumitrescu et al. [116], which included 28 SSc patients with echocardiographic systolic pulmonary artery pressure (sPAP)≤35 mmHg, an early pulmonary vasculopathy profile was identified in eight (62%) out of the 13 patients with ILD on HRCT (ILD-SSc). Nevertheless, these studies chose to solely characterize the predominant mechanism of exercise limitation for each patient. On the other side, a French retrospective multicentric study by Martis et al. [118], with 27 SSc patients having performed CPET, revealed that a combination of putative mechanisms was involved in 19 cases (70%). CPET found an ILD pattern in 16 patients (60%), which was 78% concordant with HRCT observations. Among the 10 patients referred for RHC, CPET variables indicating a pulmonary vasculopathy were more concordant with RHC than with TTE. Indeed, a good correlation between RHC and CPET variables, including V˙E/V˙CO2, was previously described in SSc [119]. In combination with the DETECT screening algorithm (associating PFTs, biological markers and TTE in SSc patients with DLCO<60% and a disease duration>3 years) [120], a V˙E-V˙CO2 slope>36 was suggested to be able to diminish the need for RHC referral, given its excellent sensitivity and negative predictive value. However, this threshold must be confirmed for ILD-SSc patients, since this Italian prospective multicentric cohort with 96 SSc patients included only seven with mild-to-intermediate lung fibrosis on HRCT [121].
The presence of coexisting PH in a patient with ILD and/or SSc is of high prognostic significance, and ventilatory inefficiency has been shown to be associated with worse outcomes in various configurations.
Prognostic implications of ventilatory inefficiency in ILDs
Many correlations were uncovered in the literature between survival and CPET variables, indicating that exercise limitation has a tremendous effect on ILD patients. In a US monocentric study that retrospectively analysed 117 patients with newly diagnosed IPF, Fell et al. [122] were the first to report that baseline peak V˙O2<8.3 ml·kg−1·min−1 was independently associated with a threefold increase in mortality. This association was later confirmed in a German multicentric cohort (retrospective analysis of prospectively collected data), with 135 IPF patients having performed PFTs, CPET and RHC, in which peak V˙O2 was the only functional variable independently predictive of transplant-free survival. Yet, the most powerful prognosticator was the presence of PH. V˙E/V˙CO2 was tightly associated with PH (area under receiver operating characteristic curve: 0.94 (0.89−0.98)), thus it was not retained as an independent marker of mortality in multivariate analysis [112]. Several other studies with retrospective designs concerning IPF patients [123–125] or lung transplantation candidates with various ILDs [126, 127] showed that V˙E/V˙CO2 was a mortality predictor at 1 or 3 years in univariate analysis, but not in final multivariate models. In a Japanese study of 41 IPF patients by Miki et al. [123] (mean VC: 69±19%; mean DLCO: 44±15%; mean peak V˙E/V˙CO2: 52±13), peak V˙E/V˙CO2 was the CPET variable most closely correlated with peak V˙O2 (r=−0.7; p<0.0001), and was also correlated with PaO2 slope, which was itself independently associated with mortality. Interestingly, in the work of Wallaert et al. [124] with 63 IPF patients, among the numerous functional prognostic markers identified in univariate analysis, TLC<65% and V˙E/V˙O2 at VTh>45 were independently predictive of 3-year transplant-free survival, that is to say another CPET variable very similar to V˙E/V˙CO2.
Finally, V˙E/V˙CO2 was found to be independently associated with mortality in two prospective monocentric series. The first one included 25 treatment-naive patients with mild-to-moderate IPF (mean FVC: 78±22%; mean DLCO: 46±15%; mean V˙E-V˙CO2 slope: 40±14) and slight-to-moderately severe dyspnoea. V˙E–V˙CO2 slope (hazard ratio: 1.09 (1.04−1.15)) and peak V˙O2 (hazard ratio: 0.75 (0.6−0.95)) were the most potent predictors of survival [128]. Interestingly, V˙E–V˙CO2 slope was the CPET variable best correlated with dyspnoea on the modified Medical Research Council (mMRC) scale (r=0.73; p<0.001) [89], whereas the mMRC scale had previously been showed to independently predict mortality [129, 130]. In the second series, Vainshelboim et al. [38, 131] included 38 stable, but not incident, IPFs (median FVC: 68 (37−109); median DLCO: 50 (23−91); median V˙E–V˙CO2 slope: 43 (39−49)). Patients were subsequently randomised into two groups to assess the effects of a supervised 12-week exercise training program. As there was no difference in transplant-free survival at 40 months between both exercise training and control groups, patients were all analysed together for other prognostic factors. V˙E/V˙CO2 at VTh>34, V˙E/V˙O2 nadir>34, peak V˙O2≤13.8 mL·kg−1·min−1, VT reserve≤0.48 L·breath−1 and peak WR<62 watts were associated with increased mortality or lung transplantation [131]. Exercise training significantly improved peak V˙O2 and V˙O2 at VTh, but not peak V˙E/V˙CO2 [86]. This lack of effect of exercise training on V˙E/ V˙CO2 was also observed in another study with 21 worsening IPFs [132].
It is not very surprising that V˙E/V˙CO2 seems to represent a reliable prognostic factor in ILDs, since it reflects the potential convergence of several pathophysiological mechanisms involved in disease progression and ultimately prognosis. Indeed, excessive hyperventilation at exercise may result from dynamic mechanical constraints secondary to lung restriction, exercise-induced hypoxaemia, pulmonary vasculopathy with increased VD and other poorly understood peripheral factors. Incidentally, one weakness of some of the aforementioned studies is that pulmonary vasculopathy was not always assessed. A recent literature systematic review identified other confounding factors, including methodological heterogeneity and selective reporting bias [133]. Another limitation is that “baseline” CPET was actually often performed at different stages of the disease, since not only newly diagnosed ILDs were included. Moreover, very few studies have investigated the value of longitudinal data from subsequent CPETs.
Several studies have explored the links between PH, exercise limitation and prognosis in ILDs. In these patients, associated PH was demonstrated to significantly impair maximal aerobic capacity [74, 110, 112–114], sometimes only when PH was classified as severe [111]. Additionally, V˙E/V˙CO2 was found to correlate with dyspnoea during CPET (Borg scale) [110] and with PH severity, as assessed by sPAP measured by TTE, with correlation coefficients varying from 0.61 to 0.87 [110, 111, 113]. In another series, peak V˙E/V˙CO2 and peak PETCO2 were the two variables best correlated with mPAP measured during RHC [114, 134]. In the monocentric work of van der Plas et al. [113], in which 38 prospectively enrolled IPF patients performed CPET and TTE, the optimal cut-off value for predicting a resting sPAP≥40 mmHg was a V˙E/V˙CO2 at VTh>45. This cut-off value also proved to be a good prognosis marker, since mean survival was 81.3±14.1 months in the 24 patients with V˙E/V˙CO2 at VTh≤45 versus 21±4.9 months in the 14 patients with V˙E/V˙CO2 at VTh>45 (p=0.001). Conversely, it is of note that the cut-off value of 40 mmHg for resting sPAP was not able to identify two groups with different prognosis (n=27 for sPAP<40 mmHg and n=11 for sPAP≥40 mmHg) [113].
Concerning SSc, an important German multicentric study by Ewert et al. [135] retrospectively analysed the outcome of 210 patients having performed CPET. Amongst them, 74 (35%) had ILD on HRCT, rated as ILD limited to less than 20% of lung surface for 42 (20%) or extensive ILD for 32 (15%). Simultaneously, RHC was performed in 139 (66%), leading to a diagnosis of PAH in 52 (25%). In multivariate analysis, V˙E–V˙CO2 slope (hazard ratio: 0.9 (0.83–0.98)) and peak V˙O2 (hazard ratio: 0.87 (0.81–0.94)) were significant predictive factors of long-term survival (median follow-up: 7.7 years), alongside age, FVC and Krogh factor (KCO, i.e. DLCO per alveolar volume). Optimal cut-off values with the highest discriminative power were 35 for V˙E–V˙CO2 slope and 64.5% of predicted value for peak V˙O2 [135]. In another recent Italian monocentric study, Rosato et al. [136] prospectively included 45 SSc patients who subsequently performed baseline CPET, PFTs, TTE and HRCT (median lung surface with HRCT pattern of ILD on CALIPER analysis: 9.8% (7.3−16.1); median FVC: 102% (89−109); median DLCO: 77% (71−81); median V˙E–V˙CO2 slope: 29 (28−32)). Then, PFTs and TTE were annually repeated during the 5-year follow-up. The study population was divided into two groups: 37 (82%) with normal V˙E-V˙CO2 slope at baseline and eight (18%) with baseline ventilatory inefficiency as defined by V˙E–V˙CO2 slope≥35. Baseline ventilatory inefficiency was a marker of ILD progression and pulmonary vasculopathy, with a greater decline of FVC (9.6% (0.5−12.2) versus 2.4% (0.4−5.0); p<0.05) and DLCO (9.2% (6.4−16.6) versus 2.3% (0.5−5.2); p<0.01), and a greater raise in sPAP (7.8 mmHg (5.2−14.2) versus −1.5 mmHg (−1-−3); p<0.0001) during follow-up. Moreover, in multivariate analysis, V˙E–V˙CO2 slope was independently associated with the onset of a new major vascular complication, namely digital ulcers, PAH and sclerodermal renal crisis (hazard ratio: 1.09 (1.02−1.2)). Lastly, V˙E–V˙CO2 slope was the only significant independent prognostic factor of mortality from ILD at 5 years (hazard ratio: 1.27 (1.003−1.6)) and a V˙E–V˙CO2 slope≥35 was a prognostic factor of all-cause mortality at 5 years [136]. The same team had previously showed that, in SSc patients without obvious cardiopulmonary involvement, V˙E–V˙CO2 slope was a marker of vascular kidney damage [137] and was significantly correlated with global disease activity and severity, as assessed by Disease Activity Index and Disease Severity Index (r=0.59 and 0.73, respectively; both p<0.0001) [138]
Conclusion
ILDs are a devastating category of diseases, which can carry a poor prognosis in cases of progressive fibrosing pattern and/or associated PH. Exercise intolerance and exertional dyspnoea are key symptoms that contribute to curtailing and then avoiding physical activity, resulting in progressive deconditioning. The mechanisms of exercise intolerance in ILD patients are due to a combination of factors including altered pulmonary gas exchange, anomalies in pulmonary mechanics and cardiovascular function, as well as SMD. CPET can be a valuable tool to not only assist in diagnosis, determine the presence of comorbidities, objectively evaluate functional capacity, determine symptom severity, accurately prescribe exercise training and monitor disease progression or therapeutic response, but also generate valuable prognostic information and optimise the management of patients with ILD. Evidence concerning the clinical utility of ventilatory efficiency as a prognostic indicator in ILD is rapidly emerging and therefore promising.
Footnotes
Provenance: Commissioned article, peer reviewed.
Number 11 in the Series “Ventilatory efficiency and its clinical prognostic value in cardiorespiratory disorders” Edited by Pierantonio Laveneziana and Paolo Palange
Previous articles in this series: No. 1: Laveneziana P, Di Paolo M, Palange P. The clinical value of cardiopulmonary exercise testing in the modern era. Eur Respir Rev 2021; 30: 200187. No. 2: Agnostoni P, Sciomer S, Palermo P, et al. Minute ventilation/carbon dioxide production in chronic heart failure. Eur Respir Rev 2021; 30: 200141. No. 3: Watson M, Ionescu MF, Sylvester K, et al. Minute ventilation/carbon dioxide production in patients with dysfunctional breathing. Eur Respir Rev 2021; 30: 200182. No. 4: Ward SA. Ventilation/carbon dioxide output relationships during exercise in health. Eur Respir Rev 2021; 30: 200160. No. 5: Collins SÉ, Phillips DB, Brotto AR, et al. Ventilatory efficiency in athletes, asthma and obesity. Eur Respir Rev 2021; 30: 200206. No. 6: Schaegger MR, Guenette JA, Jensen D. Impact of ageing and pregnancy on the minute ventilation/carbon dioxide production response to exercise. Eur Respir Rev 2021; 30: 200225. No. 7: Weatherald J, Philipenko B, Montani D, et al. Ventilatory efficiency in pulmonary vascular diseases. Eur Respir Rev 2021; 30: 200214. No. 8: Neder JA, Berton DC, Phillips DB, et al. Exertional ventilation/carbon dioxide output relationship in COPD: from physiological mechanisms to clinical applications. Eur Respir Rev 2021; 30: 200190. No. 9: Hager A. Minute ventilation/carbon dioxide production in congenital heart disease. Eur Respir Rev 2021; 30: 200178. No. 10: Laveneziana P, Palange P. Ventilatory efficiency and its clinical and prognostic value in adults with cystic fibrosis. Eur Respir Rev 2021; 30: 200395.
Conflict of interest: T. Gille reports personal fees from Boehringer Ingelheim and Roche, and other funding from Oxyvie (oxygen provider), LVL Medical (oxygen provider) and VITALAIRE (oxygen provider), outside the submitted work.
Conflict of interest: P. Laveneziana reports personal fees from Novartis France, Chiesi France and Boehringer France, outside the submitted work.
- Received November 3, 2020.
- Accepted May 26, 2021.
- Copyright ©The authors 2021
This version is distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0. For commercial reproduction rights and permissions contact permissions{at}ersnet.org
References










